
Exhibit 99.1
Exhibit 99.1
2 Safe Harbor Statements Forward-Looking Statements Certain statements contained in this presentation are or may be considered "forward-looking statements" as defined in the Private Securities Litigation Reform Act of 1995. These statements can be identified by the fact that they do not relate strictly to historic or current facts. They use words such as "estimate," "expect," "intend," "believe," "plan," "anticipate," "potential," "projected" and other words and terms of similar meaning in connection with any discussion of future operating or financial performance or condition. Jasper Therapeutics, Inc. ("Jasper") cautions that these statements are based upon the current beliefs and expectations of Jasper's management and are subject to significant risks, uncertainties and assumptions, including, without limitation, risks related to the market price of Jasper's common stock relative to the value suggested by the exchange ratio in connection with Jasper's acquisition of Kira Pharmaceuticals ("Kira" and together with Jasper, the "Combined Company" pursuant to a merger); unexpected costs, charges or expenses resulting from the merger; potential adverse reactions or changes to business relationships resulting from the announcement or completion of the merger; the uncertainties associated with the Combined Company's product candidates, as well as risks associated with the clinical development and regulatory approval of product candidates, including potential delays in the commencement, enrollment and completion of clinical trials; risks related to the inability of the Combined Company to obtain sufficient additional capital to continue to advance these product candidates and its preclinical programs; uncertainties in obtaining successful clinical results for product candidates and unexpected costs that may result therefrom; risks related to the failure to realize any value from product candidates and preclinical programs being developed and anticipated to be developed in light of inherent risks and difficulties involved in successfully bringing product candidates to market; risks associated with the possible failure to realize certain anticipated benefits of the merger, including with respect to future financial and operating results; the risk that the private placement is not consummated; the possibility that holders of CVRs may never receive any proceeds; risks related to the possibility that Jasper's shareholders may not approve the conversion of the Preferred Stock, and such additional risks and uncertainties contained in the "Risk Factors" section of Jasper's Annual Reports on Form 10-K for the year ended December 31, 2025, Quarterly Reports on Form 10-Q and Current Reports on Form 8-K that Jasper has subsequently filed or may subsequently file with the SEC. Statements regarding future actions, future performance and/or future results including, without limitation, those relating to the timing for completion, and results of, scheduled or additional clinical trials and the FDA's or other regulatory review and/or approval and commercial launch and sales results (if any) of the Combined Company's formulations and product candidates and regulatory filings related to the same, financial projections and targets, business strategy, plans and objectives for future operations, statements regarding the Combined Company and its operations and prospects, may not occur, and actual results could differ materially and adversely from those anticipated or implied in the forward-looking statements. In light of these risks, uncertainties and assumptions, the forward-looking events and circumstances discussed in this press release are inherently uncertain and may not occur, and actual results could differ materially and adversely from those anticipated or implied in the forward-looking statements. Accordingly, you should not rely upon forward-looking statements as predictions of future events. There is no obligation to update publicly or revise any forward-looking statements for any reason after the date of this presentation or to conform these statements to actual results or to changes in the Combined Company's expectations, whether as a result of new information, future events, inaccuracies that become apparent after the date hereof or otherwise, except as may be required under applicable securities laws. Industry and Market Data: Certain data in this presentation was obtained from various external sources, and neither Jasper nor its affiliates, advisers or representatives has verified such data with independent sources. Accordingly, neither Jasper nor any of its affiliates, advisers or representatives makes any representations as to the accuracy or completeness of that data or undertakes any obligation to update such data after the date of this presentation. Such data involves risks and uncertainties and is subject to change based on various factors. Trademarks: The trademarks included herein are the property of the owners thereof and are used for reference purposes only. Such use should not be construed as an endorsement of the products or services of Jasper.
3 Merger • On July 16, 2026, Kira Pharmaceuticals ("Kira") and Jasper Therapeutics, Inc. (NASDAQ: JSPR) entered into a merger agreement whereby Jasper acquired all outstanding shares of Kira in in an all-stock transaction, and concurrently raised $132 million in a PIPE offering • On a fully diluted basis, assuming exercise of all outstanding equity instruments and conversion of all preferred stock issued in connection with the merger and the PIPE offering: • Equityholders of Jasper immediately prior to the transaction will own approximately 6.68% of Jasper's common stock, • Equityholders of Kira immediately prior to the acquisition will own approximately 49.86% of Jasper's common stock, and • Investors in the private placement financing will own approximately 43.46% of Jasper's common stock • The total number of shares of Jasper common stock outstanding would be approximately 653.6 million (on an as-converted-to- common basis) • In connection with the acquisition of Kira, each holder of Jasper common stock as of immediately before the closing of the transaction will receive a non-transferrable contingent value right ("CVR") entitling holders to receive an aggregate $30 million in payments related to Jasper obtaining a priority review voucher ("PRV") for briquilimab by the end of 2028. Payments under the CVR shall only be due upon the monetization of the CVR or in the event of an acquisition of the Combined Company. Concurrent PIPE • Concurrent with the merger, Jasper entered into a securities purchase agreement pursuant to which Jasper agreed to sell approximately 4.7 million shares of preferred stock for an aggregate purchase price of approximately $132M Use of proceeds focused on key value drivers: • KP 104 - Research and development of Ph. 2, interim Stage 1 and Stage 2 data in rare renal disorders, • KP-104 Ph. 3 initiation in PNH • Briquilimab pre-BLA meeting in SCID • KP-701 Ph. 1b data / Ph. 2 initiation in B-cell mediated diseases • General corporate expenses and working capital needs Strong balance sheet expected to fund multiple anticipated clinical milestones and operating plan through 2H 2028 Out-License • Kira has out-licensed KP-301, a preclinical long-acting anti-C5a monoclonal antibody, and KP-402, a small molecule C5a receptor antagonist, to Mirador Therapeutics • The out-licensing transaction will provide an upfront payment of $12M, and potential development and sales milestone payments Merger creates a combined company with deep expertise in antibody drug development and immunologically- driven disorders Overview of the Merger Transaction and Financing

4 Jasper Executive Team Experienced drug developers focused on driving value Wenru Song, MD, PhD Executive Vice President and Head of R&D Ex-VP level clinical positions at large pharma companies Greg Keenan, MD Chief Medical Officer Rheumatologist, antibody drug developer & former CMO at publicly traded biotechs Matthew Ros Chief Operating Officer Former COO / CFO and Board member at publicly traded pharma companies Jeet Mahal Chief Executive Officer Biotech executive and Board member with 30+ years of experience in development & commercialization Patrick Crutcher, MSc Board of Directors, Chairman, Kira Pharmaceuticals Herb Cross Chief Financial Officer Biotech executive with extensive experience in leadership roles at publicly traded biotech companies
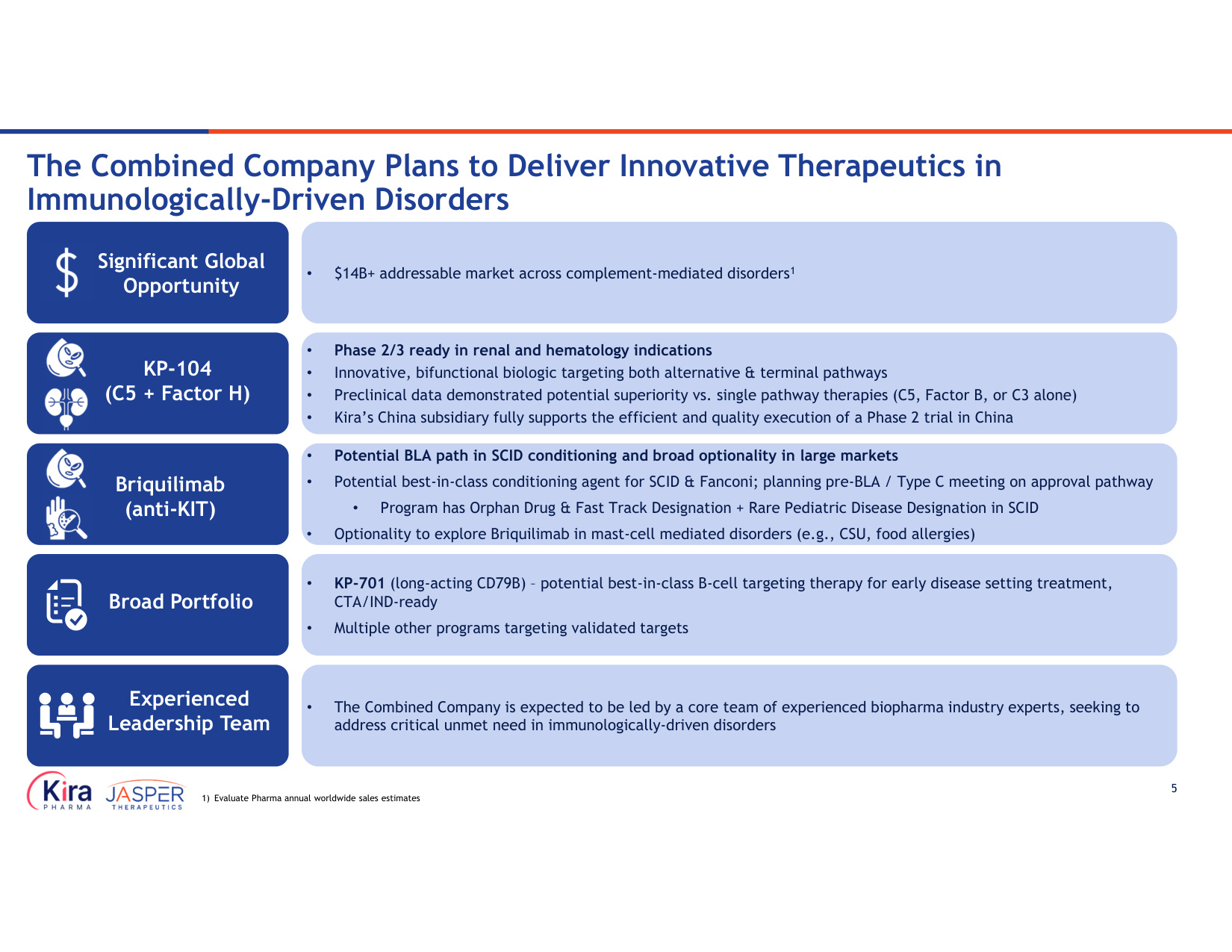
5 • $14B+ addressable market across complement-mediated disorders1 • Phase 2/3 ready in renal and hematology indications • Innovative, bifunctional biologic targeting both alternative & terminal pathways • Preclinical data demonstrated potential superiority vs. single pathway therapies (C5, Factor B, or C3 alone) • Kira's China subsidiary fully supports the efficient and quality execution of a Phase 2 trial in China • Potential BLA path in SCID conditioning and broad optionality in large markets • Potential best-in-class conditioning agent for SCID & Fanconi; planning pre-BLA / Type C meeting on approval pathway • Program has Orphan Drug & Fast Track Designation + Rare Pediatric Disease Designation in SCID • Optionality to explore Briquilimab in mast-cell mediated disorders (e.g., CSU, food allergies) • The Combined Company is expected to be led by a core team of experienced biopharma industry experts, seeking to address critical unmet need in immunologically-driven disorders • KP-701 (long-acting CD79B) – potential best-in-class B-cell targeting therapy for early disease setting treatment, CTA/IND-ready • Multiple other programs targeting validated targets The Combined Company Plans to Deliver Innovative Therapeutics in Immunologically-Driven Disorders 1) Evaluate Pharma annual worldwide sales estimates Significant Global Opportunity KP-104 (C5 + Factor H) Briquilimab (anti-KIT) Broad Portfolio Experienced Leadership Team
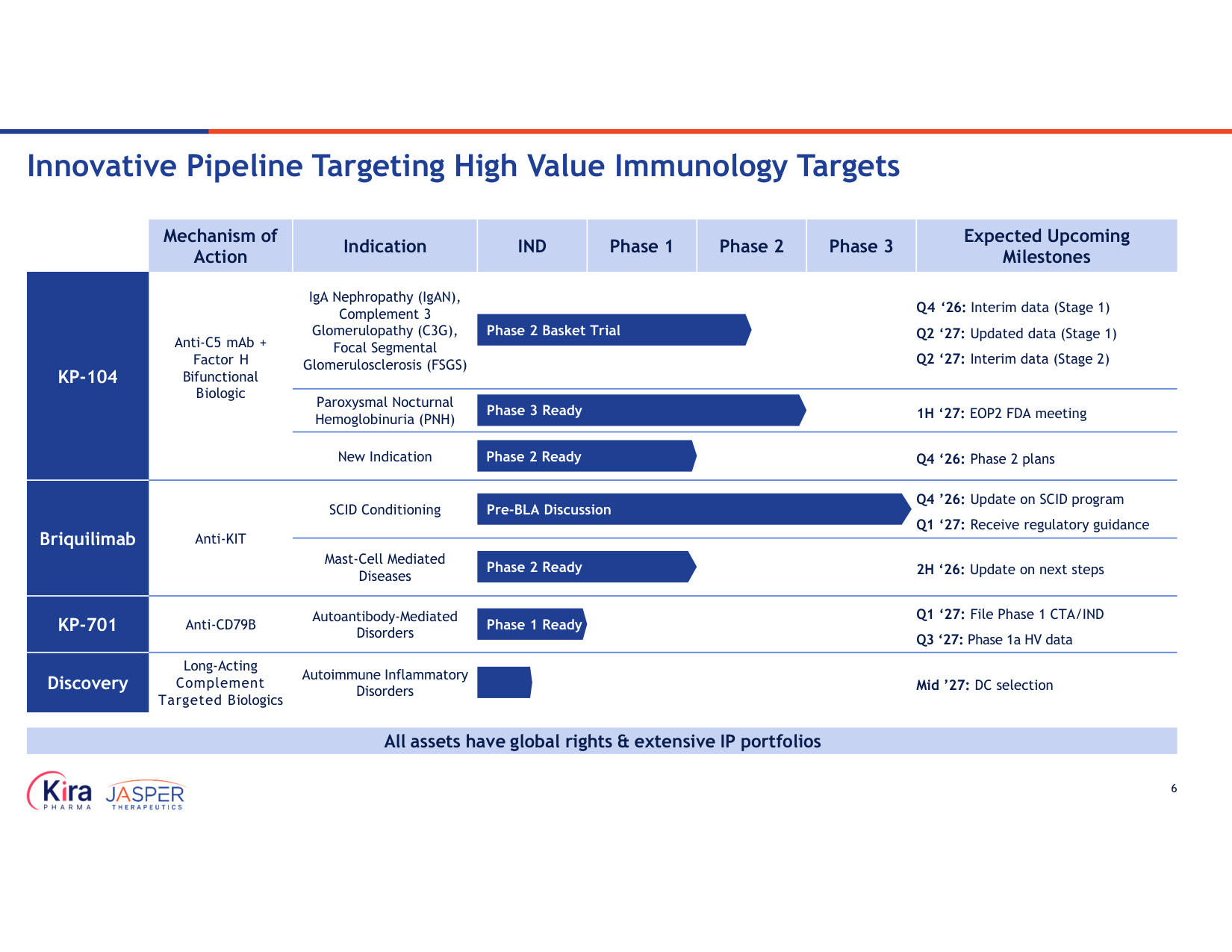
6 Expected Upcoming Milestones Phase 3 Phase 2 Phase 1 IND Indication Mechanism of Action Q4 '26: Interim data (Stage 1) Q2 '27: Updated data (Stage 1) Q2 '27: Interim data (Stage 2) IgA Nephropathy (IgAN), Complement 3 Glomerulopathy (C3G), Focal Segmental Glomerulosclerosis (FSGS) Anti-C5 mAb + Factor H Bifunctional Biologic KP-104 1H '27: EOP2 FDA meeting Paroxysmal Nocturnal Hemoglobinuria (PNH) Q4 '26: Phase 2 plans New Indication Q4 '26: Update on SCID program Q1 '27: Receive regulatory guidance SCID Conditioning Anti-KIT Briquilimab 2H '26: Update on next steps Mast-Cell Mediated Diseases Q1 '27: File Phase 1 CTA/IND Q3 '27: Phase 1a HV data Autoantibody-Mediated Disorders Anti-CD79B KP-701 Mid '27: DC selection Autoimmune Inflammatory Disorders Long-Acting Complement Targeted Biologics Discovery Phase 2 Basket Trial Phase 2 Ready Phase 3 Ready Phase 2 Ready All assets have global rights & extensive IP portfolios Pre-BLA Discussion Innovative Pipeline Targeting High Value Immunology Targets Phase 1 Ready
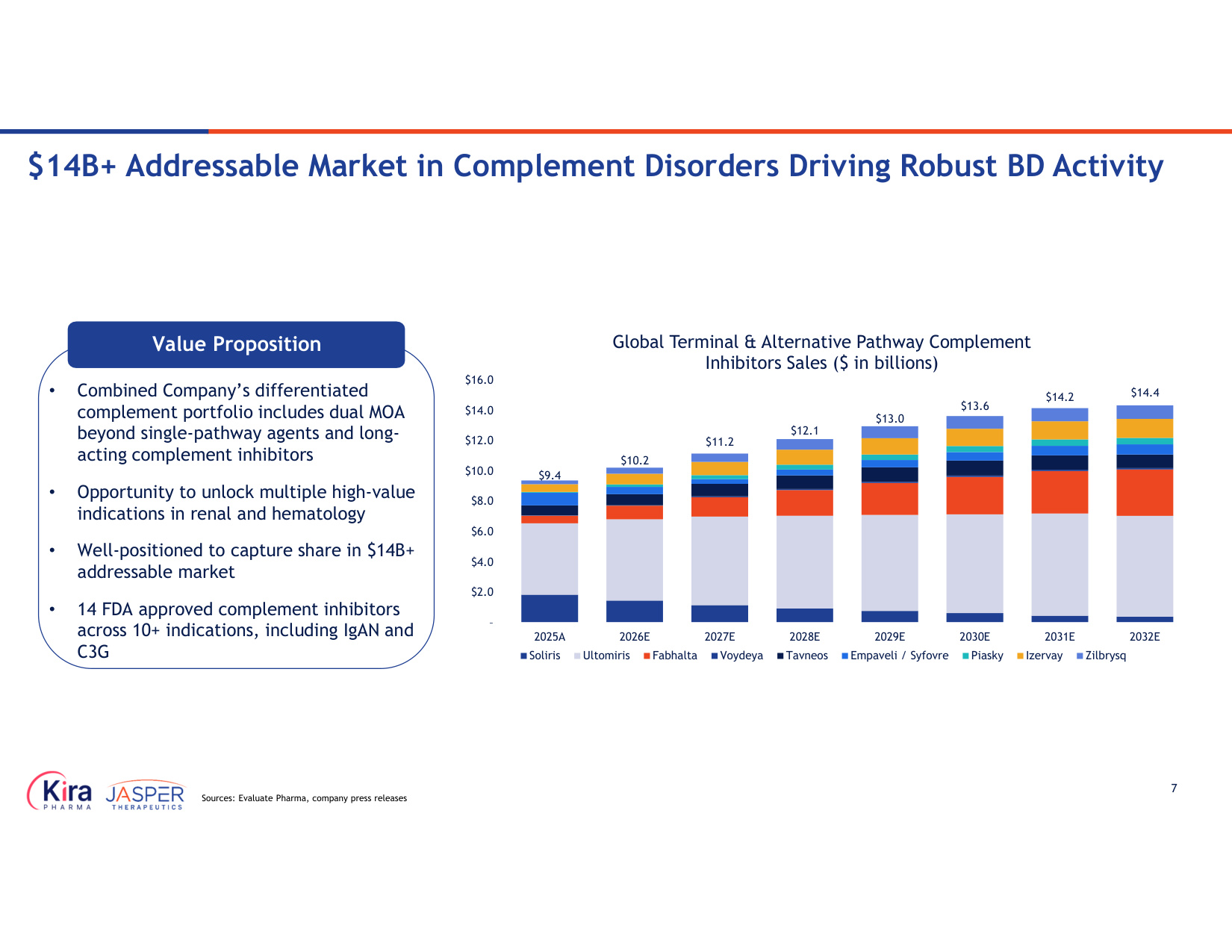
7 $9.4 $10.2 $11.2 $12.1 $13.0 $13.6 $14.2 $14.4 – $2.0 $4.0 $6.0 $8.0 $10.0 $12.0 $14.0 $16.0 2025A 2026E 2027E 2028E 2029E 2030E 2031E 2032E Global Terminal & Alternative Pathway Complement Inhibitors Sales ($ in billions) Soliris Ultomiris Fabhalta Voydeya Tavneos Empaveli / Syfovre Piasky Izervay Zilbrysq Value Proposition • Combined Company's differentiated complement portfolio includes dual MOA beyond single-pathway agents and long- acting complement inhibitors • Opportunity to unlock multiple high-value indications in renal and hematology • Well-positioned to capture share in $14B+ addressable market • 14 FDA approved complement inhibitors across 10+ indications, including IgAN and C3G Source: IQVIA $14B+ Addressable Market in Complement Disorders Driving Robust BD Activity Sources: Evaluate Pharma, company press releases
KP-104 (Vensobafusp alfa) Anti-C5 mAb + Factor H Bifunctional Biologic
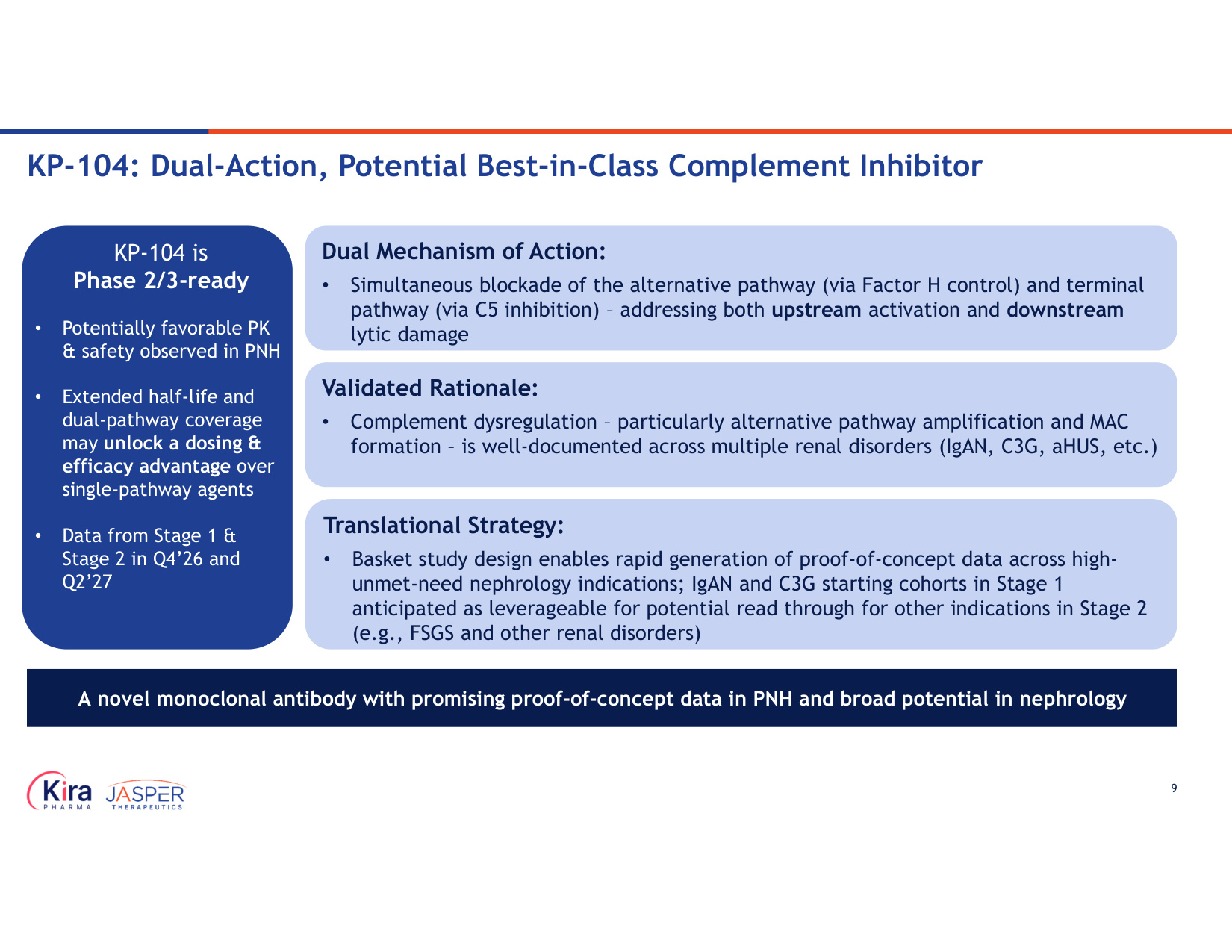
9 KP-104: Dual-Action, Potential Best-in-Class Complement Inhibitor Validated Rationale: • Complement dysregulation – particularly alternative pathway amplification and MAC formation – is well-documented across multiple renal disorders (IgAN, C3G, aHUS, etc.) Dual Mechanism of Action: • Simultaneous blockade of the alternative pathway (via Factor H control) and terminal pathway (via C5 inhibition) – addressing both upstream activation and downstream lytic damage A novel monoclonal antibody with promising proof-of-concept data in PNH and broad potential in nephrology Translational Strategy: • Basket study design enables rapid generation of proof-of-concept data across high- unmet-need nephrology indications; IgAN and C3G starting cohorts in Stage 1 anticipated as leverageable for potential read through for other indications in Stage 2 (e.g., FSGS and other renal disorders) KP-104 is Phase 2/3-ready • Potentially favorable PK & safety observed in PNH • Extended half-life and dual-pathway coverage may unlock a dosing & efficacy advantage over single-pathway agents • Data from Stage 1 & Stage 2 in Q4'26 and Q2'27
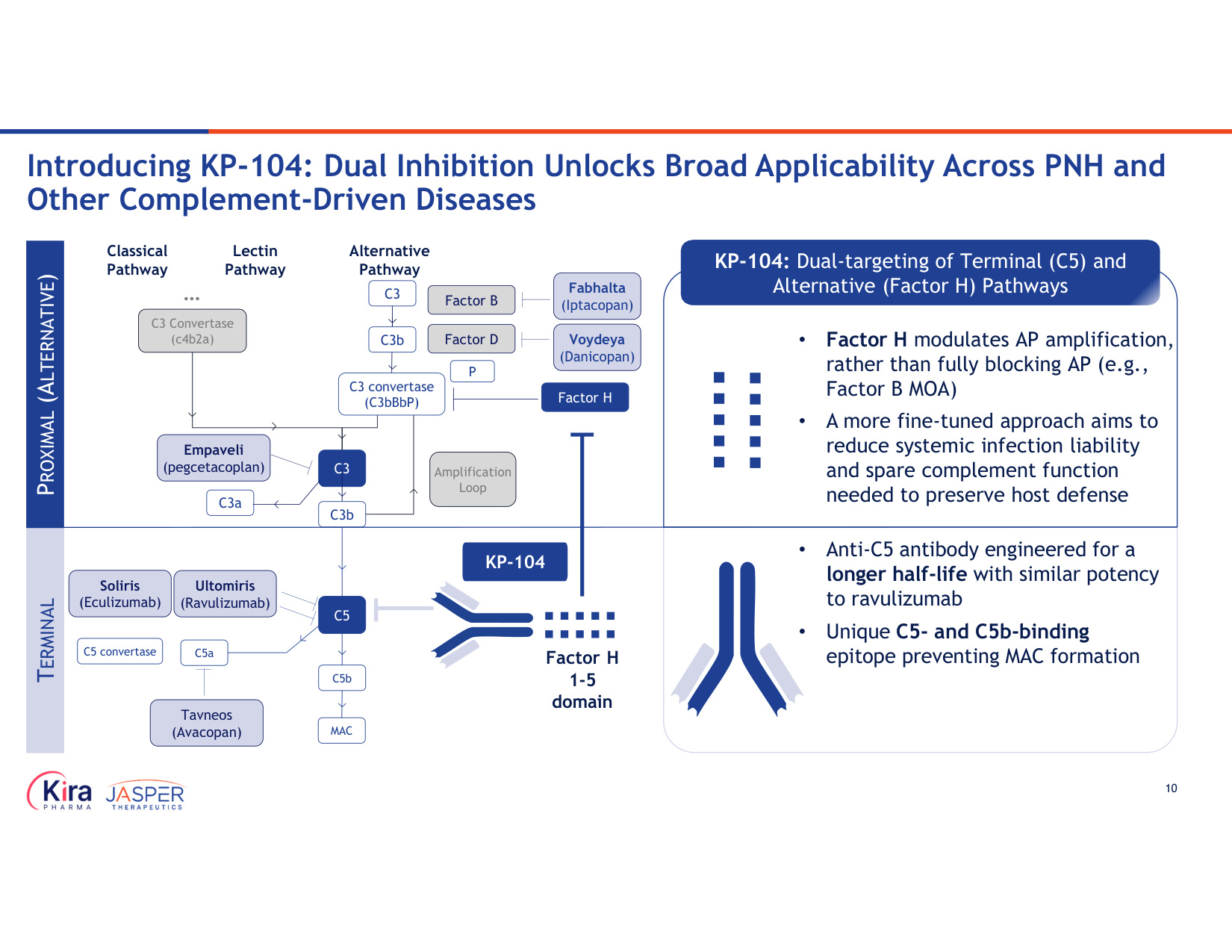
10 Introducing KP-104: Dual Inhibition Unlocks Broad Applicability Across PNH and Other Complement-Driven Diseases TERMINAL PROXIMAL (ALTERNATIVE) • Anti-C5 antibody engineered for a longer half-life with similar potency to ravulizumab • Unique C5- and C5b-binding epitope preventing MAC formation • Factor H modulates AP amplification, rather than fully blocking AP (e.g., Factor B MOA) • A more fine-tuned approach aims to reduce systemic infection liability and spare complement function needed to preserve host defense KP-104: Dual-targeting of Terminal (C5) and Alternative (Factor H) Pathways Factor B Factor D P C3 C3a Amplification Loop C3 convertase (C3bBbP) Factor H Empaveli (pegcetacoplan) Fabhalta (Iptacopan) Voydeya (Danicopan) Classical Pathway Lectin Pathway Alternative Pathway C3 Convertase (c4b2a) ... C3 C3b C3b Soliris (Eculizumab) C5 C5a C5b MAC C5 convertase Ultomiris (Ravulizumab) Tavneos (Avacopan) KP-104 Factor H 1-5 domain
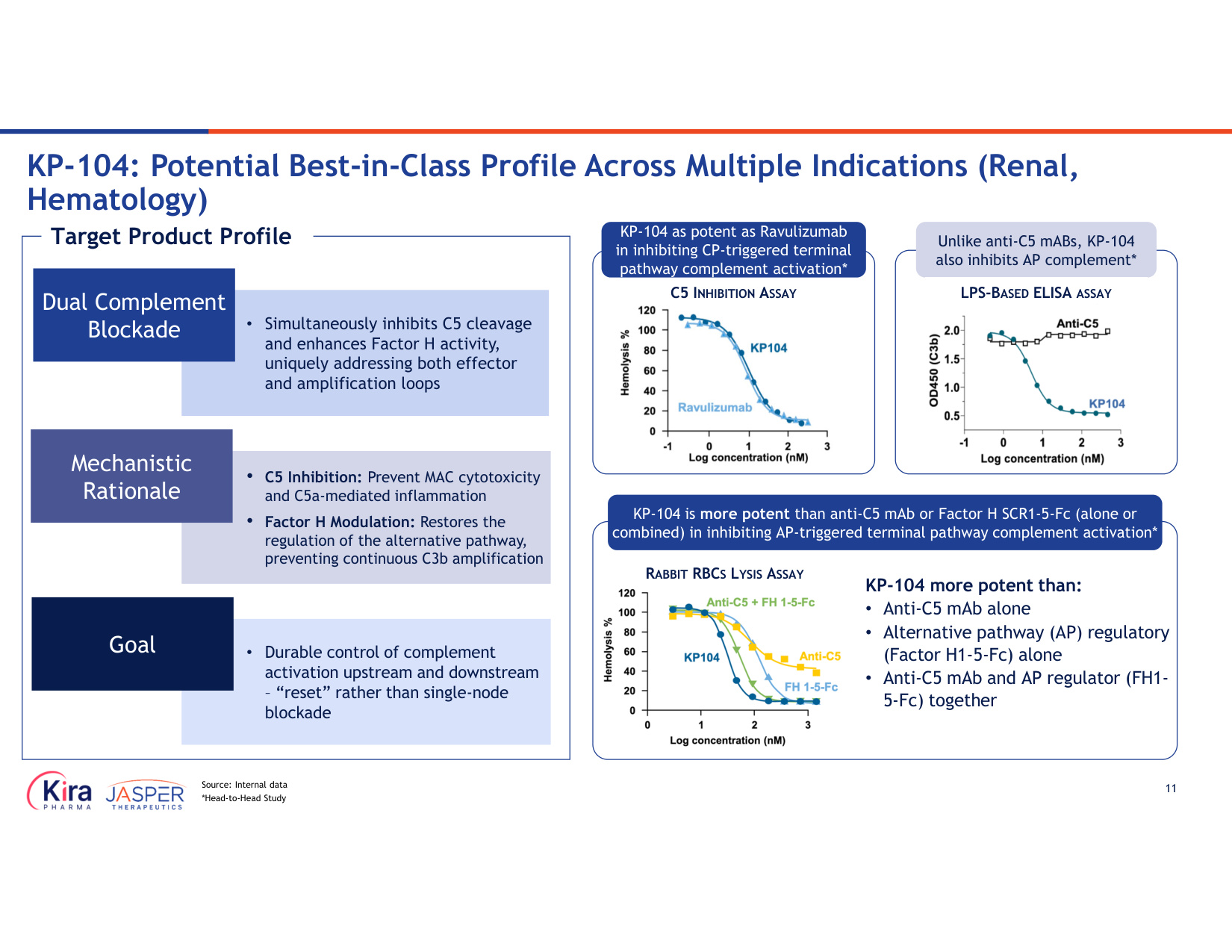
11 RABBIT RBCS LYSIS ASSAY KP-104 more potent than: • Anti-C5 mAb alone • Alternative pathway (AP) regulatory (Factor H1-5-Fc) alone • Anti-C5 mAb and AP regulator (FH1- 5-Fc) together KP-104 is more potent than anti-C5 mAb or Factor H SCR1-5-Fc (alone or combined) in inhibiting AP-triggered terminal pathway complement activation* Unlike anti-C5 mABs, KP-104 also inhibits AP complement* LPS-BASED ELISA ASSAY C5 INHIBITION ASSAY KP-104 as potent as Ravulizumab in inhibiting CP-triggered terminal pathway complement activation* • Simultaneously inhibits C5 cleavage and enhances Factor H activity, uniquely addressing both effector and amplification loops Dual Complement Blockade • C5 Inhibition: Prevent MAC cytotoxicity and C5a-mediated inflammation • Factor H Modulation: Restores the regulation of the alternative pathway, preventing continuous C3b amplification Mechanistic Rationale • Durable control of complement activation upstream and downstream – "reset" rather than single-node blockade Goal Target Product Profile KP-104: Potential Best-in-Class Profile Across Multiple Indications (Renal, Hematology) Source: Internal data *Head-to-Head Study
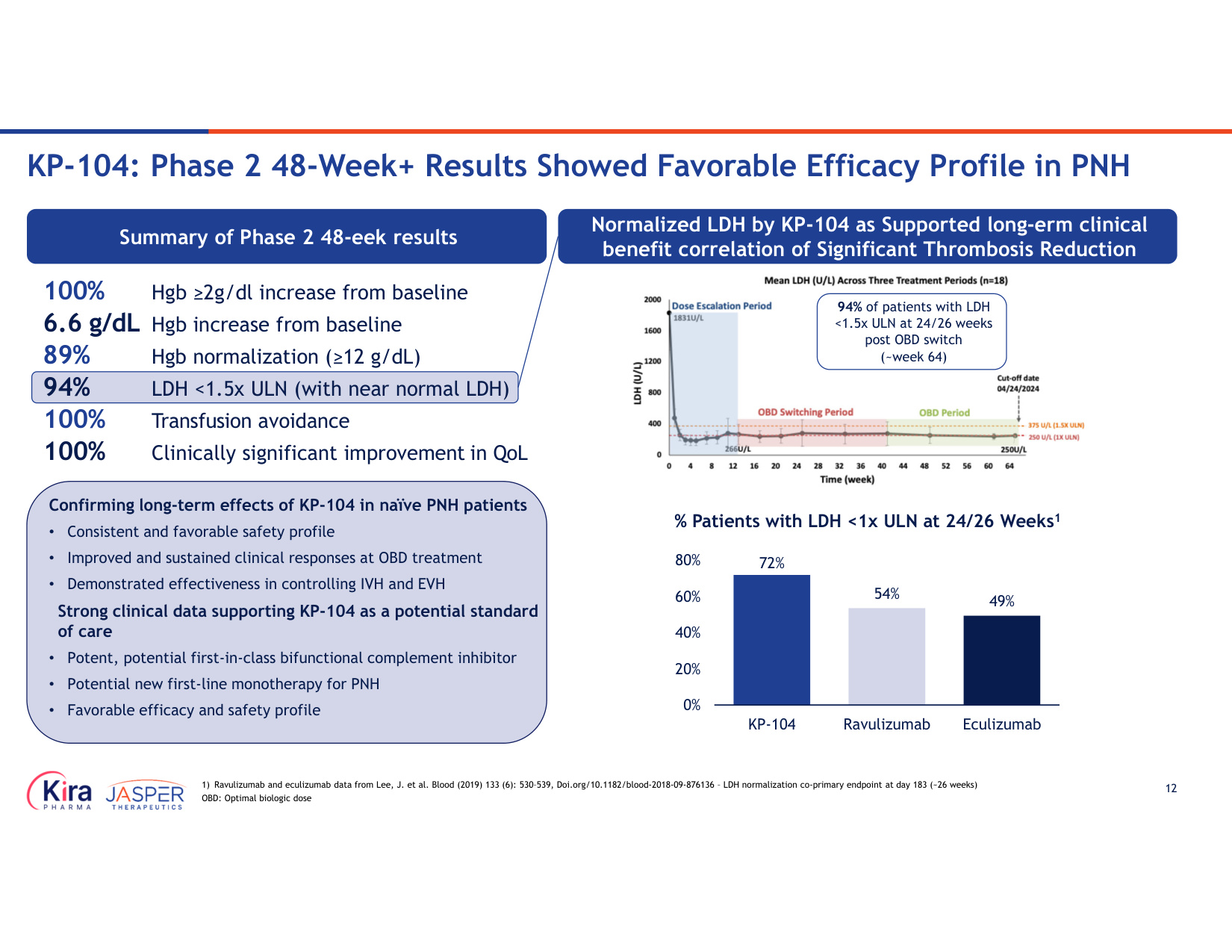
12 Confirming long-term effects of KP-104 in naïve PNH patients • Consistent and favorable safety profile • Improved and sustained clinical responses at OBD treatment • Demonstrated effectiveness in controlling IVH and EVH Strong clinical data supporting KP-104 as a potential standard of care • Potent, potential first-in-class bifunctional complement inhibitor • Potential new first-line monotherapy for PNH • Favorable efficacy and safety profile Summary of Phase 2 48-eek results 94% of patients with LDH <1.5x ULN at 24/26 weeks post OBD switch (~week 64) % Patients with LDH <1x ULN at 24/26 Weeks1 72% 54% 49% 0% 20% 40% 60% 80% KP-104 Ravulizumab Eculizumab Normalized LDH by KP-104 as Supported long-erm clinical benefit correlation of Significant Thrombosis Reduction 100% Hgb ≥2g/dl increase from baseline 6.6 g/dL Hgb increase from baseline 89% Hgb normalization (≥12 g/dL) 94% LDH <1.5x ULN (with near normal LDH) 100% Transfusion avoidance 100% Clinically significant improvement in QoL 1) Ravulizumab and eculizumab data from Lee, J. et al. Blood (2019) 133 (6): 530–539, Doi.org/10.1182/blood-2018-09-876136 – LDH normalization co-primary endpoint at day 183 (~26 weeks) OBD: Optimal biologic dose KP-104: Phase 2 48-Week+ Results Showed Favorable Efficacy Profile in PNH
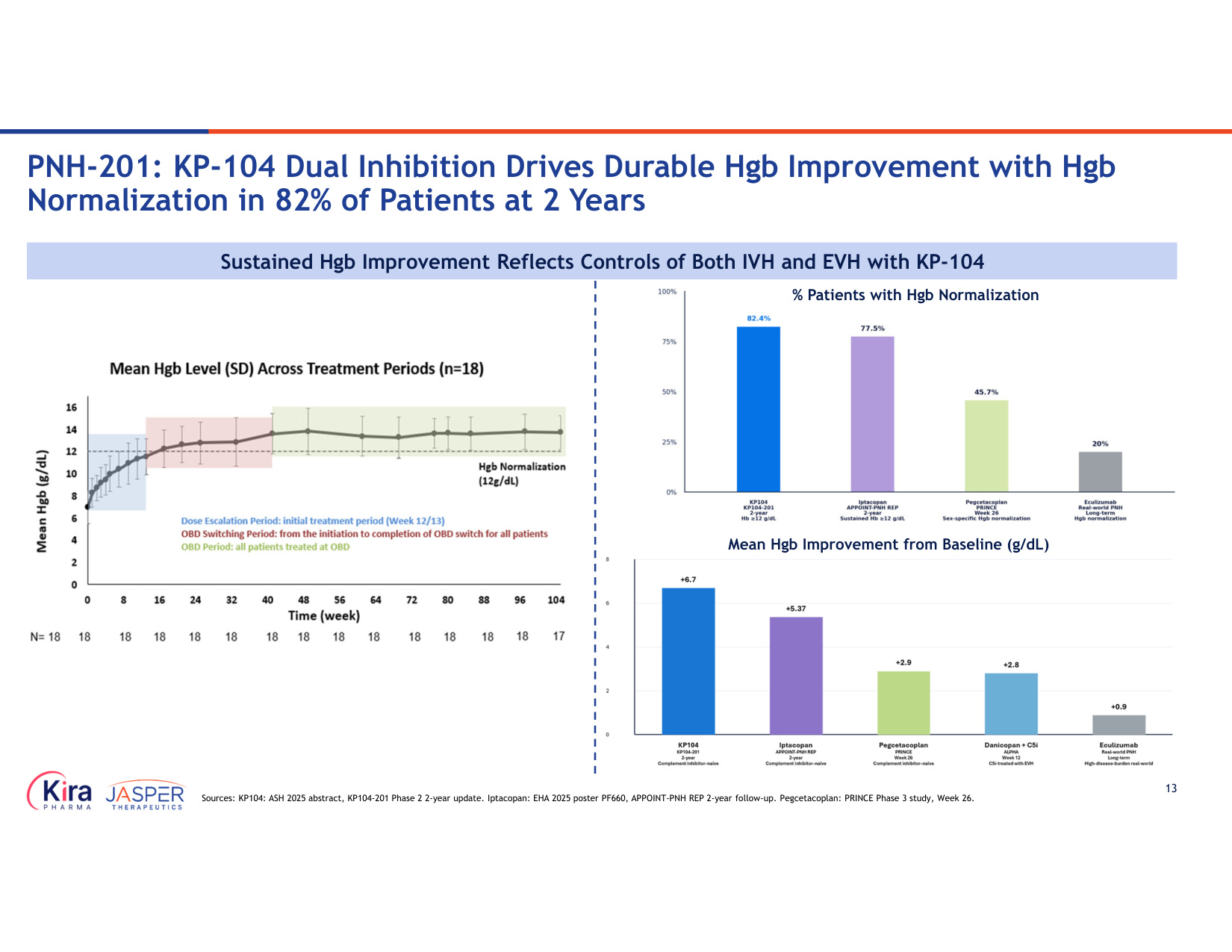
13 PNH-201: KP-104 Dual Inhibition Drives Durable Hgb Improvement with Hgb Normalization in 82% of Patients at 2 Years Sustained Hgb Improvement Reflects Controls of Both IVH and EVH with KP-104 % Patients with Hgb Normalization Mean Hgb Improvement from Baseline (g/dL) Sources: KP104: ASH 2025 abstract, KP104-201 Phase 2 2-year update. Iptacopan: EHA 2025 poster PF660, APPOINT-PNH REP 2-year follow-up. Pegcetacoplan: PRINCE Phase 3 study, Week 26.
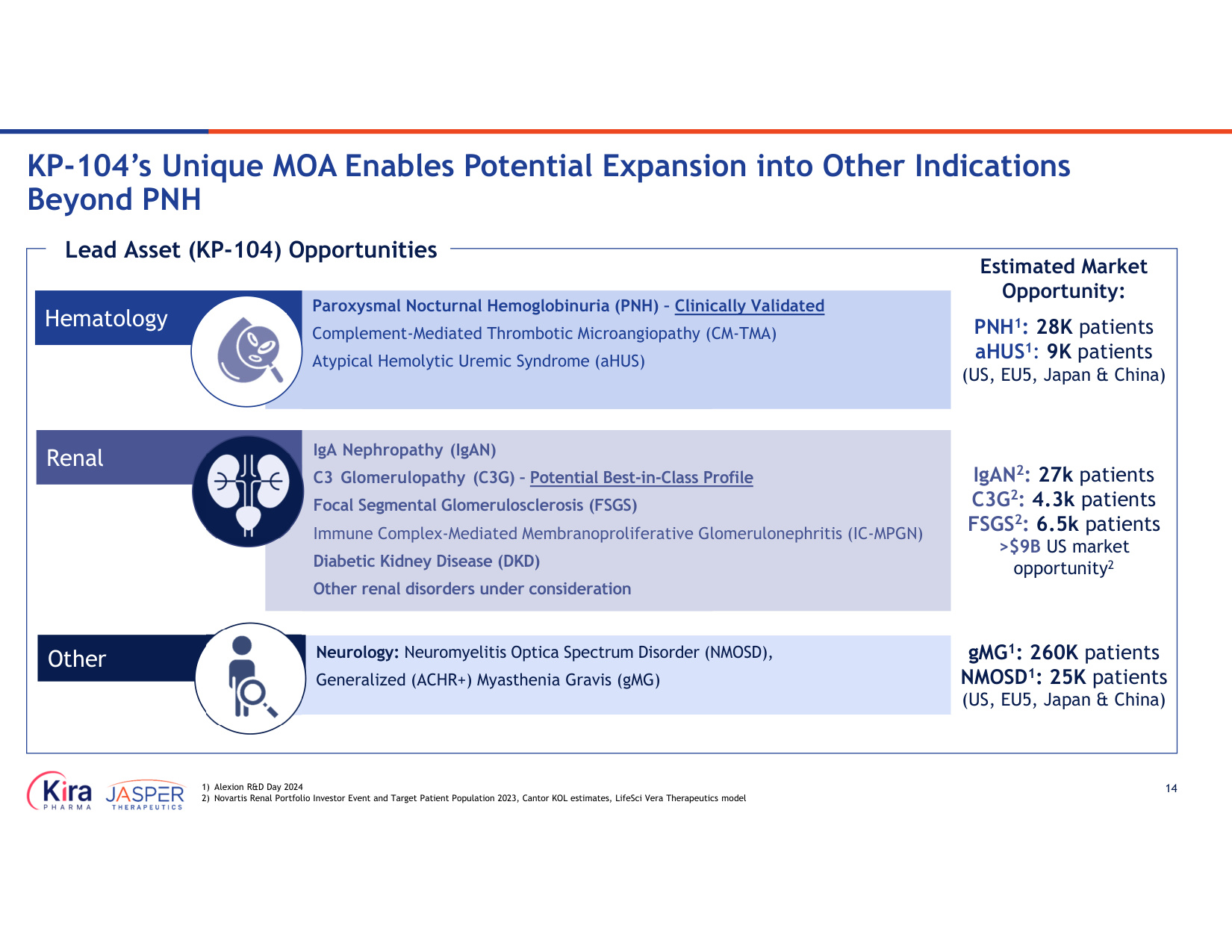
14 KP-104's Unique MOA Enables Potential Expansion into Other Indications Beyond PNH Hematology Lead Asset (KP-104) Opportunities Renal Other PNH1: 28K patients aHUS1: 9K patients (US, EU5, Japan & China) IgAN2: 27k patients C3G2: 4.3k patients FSGS2: 6.5k patients >$9B US market opportunity2 gMG1: 260K patients NMOSD1: 25K patients (US, EU5, Japan & China) Neurology: Neuromyelitis Optica Spectrum Disorder (NMOSD), Generalized (ACHR+) Myasthenia Gravis (gMG) IgA Nephropathy (IgAN) C3 Glomerulopathy (C3G) – Potential Best-in-Class Profile Focal Segmental Glomerulosclerosis (FSGS) Immune Complex-Mediated Membranoproliferative Glomerulonephritis (IC-MPGN) Diabetic Kidney Disease (DKD) Other renal disorders under consideration Paroxysmal Nocturnal Hemoglobinuria (PNH) – Clinically Validated Complement-Mediated Thrombotic Microangiopathy (CM-TMA) Atypical Hemolytic Uremic Syndrome (aHUS) 1) Alexion R&D Day 2024 2) Novartis Renal Portfolio Investor Event and Target Patient Population 2023, Cantor KOL estimates, LifeSci Vera Therapeutics model Estimated Market Opportunity:
15 Opportunity to demonstrate KP-104's best-in-class potential and differentiated profile in renal indications vs. other complement inhibitors KP-104 is Being Evaluated in an Ongoing Phase 2 Basket Study in Rare Renal Indications With Potential to Achieve Fast POC IgAN • IgAN pathogenesis involves both alternative pathway (AP) and lectin pathway (LP) complement C3G • KP-104 demonstrated best-in-class potential, with improvements observed in renal function and pathology including C3 and C9 glomeruli deposition elimination compared to C5 mAb alone FSGS and Other Renal Disorders • Robust in vitro and in vivo data supporting multiple complement pathway in FSGS • Opportunity to expand into other renal disorders
Briquilimab Potential Best-in-Class Anti-KIT Antibody
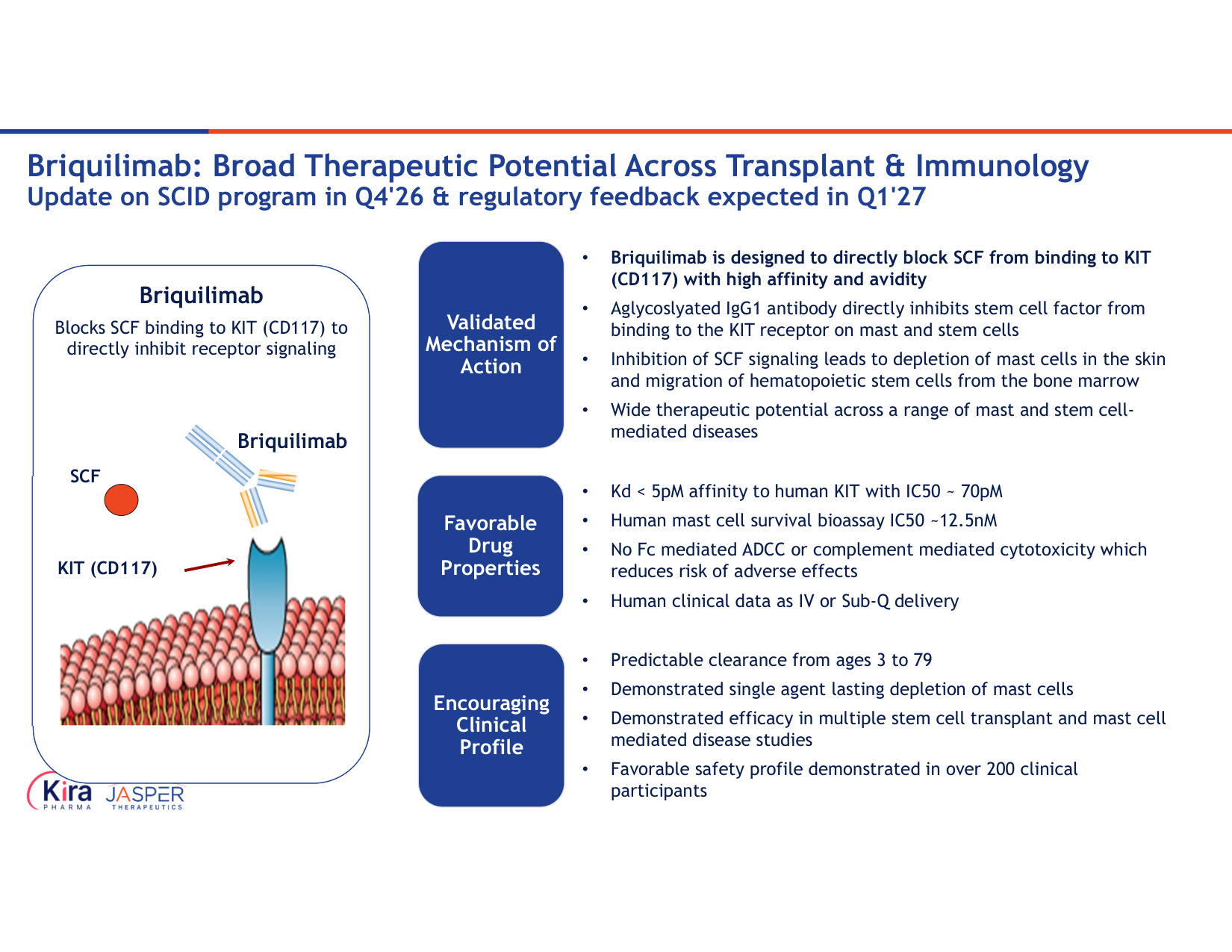
17 Briquilimab: Broad Therapeutic Potential Across Transplant & Immunology Update on SCID program in Q4'26 & regulatory feedback expected in Q1'27 SCF KIT (CD117) Briquilimab Briquilimab Blocks SCF binding to KIT (CD117) to directly inhibit receptor signaling Validated Mechanism of Action • Briquilimab is designed to directly block SCF from binding to KIT (CD117) with high affinity and avidity • Aglycoslyated IgG1 antibody directly inhibits stem cell factor from binding to the KIT receptor on mast and stem cells • Inhibition of SCF signaling leads to depletion of mast cells in the skin and migration of hematopoietic stem cells from the bone marrow • Wide therapeutic potential across a range of mast and stem cell- mediated diseases Favorable Drug Properties • Kd < 5pM affinity to human KIT with IC50 ~ 70pM • Human mast cell survival bioassay IC50 ~12.5nM • No Fc mediated ADCC or complement mediated cytotoxicity which reduces risk of adverse effects • Human clinical data as IV or Sub-Q delivery Encouraging Clinical Profile • Predictable clearance from ages 3 to 79 • Demonstrated single agent lasting depletion of mast cells • Demonstrated efficacy in multiple stem cell transplant and mast cell mediated disease studies • Favorable safety profile demonstrated in over 200 clinical participants
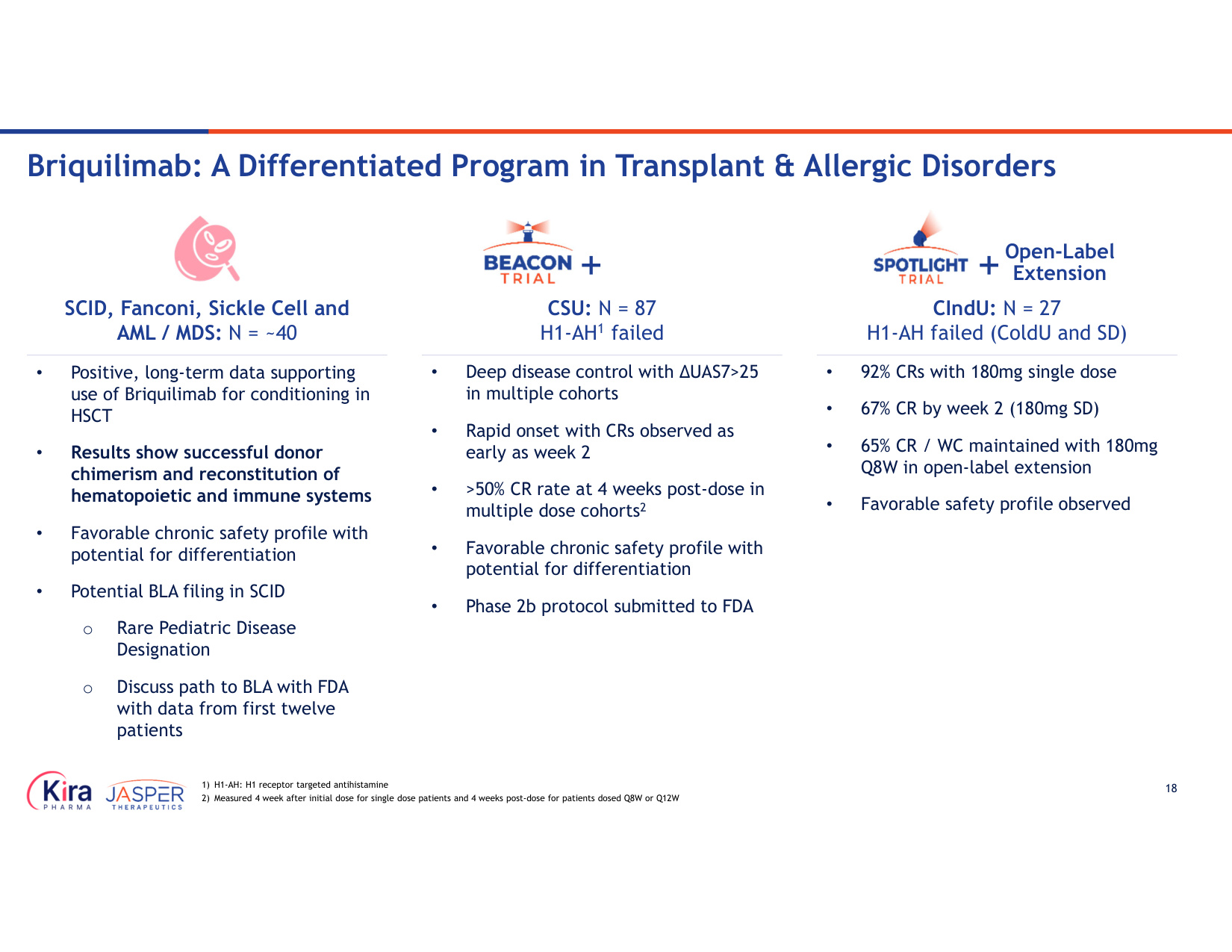
18 Open-Label Extension CSU: N = 87 H1-AH1 failed CIndU: N = 27 H1-AH failed (ColdU and SD) SCID, Fanconi, Sickle Cell and AML / MDS: N = ~40 • Positive, long-term data supporting use of Briquilimab for conditioning in HSCT • Results show successful donor chimerism and reconstitution of hematopoietic and immune systems • Favorable chronic safety profile with potential for differentiation • Potential BLA filing in SCID o Rare Pediatric Disease Designation o Discuss path to BLA with FDA with data from first twelve patients • Deep disease control with ∆UAS7>25 in multiple cohorts • Rapid onset with CRs observed as early as week 2 • >50% CR rate at 4 weeks post-dose in multiple dose cohorts2 • Favorable chronic safety profile with potential for differentiation • Phase 2b protocol submitted to FDA • 92% CRs with 180mg single dose • 67% CR by week 2 (180mg SD) • 65% CR / WC maintained with 180mg Q8W in open-label extension • Favorable safety profile observed Briquilimab: A Differentiated Program in Transplant & Allergic Disorders 1) H1-AH: H1 receptor targeted antihistamine 2) Measured 4 week after initial dose for single dose patients and 4 weeks post-dose for patients dosed Q8W or Q12W
19 Multiple Potential FDA Filing Strategies: • SCID re-transplant patients are ultra orphan, high unmet need population • Focused on data with Briquilimab in 11 SCID re-transplant T-B- patients • Immune reconstitution (chimerism, naïve T-cells) • Function immunity (reduction of IVIG, infections, response to vaccination) • Additional longitudinal data in existing patients and separate natural history data • Combined Company has 5-year follow up data in patients • Example: Rocket Pharmaceuticals recent approval of KRESLADI provides roadmap to support approval path • Allogeneic stem cell transplant can restore bone marrow and blood formation in Fanconi anemia patients • Development strategy: • Discuss path to BLA with FDA with 2 yr-data in first three patients • Consider expansion to additional clinical sites following FDA discussion • Successful development of Briquilimab in Fanconi anemia may lead to rare pediatric disease designation and a Priority Review Voucher Briquilimab granted Rare Pediatric Disease Designation in SCID and may be eligible for Priority Review Voucher (PRV) with approval SCID and Fanconi anemia are difficult to treat ultra-orphan disorders where HCT is the only proven cure, but challenging setting due to limited pre-conditioning options Briquilimab: Potential US Licensing Pathway & PRV Opportunity for SCID
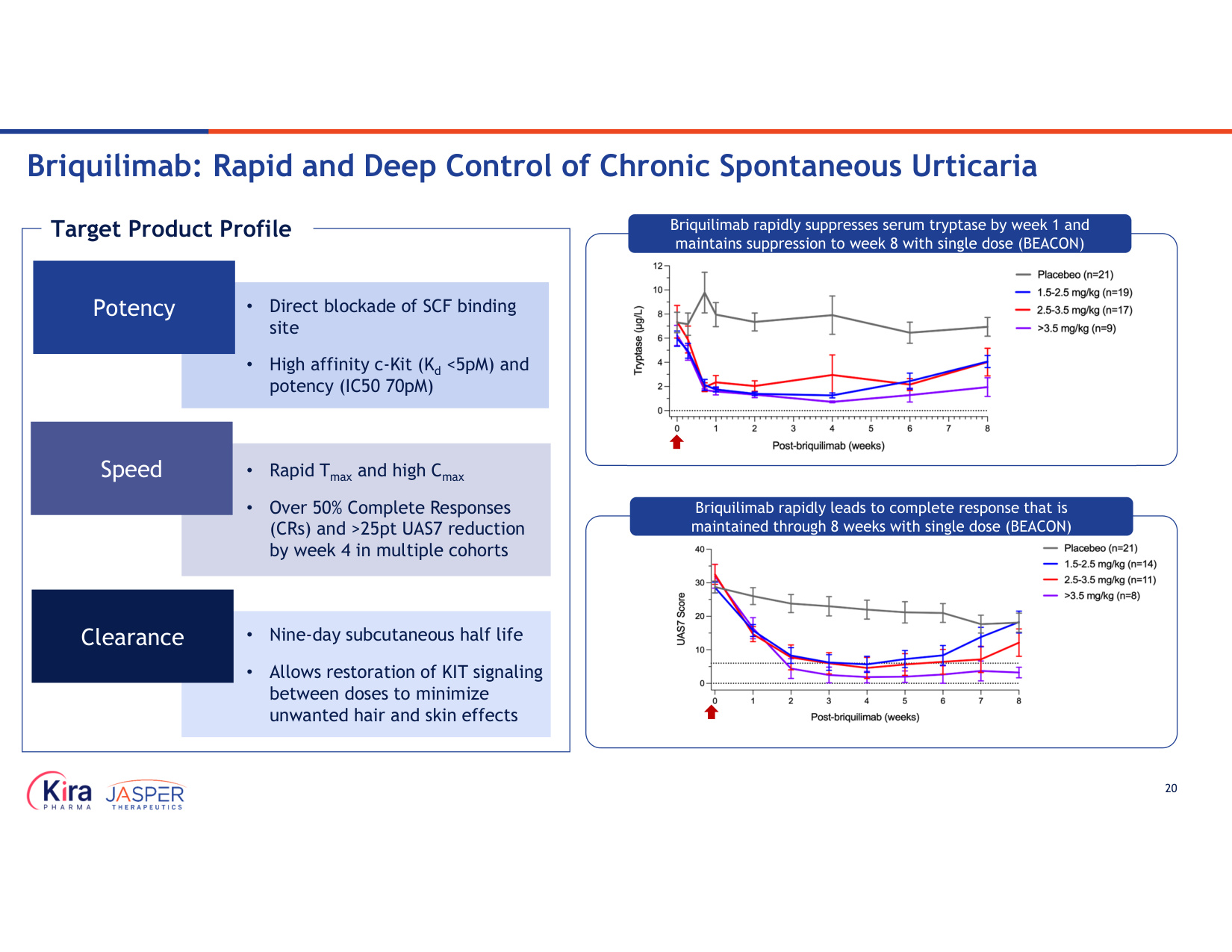
20 Briquilimab: Rapid and Deep Control of Chronic Spontaneous Urticaria • Direct blockade of SCF binding site • High affinity c-Kit (Kd <5pM) and potency (IC50 70pM) Potency • Rapid Tmax and high Cmax • Over 50% Complete Responses (CRs) and >25pt UAS7 reduction by week 4 in multiple cohorts Speed • Nine-day subcutaneous half life • Allows restoration of KIT signaling between doses to minimize unwanted hair and skin effects Clearance Target Product Profile Briquilimab rapidly suppresses serum tryptase by week 1 and maintains suppression to week 8 with single dose (BEACON) Briquilimab rapidly leads to complete response that is maintained through 8 weeks with single dose (BEACON)
KP-701 Potentially Best-in-Class Anti-CD79BxCD32B
22 KP-701 (CD79BxCD32B): potential best-in-class B-cell control New Emphasis Beyond Conventional B-Cell Depletion MOAs • Human genetics supports B-cell control • Prior proof-of-concept with weaker molecules & similar Fc constructs (e.g., PRV3279, Obexelimab) • Recent positive Obexelimab Phase 2 & Phase 3 data • Platform program to build around (e.g., FcRn & APRIL / BAFF class) • Multiple go-forward large indications under consideration Validated Target with Human POC • Blockade of CD79B and engagement of CD32B suppresses B-cell function, lowers cytokine and autoantibody production • Demonstrated B-cell inhibition & phagocytosis (ADCP) without CDC or ADCC in NHPs • CTA-ready, potential rapid path in patients in China • Efficient path to proof-of- concept in HV and autoimmune disease patients • Once-monthly dosing potential Compelling Preclinical Data & Clinical Strategy
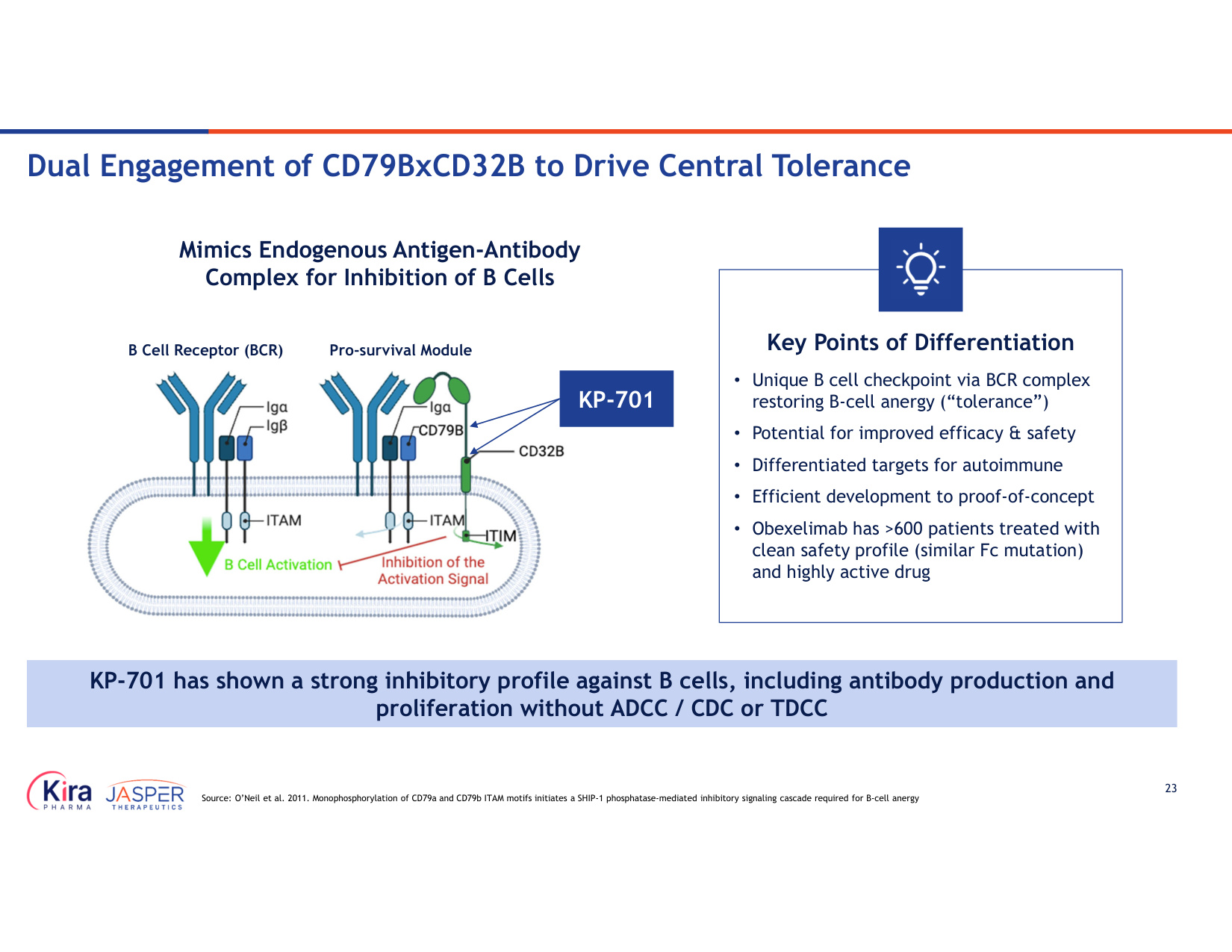
23 Source: O'Neil et al. 2011. Monophosphorylation of CD79a and CD79b ITAM motifs initiates a SHIP-1 phosphatase-mediated inhibitory signaling cascade required for B-cell anergy Mimics Endogenous Antigen-Antibody Complex for Inhibition of B Cells Key Points of Differentiation • Unique B cell checkpoint via BCR complex restoring B-cell anergy ("tolerance") • Potential for improved efficacy & safety • Differentiated targets for autoimmune • Efficient development to proof-of-concept • Obexelimab has >600 patients treated with clean safety profile (similar Fc mutation) and highly active drug KP-701 B Cell Receptor (BCR) Pro-survival Module KP-701 has shown a strong inhibitory profile against B cells, including antibody production and proliferation without ADCC / CDC or TDCC Dual Engagement of CD79BxCD32B to Drive Central Tolerance
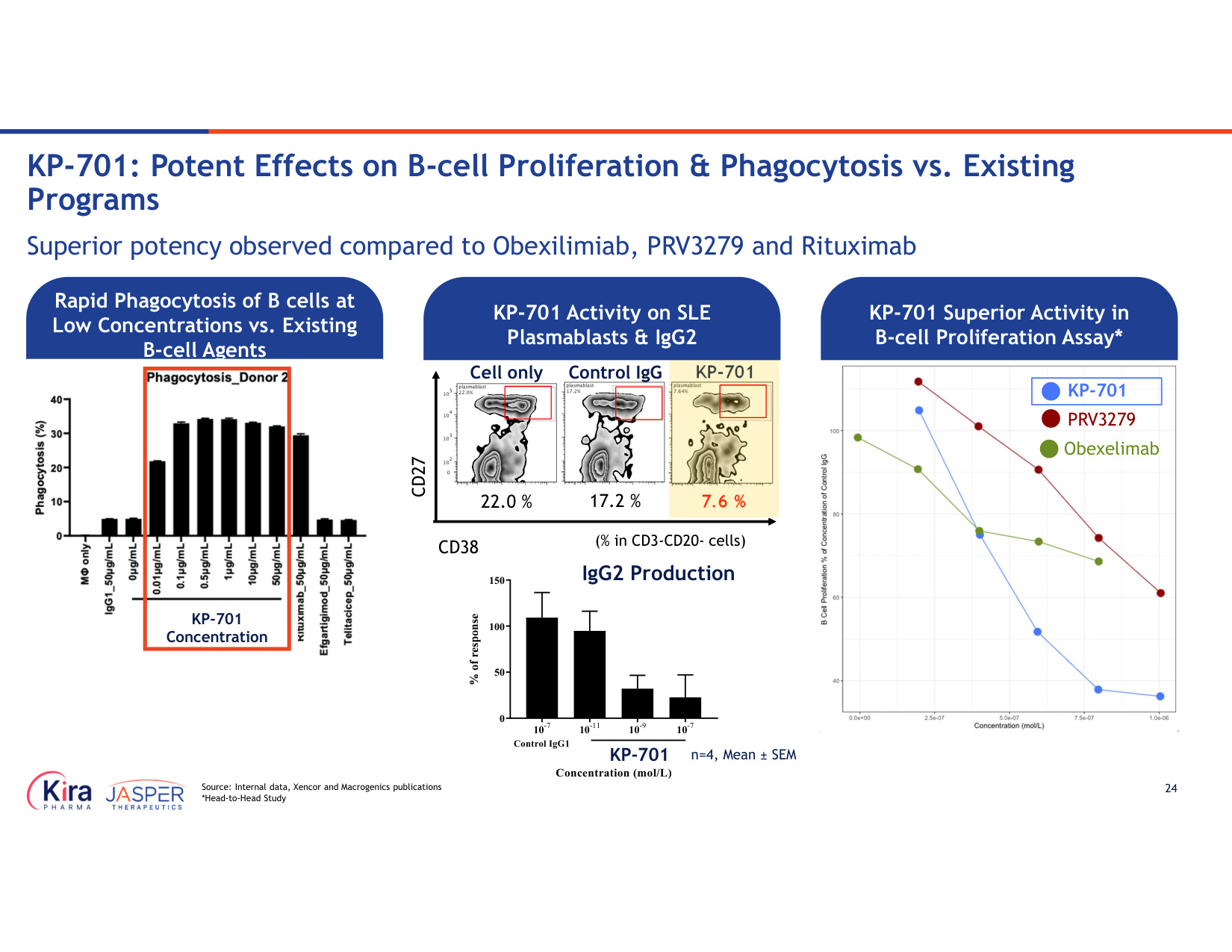
24 Source: Internal data, Xencor and Macrogenics publications *Head-to-Head Study Superior potency observed compared to Obexilimiab, PRV3279 and Rituximab KP-701: Potent Effects on B-cell Proliferation & Phagocytosis vs. Existing Programs KP-701 Control IgG CD27 CD38 7.6 % 22.0 % Cell only 17.2 % (% in CD3-CD20- cells) n=4, Mean ± SEM 10-7 10-11 10-9 10-7 0 50 100 150 Concentration (mol/L) Control IgG1 ASP2713 IgG2 Production KP-701 KP-701 Activity on SLE Plasmablasts & IgG2 PRV3279 KP-701 Superior Activity in B-cell Proliferation Assay* Rapid Phagocytosis of B cells at Low Concentrations vs. Existing B-cell Agents KP-701 Concentration KP-701 Obexelimab
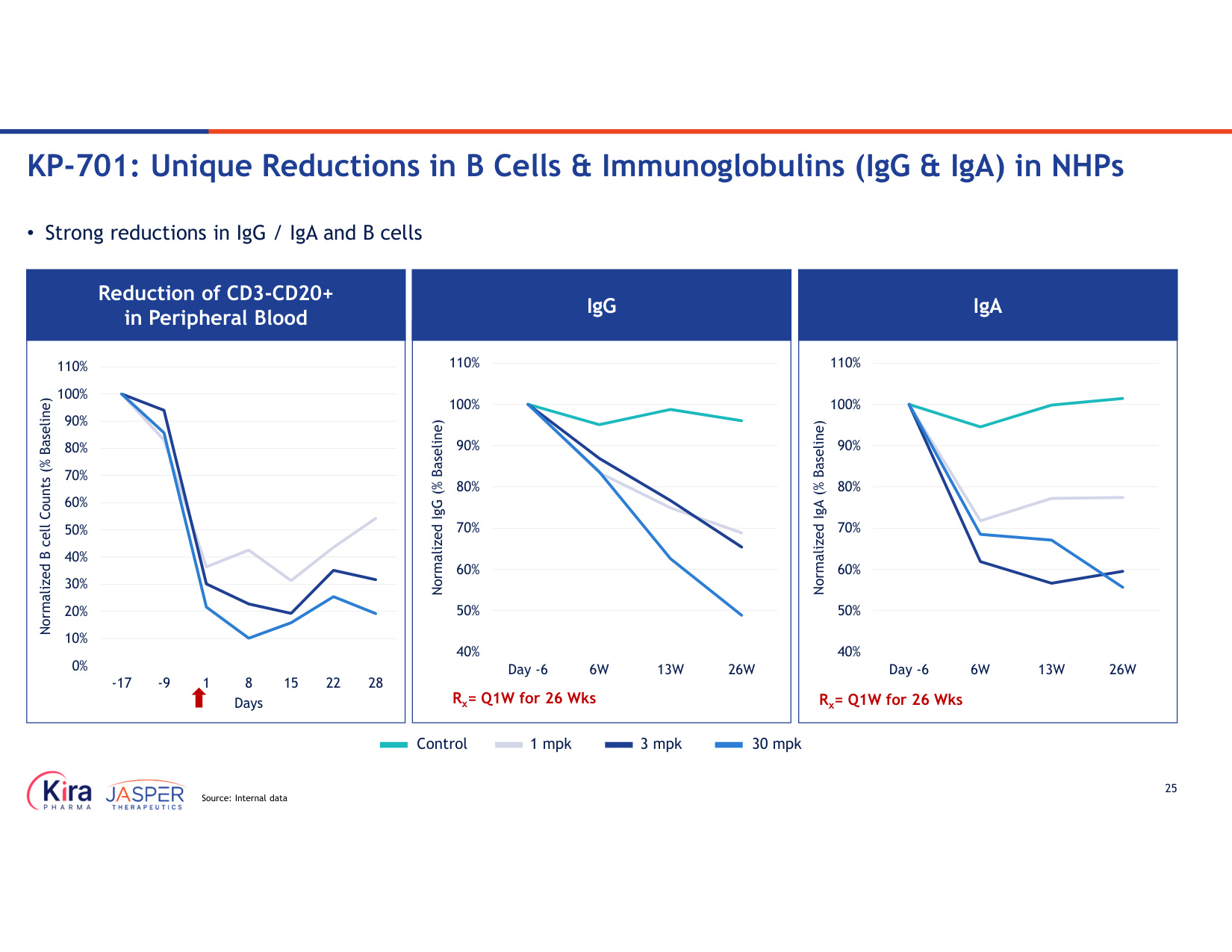
25 0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100% 110% -17 -9 1 8 15 22 28 Normalized B cell Counts (% Baseline) Days Reduction of CD3-CD20+ in Peripheral Blood 40% 50% 60% 70% 80% 90% 100% 110% Day -6 6W 13W 26W Normalized IgG (% Baseline) Rx= Q1W for 26 Wks IgG 40% 50% 60% 70% 80% 90% 100% 110% Day -6 6W 13W 26W Normalized IgA (% Baseline) Rx= Q1W for 26 Wks IgA Control 1 mpk 3 mpk 30 mpk • Strong reductions in IgG / IgA and B cells KP-701: Unique Reductions in B Cells & Immunoglobulins (IgG & IgA) in NHPs Source: Internal data
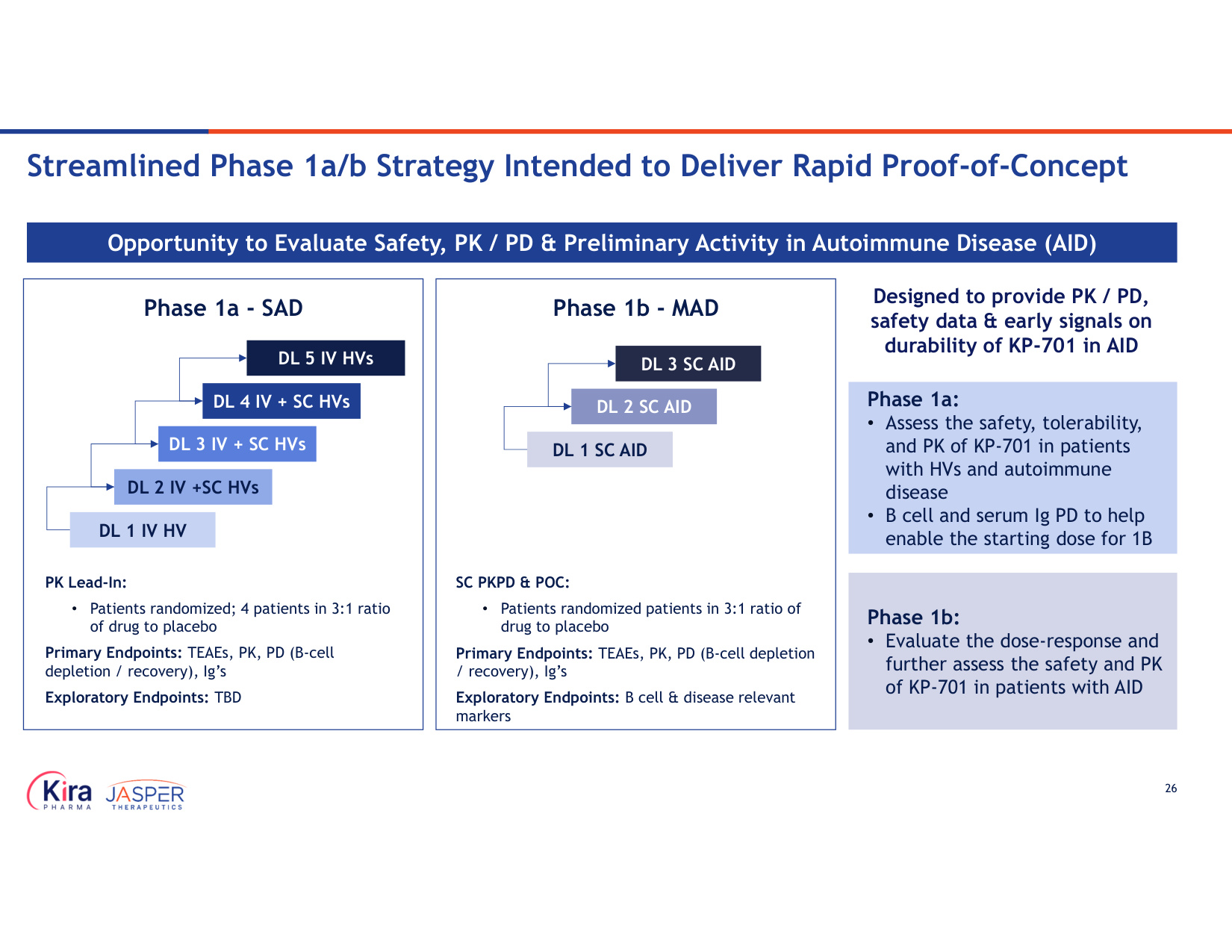
26 Streamlined Phase 1a/b Strategy Intended to Deliver Rapid Proof-of-Concept Phase 1a - SAD Phase 1b - MAD Phase 1a: • Assess the safety, tolerability, and PK of KP-701 in patients with HVs and autoimmune disease • B cell and serum Ig PD to help enable the starting dose for 1B Opportunity to Evaluate Safety, PK / PD & Preliminary Activity in Autoimmune Disease (AID) PK Lead-In: • Patients randomized; 4 patients in 3:1 ratio of drug to placebo Primary Endpoints: TEAEs, PK, PD (B-cell depletion / recovery), Ig's Exploratory Endpoints: TBD SC PKPD & POC: • Patients randomized patients in 3:1 ratio of drug to placebo Primary Endpoints: TEAEs, PK, PD (B-cell depletion / recovery), Ig's Exploratory Endpoints: B cell & disease relevant markers DL 1 IV HV DL 2 IV +SC HVs DL 3 IV + SC HVs DL 4 IV + SC HVs DL 5 IV HVs DL 1 SC AID DL 2 SC AID Designed to provide PK / PD, safety data & early signals on durability of KP-701 in AID Phase 1b: • Evaluate the dose-response and further assess the safety and PK of KP-701 in patients with AID DL 3 SC AID
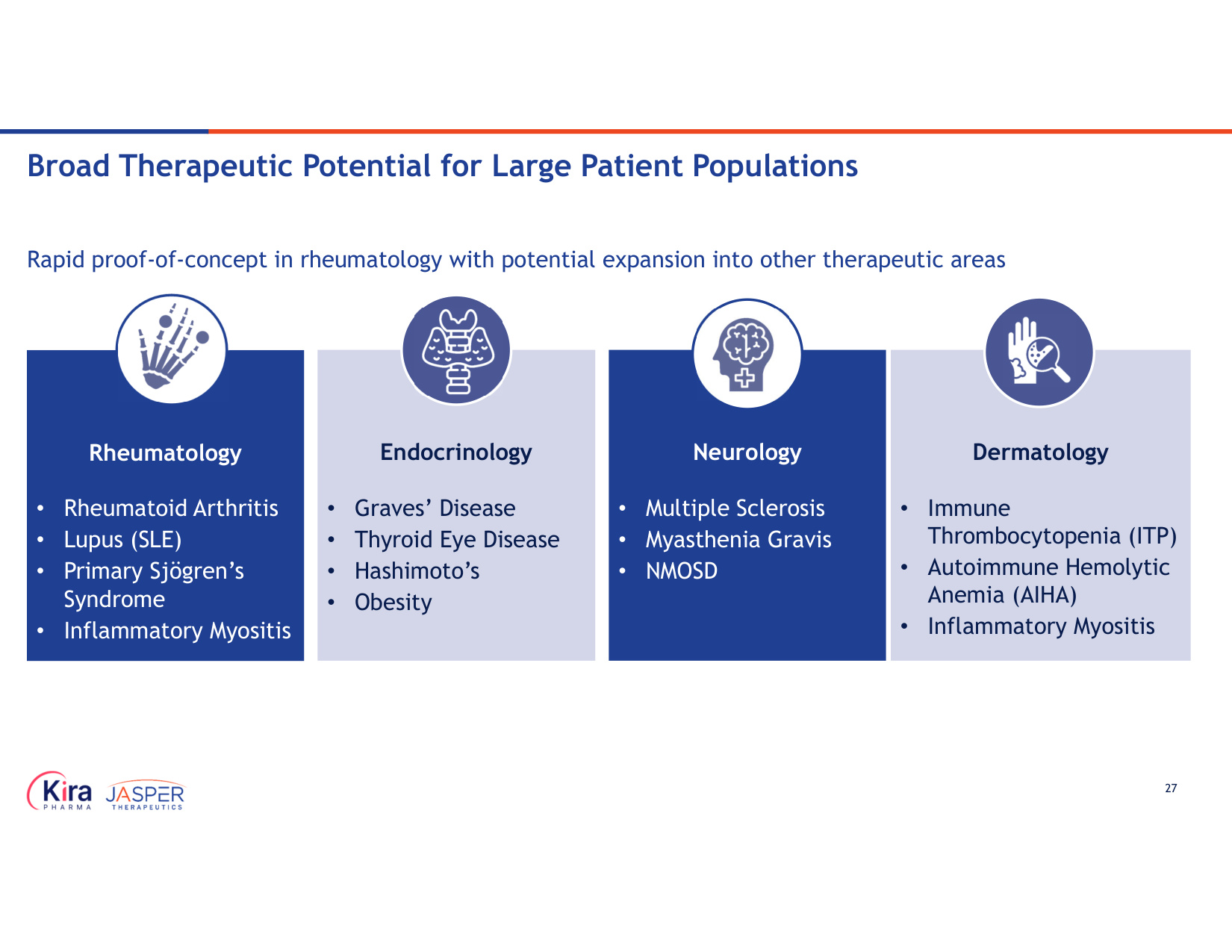
27 Rapid proof-of-concept in rheumatology with potential expansion into other therapeutic areas Rheumatology • Rheumatoid Arthritis • Lupus (SLE) • Primary Sjögren's Syndrome • Inflammatory Myositis Dermatology • Immune Thrombocytopenia (ITP) • Autoimmune Hemolytic Anemia (AIHA) • Inflammatory Myositis Endocrinology • Graves' Disease • Thyroid Eye Disease • Hashimoto's • Obesity Neurology • Multiple Sclerosis • Myasthenia Gravis • NMOSD Broad Therapeutic Potential for Large Patient Populations
Summary
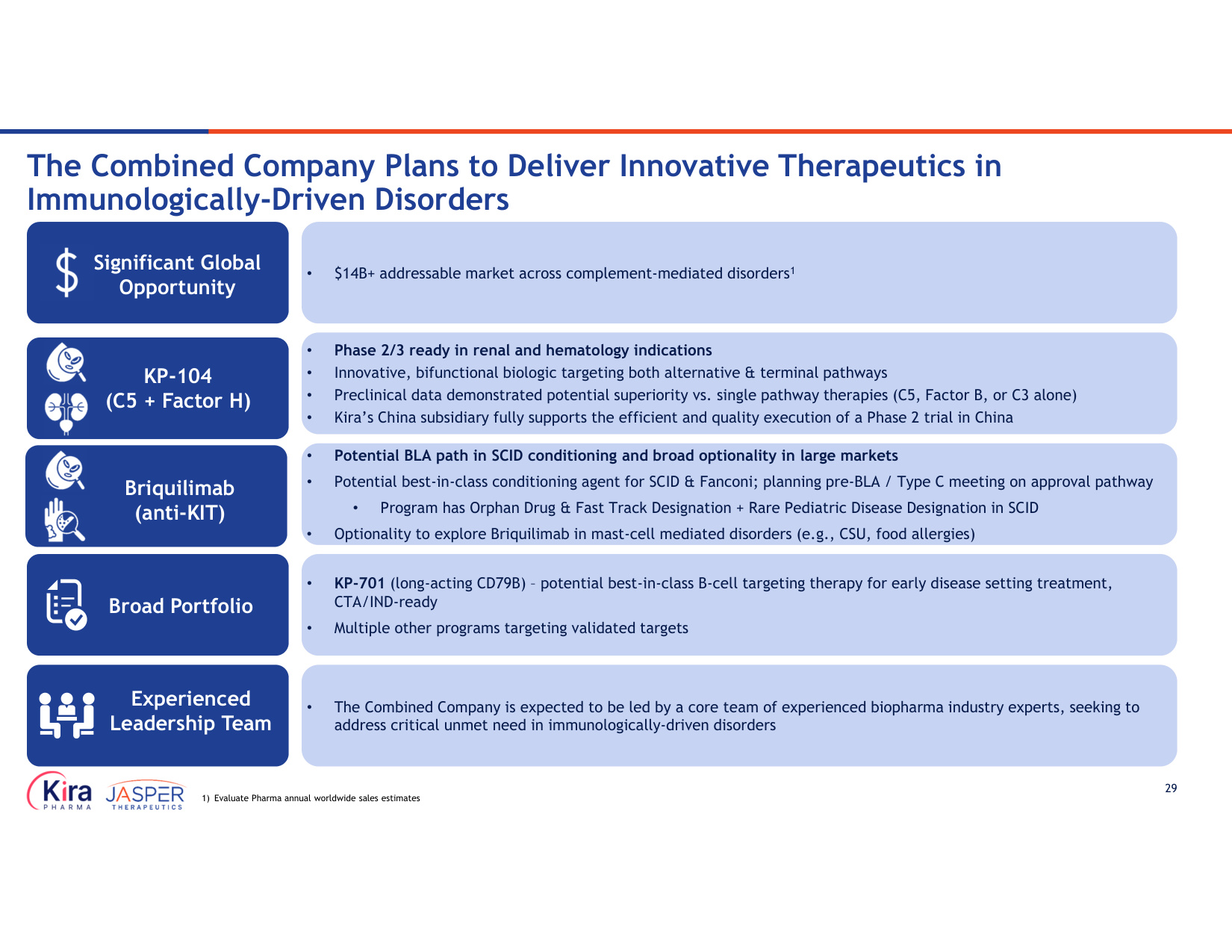
29 • $14B+ addressable market across complement-mediated disorders1 • Phase 2/3 ready in renal and hematology indications • Innovative, bifunctional biologic targeting both alternative & terminal pathways • Preclinical data demonstrated potential superiority vs. single pathway therapies (C5, Factor B, or C3 alone) • Kira's China subsidiary fully supports the efficient and quality execution of a Phase 2 trial in China • Potential BLA path in SCID conditioning and broad optionality in large markets • Potential best-in-class conditioning agent for SCID & Fanconi; planning pre-BLA / Type C meeting on approval pathway • Program has Orphan Drug & Fast Track Designation + Rare Pediatric Disease Designation in SCID • Optionality to explore Briquilimab in mast-cell mediated disorders (e.g., CSU, food allergies) • The Combined Company is expected to be led by a core team of experienced biopharma industry experts, seeking to address critical unmet need in immunologically-driven disorders • KP-701 (long-acting CD79B) – potential best-in-class B-cell targeting therapy for early disease setting treatment, CTA/IND-ready • Multiple other programs targeting validated targets The Combined Company Plans to Deliver Innovative Therapeutics in Immunologically-Driven Disorders 1) Evaluate Pharma annual worldwide sales estimates Significant Global Opportunity KP-104 (C5 + Factor H) Briquilimab (anti-KIT) Broad Portfolio Experienced Leadership Team
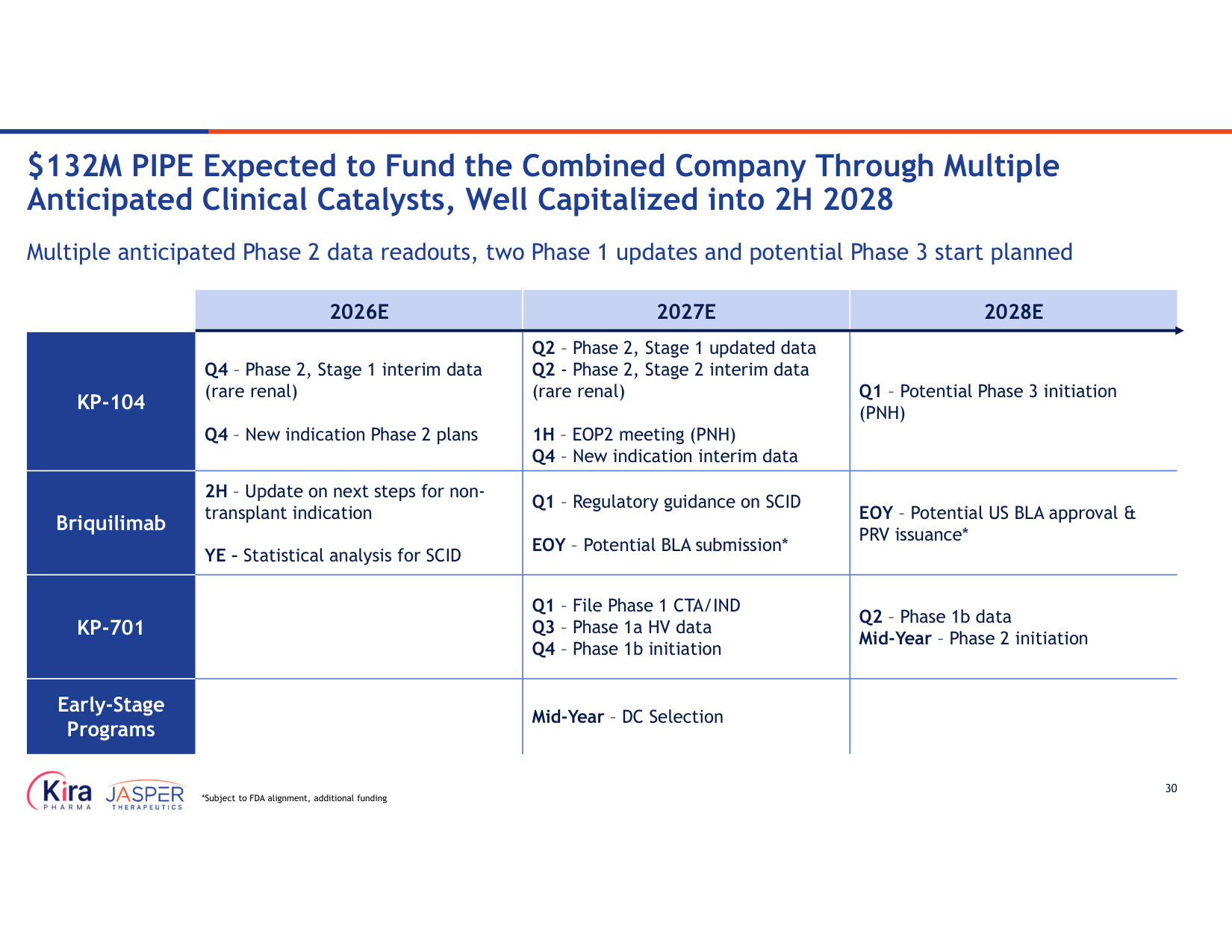
30 2028E 2027E 2026E Q1 – Potential Phase 3 initiation (PNH) Q2 – Phase 2, Stage 1 updated data Q2 - Phase 2, Stage 2 interim data (rare renal) 1H – EOP2 meeting (PNH) Q4 – New indication interim data Q4 – Phase 2, Stage 1 interim data (rare renal) Q4 – New indication Phase 2 plans KP-104 EOY – Potential US BLA approval & PRV issuance* Q1 – Regulatory guidance on SCID EOY – Potential BLA submission* 2H – Update on next steps for non- transplant indication YE – Statistical analysis for SCID Briquilimab Q2 – Phase 1b data Mid-Year – Phase 2 initiation Q1 – File Phase 1 CTA/IND Q3 – Phase 1a HV data Q4 – Phase 1b initiation KP-701 Mid-Year – DC Selection Early-Stage Programs Multiple anticipated Phase 2 data readouts, two Phase 1 updates and potential Phase 3 start planned $132M PIPE Expected to Fund the Combined Company Through Multiple Anticipated Clinical Catalysts, Well Capitalized into 2H 2028 *Subject to FDA alignment, additional funding