
Exhibit 99.1
Pioneering Bisphosphocin® Compounds Advancing a novel class of fast- acting antimicrobials toaddress the global threat ofresistance 1
Forward-looking Statements This presentation may contain forward-looking statements as defined by the Private Securities Litigation Reform Act of 1995. Generally, the words "believe," "expect," "intends," "estimate," "anticipate," "project," "will" and similar expressions identify forward-looking statements, which generally are not historical in nature. However, the absence of these words or similar expressions does not m e a n that a statement is not forward-looking. All statements that address operating performance, events or developments that we expect or anticipate will occur in the future are forward-looking statements. Management believes that these forward-looking statements are reasonable as and when made. However, caution should be taken not to place undue reliance on any such forward-looking statements because such statements speak only as of the date when made. Our C ompany undertakes no obligation to publicly update or revise any forward-looking statements, whether as a result of new information, future events or otherwise, except as required by law. In addition, forward-looking statements are subject to certain risks and uncertainties that could cause our Company's actual results to differ materially from historical experience and our present expectations or projections. Relying on such statements involves risk, uncertainty and assumptions. These statements are based on the current estimates and assumptions of the ma n a gement of Lakewood‐Amedex Biotherapeutics Inc. as of the date of this press release and are subject to uncertainty and changes. All statements obtained in this press release are ma d e only as of the date of this press release and Lakewood‐Amedex Biotherapeutics Inc. does not undertake any obligation to publicly update any forward‐looking statements. 2
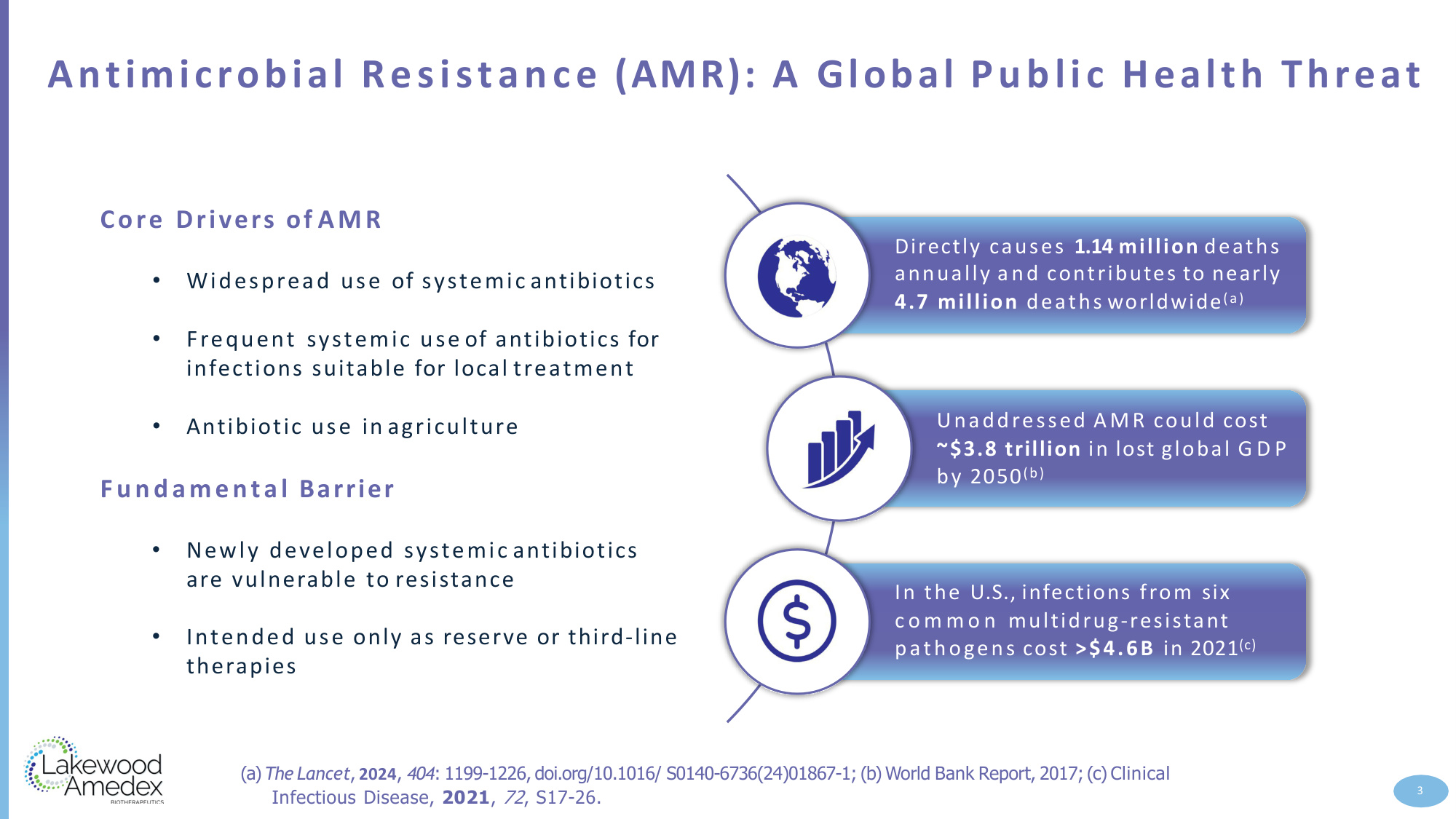
Antimicrobial Resistance (AMR): A Global Public Health Threat Directly causes 1.14 million deaths annually and contributes to nearly 4.7 million deaths worldwide(a) Unaddressed AMR could cost ~$3.8 trillion in lost global G D P by 2050(b) In the U.S., infections from six c o m m o n multidrug-resistant pathogens cost >$4.6B in 2021(c) Core Drivers of AMR 3 • Widespread use of systemic antibiotics • Frequent systemic use of antibiotics for infections suitable for local treatment • Antibiotic use in agriculture Fundamental Barrier • Newly developed systemic antibiotics are vulnerable to resistance • Intended use only as reserve or third-line therapies (a) The Lancet, 2024, 404: 1199-1226, doi.org/10.1016/ S0140-6736(24)01867-1; (b) World Bank Report, 2017; (c) Clinical Infectious Disease, 2021, 72, S17-26.
Value Proposition of Patented Bisphosphocin ® Class First-in-class, antimicrobial compounds with potential to mitigate the impact of the global AMR crisis Broad-spectrum activity against both susceptible and clinically relevant resistant pathogens ( a) Demonstrated cidal activity against biofilm organisms (b) Favorable resistance profile with low risk of resistance development (a) Local delivery achieves high concentration at the site of infection Reduced likelihood of systemic side effects due to targeted delivery 4 (a) –Cooper K, et al, Antimicrobial Agents and Chemotherapy, 2025, https://doi.org/10.1128/aac.00948-25; (b) –Akiyosji D., et al., 53rd ICAAC, 2013, Denver, CO, (abstract F1701a)
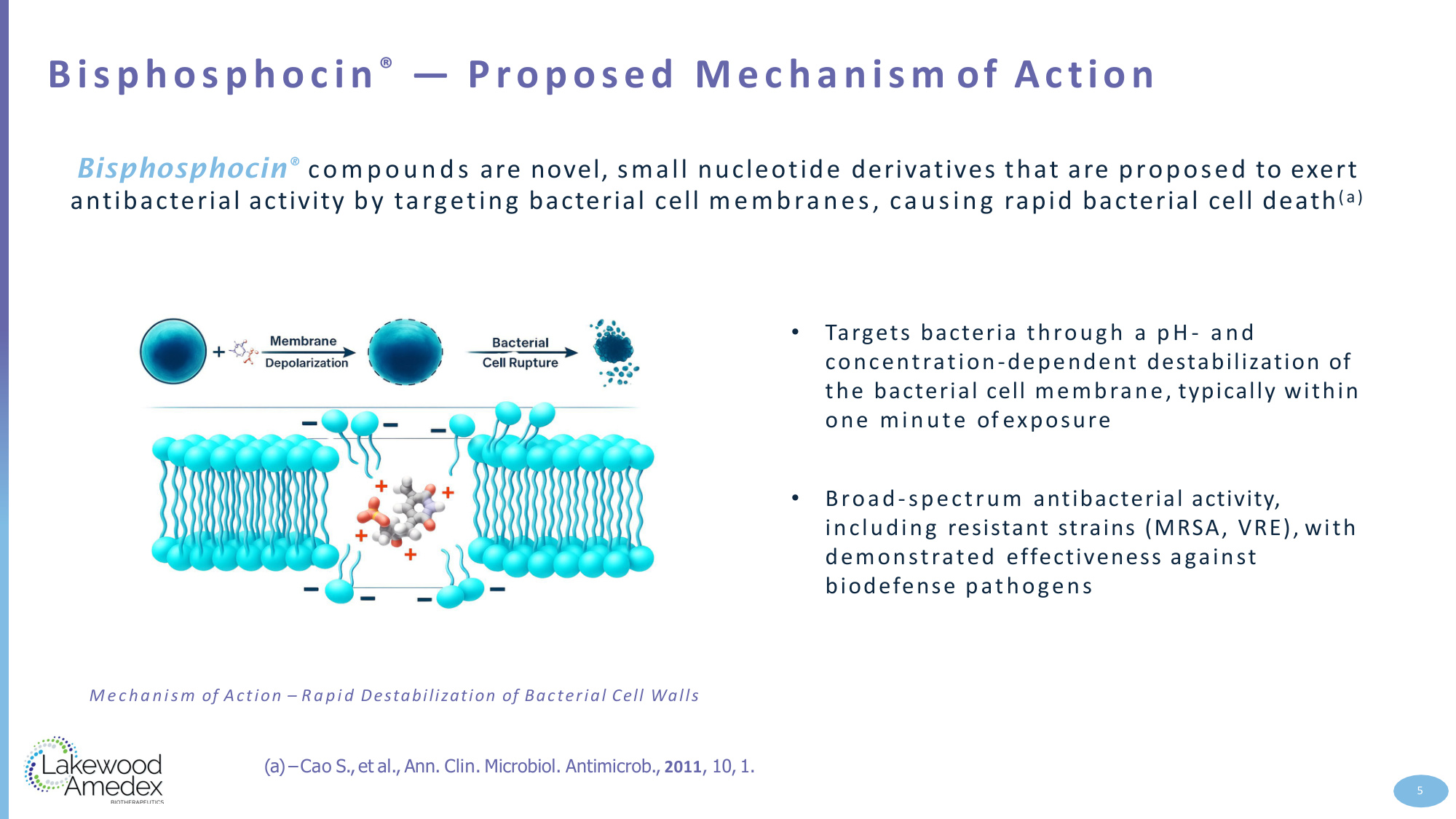
Bisphosphocin ® — Proposed Mechanism of Action • Targets bacteria through a pH- and concentration-dependent destabilization of the bacterial cell membrane, typically within one minute of exposure • Broad-spectrum antibacterial activity, including resistant strains (MRSA, VRE), with demonstrated effectiveness against biodefense pathogens Bisphosphocin® compounds are novel, small nucleotide derivatives that are proposed to exert antibacterial activity by targeting bacterial cell membranes, causing rapid bacterial cell death(a) 5 Mechanism of Action – Rapid Destabilization of Bacterial Cell Walls (a)–Cao S.,et al., Ann. Clin. Microbiol. Antimicrob., 2011, 10, 1.
Lead Program: Infected Diabetic Foot Ulcer (iDFU) 6 Global Prevalence • 830M people with diabetes;(a) about one third will develop a DFU ( b ) Infection Rate • ~50% of D FUs become infected; ma ny patients face recurrent events (b) Severe Ou tcomes • Infections are a critical risk factor for amputation, alongside the presence of peripheral arterial disease (b) Resistance Challenge • 15–20% of iDFUs involve resistant pathogens (primarily MRSA) (c) Treatment Shortcomings • Standard-of-care: systemic antibiotics and wound care — yet outcomes remain poor with high recurrence and amputation rates (a) WHO report on diabetes, 2024; (b) Armstrong D., et al., Diabetes Care, 1998, 21 (5), pp 855-859; (c)Zhou S., et al., Metabolic Syndrome and Obesity, 2024, 17, 563-574
Nu-3 Selected for Clinical Development ( a ) Broad spectrum in vitro; Nu-3 shown to be rapidly cidal against a broad spectrum of microbes, including resistant strains, with low potential for resistance development and activity against biofilm Robust efficacy in skin infection models; Nu-3 active as solution or gel formulation in single dose and multiple dose in vivo studies Formulation designed for local administration; Gel formulation developed as most appropriate dosage form for topical application Excellent safety profile toxicology program; minimal effects given at high doses both iv and topical safety studies O pe n IND; Nu-3 IND open and active (a)Cooper K, et al, AntimicrobialAgents and Chemotherapy, 2025, https://doi.org/10.1128/aac.00948-25 7
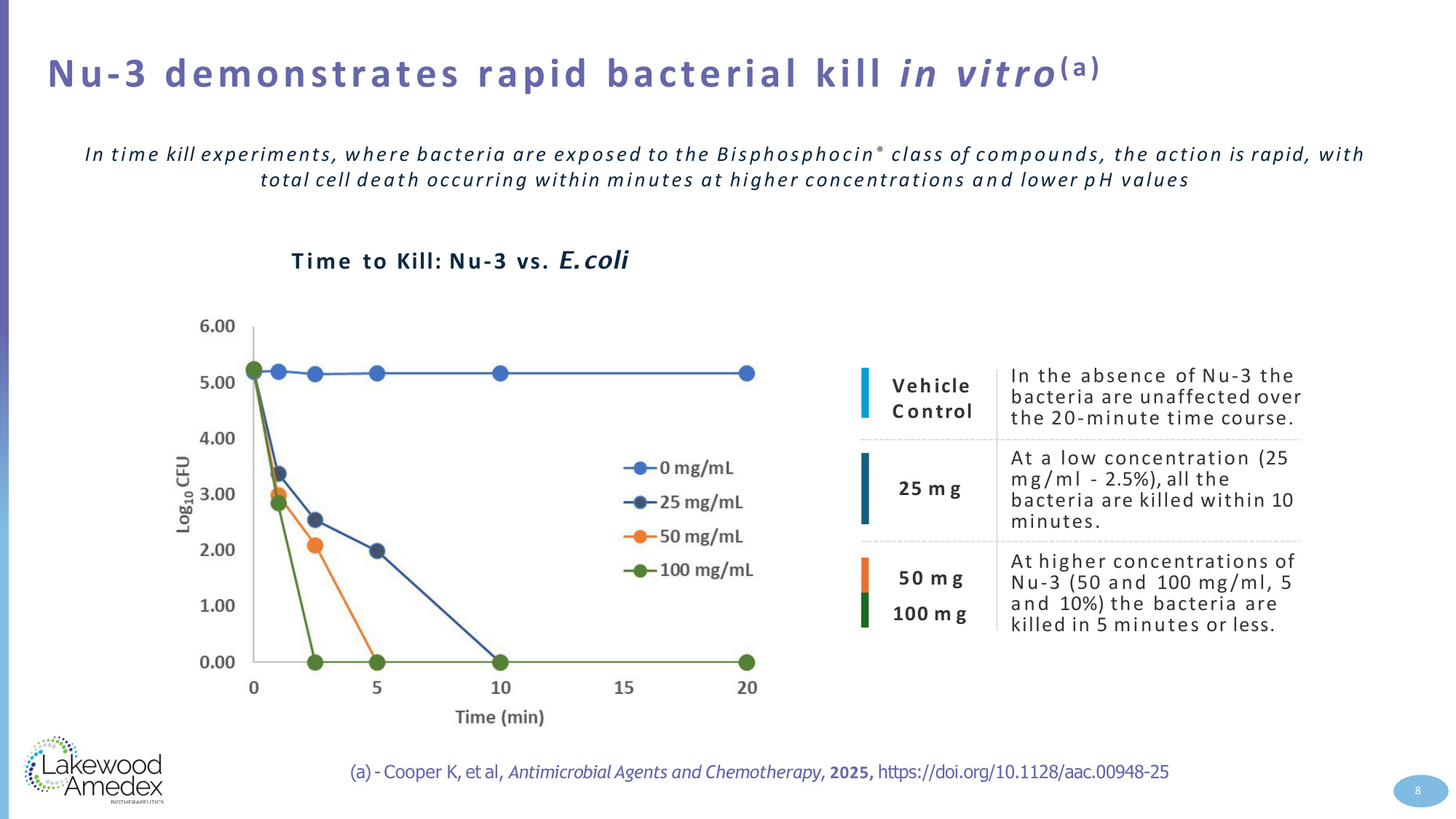
Nu-3 demonstrates rapid bacterial kill in vitro (a) In the absence of Nu-3 the bacteria are unaffected over the 20-minute time course. 25 m g Vehicle C ontrol At a low concentration (25 mg /ml - 2.5%), all the bacteria are killed within 10 minutes. 50 m g 100 m g At higher concentrations of Nu-3 (50 and 100 mg/ml, 5 and 10%) the bacteria are killed in 5 minutes or less. In time kill experiments, where bacteria are exposed to the Bisphosphocin ® class of compounds, the action is rapid, with total cell death occurring within minutes at higher concentrations a n d lower p H values Time to Kill: Nu-3 vs. E.coli (a)- Cooper K, et al, AntimicrobialAgents and Chemotherapy, 2025, https://doi.org/10.1128/aac.00948-25 8
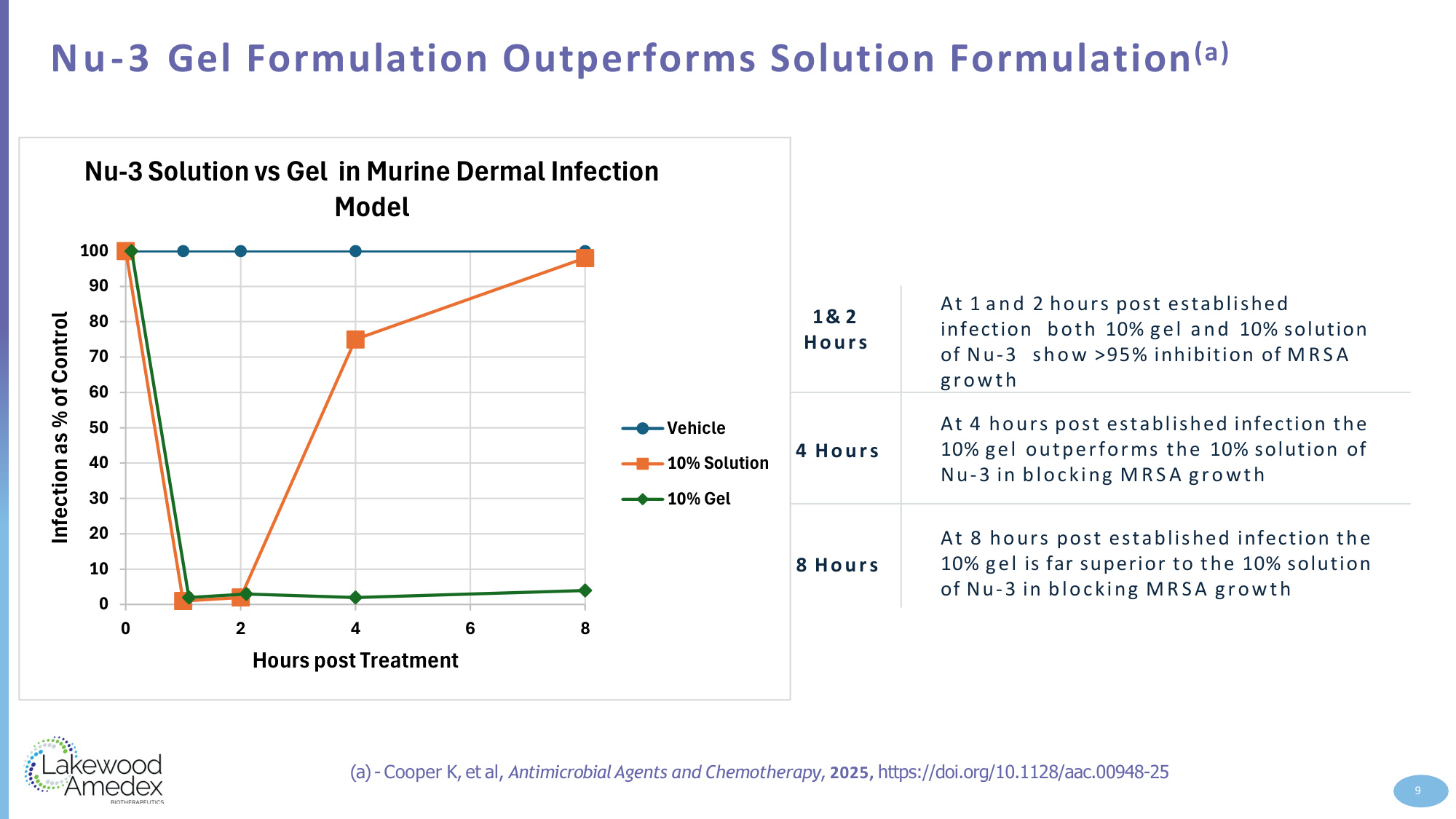
Nu-3 Gel Formulation Outperforms Solution Formulation(a) 1& 2 Hours At 1 and 2 hours post established infection both 10% gel and 10% solution of Nu-3 show >95% inhibition of MRSA growth 4 Hours At 4 hours post established infection the 10% gel outperforms the 10% solution of Nu-3 in blocking MRSA growth 8 Hours At 8 hours post established infection the 10% gel is far superior to the 10% solution of Nu-3 in blocking MRSA growth (a)- Cooper K, et al, AntimicrobialAgents and Chemotherapy, 2025, https://doi.org/10.1128/aac.00948-25 9 0 10 20 30 40 50 60 70 80 90 100 0 2 4 6 8 Infection as % of Control Hours post Treatment Nu-3 Solution vs Gel in Murine Dermal Infection Model Vehicle 10% Solution 10% Gel
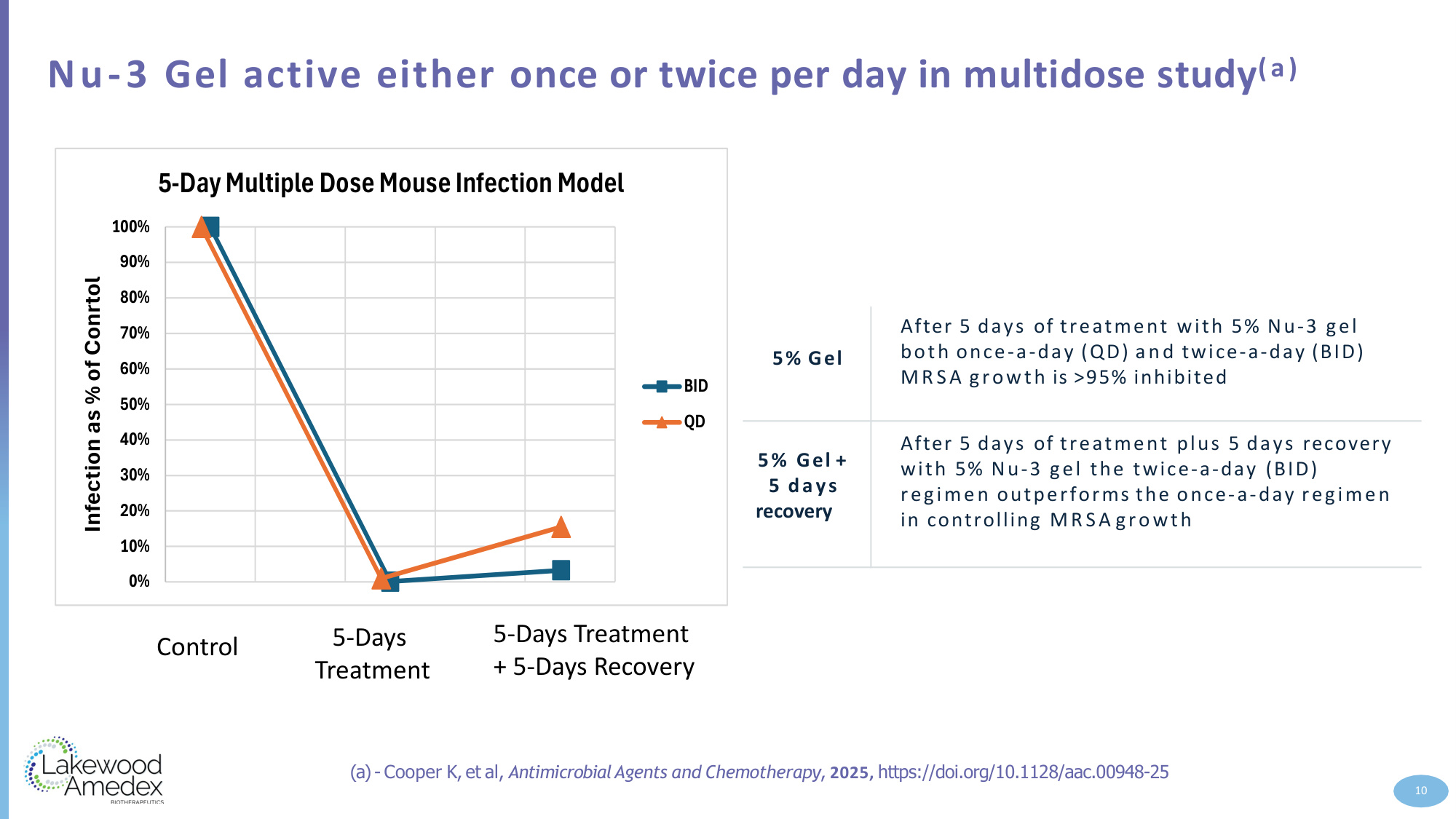
Nu-3 Gel active either once or twice per day in multidose study(a) 5% Gel After 5 days of treatment with 5% Nu-3 gel both once-a-day (QD) and twice-a-day (BID) MRSA growth is >95% inhibited 5% Gel + 5 days recovery After 5 days of treatment plus 5 days recovery with 5% Nu-3 gel the twice-a-day (BID) regimen outperforms the once-a-day regimen in controlling MRSA growth (a)- Cooper K, et al, AntimicrobialAgents and Chemotherapy, 2025, https://doi.org/10.1128/aac.00948-25 10 0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100% Infection as % of Conrtol 5-Day Multiple Dose Mouse Infection Model BID QD Control 5-Days Treatment 5-Days Treatment + 5-Days Recovery
Advantages of Bisphosphocin ® Class in Com bat ing AMR: based on available non-clinical evidence 11 Right Drug Right Application Right MOA
Clinical Evidence Supporting Development of Nu-3 • A 21‐Day Repeat Patch Test to Evaluate the Irritation Potential of Test Product (2% Nu‐3 in 0.85% Saline, W/V) on Abraded and Intact Skin Sites with Controls • 35 healthy subjects exposed • Abraded skin: Positive control > 2% Nu‐3 > Negative saline solution control • Intact skin: Positive control > 2% Nu‐3 = Negative saline solution control • Double blinded, randomized, dose‐escalating • Doses of Nu‐3 solution: 0.1%, 1% and 2 % or placebo (8:8:8:6 randomization) • 30 patients analyzed • Safety as primary endpoint • Efficacy secondary: pathogen reduction and ulcer surface area measurements 12 Phase 1 Patch Study Exploratory Phase 2a Study in Patients with iDFU
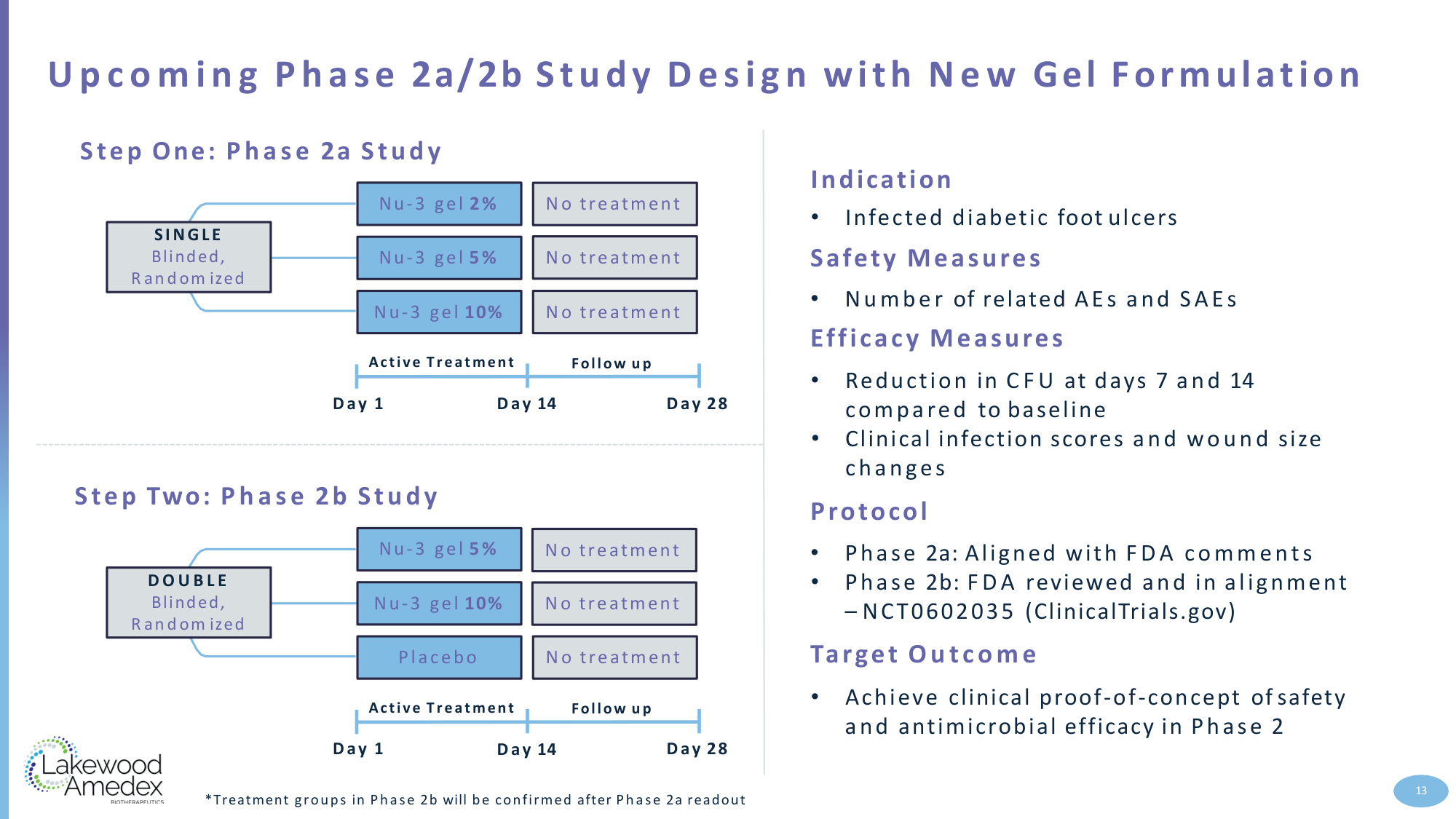
Step One: Phase 2a Study SINGLE Blinded, R an d om ized Nu-3 gel 2% Nu-3 gel 5% Nu-3 gel 10% Active Treatment D ay 1 Day 14 Day 28 Follow u p N o treatment N o treatment N o treatment Step Two: Phase 2b Study 13 U p c o m i n g Phase 2a/2b Study Design with N e w Gel Formulation Indication • Infected diabetic foot ulcers Safety Measures • Number of related AEs and SAEs Efficacy Measures • Reduction in C F U at days 7 and 14 compared to baseline • Clinical infection scores and wound size changes Protocol • Phase 2a: Aligned with F D A comments • Phase 2b: F D A reviewed and in alignment – NCT0602035 (ClinicalTrials.gov) Target Outcome • Achieve clinical proof-of-concept of safety and antimicrobial efficacy in Phase 2 *Treatment groups in Phase 2b will be confirmed after Phase 2a readout D O U B L E Blinded, R an d om ized Nu-3 gel 5% Nu-3 gel 10% Placebo Active Treatment D ay 1 Day 14 Day 28 Follow u p N o treatment N o treatment N o treatment

iDFU Development and Regulatory Strategy 14 Geographic Scope • Phase 2 U.S.development • Phase 3 International development Clinical Development • 2 small accessory studies full pharmacokinetic and skin sensitization • E n d of Phase 2 Meeting • Phase 3: In partnership to attain global reach and capabilities o Active comparator trial(s) o Longer follow-up in Phase 3 to establish clinical utility on wound healing (Performance + Utility) Manufacturing Final Formulation at end of Phase 2 • Defining the commercial application for Phase 3 • Application system will determine drug or combination drug-device development path
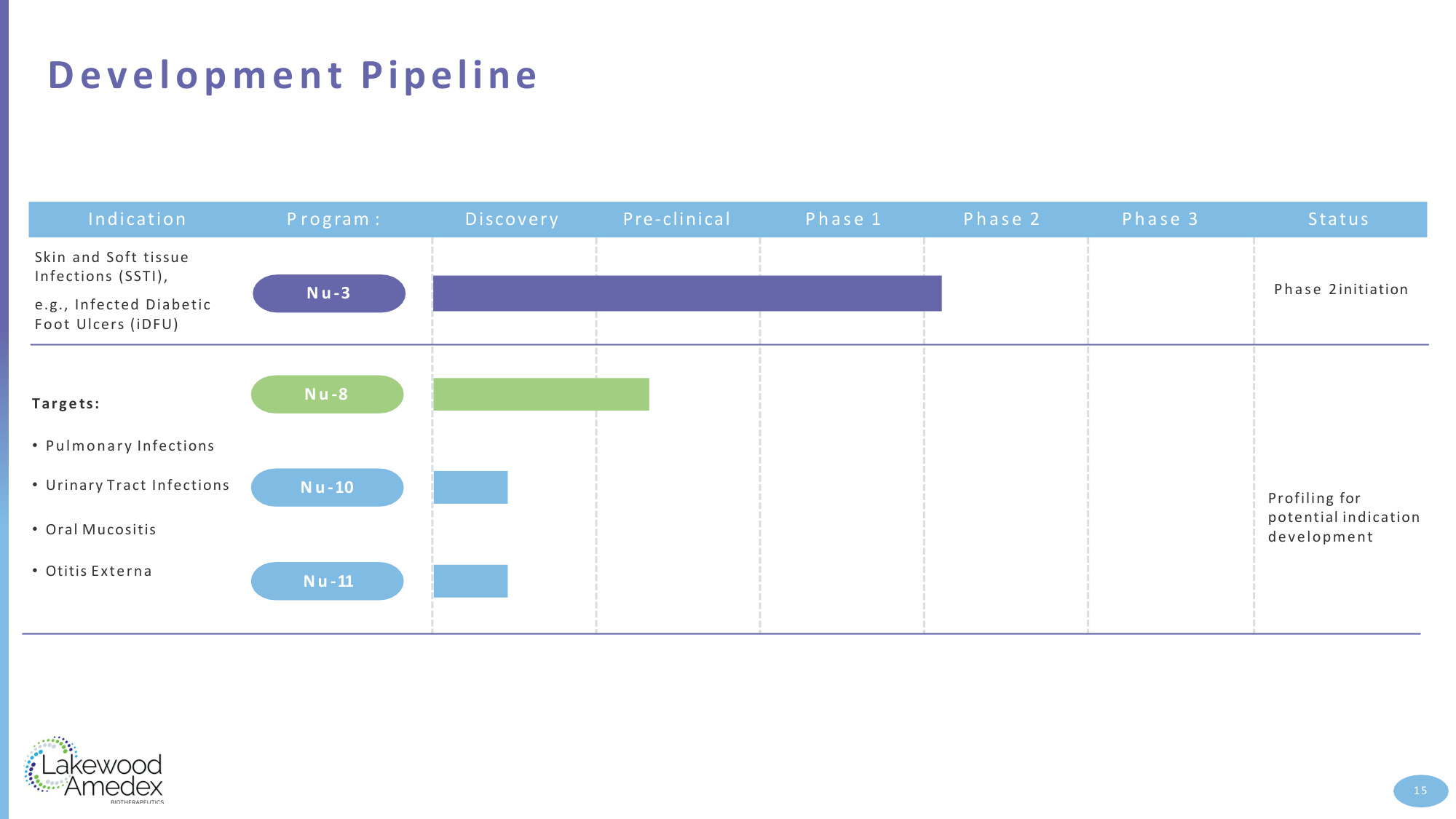
N u -3 N u -8 N u -11 N u -10 Indication P rogram : Discovery Pre-clinical Phase 1 Phase 2 Phase 3 Status Targe ts: • Pulmonary Infections • Urinary Tract Infections • Oral Mucositis • Otitis Externa Skin and Soft tissue Infections (SSTI), e.g., Infected Diabetic Foot Ulcers (iDFU) Phase 2initiation Profiling for potential indication development Development Pipeline 15

Upcoming Milestones 2Q26 • Drug product manufacturing initiated • Site enrollment initiated 16 3Q26 • Drug product manufacturing completed • Site enrollment completed • Clinical Trial Commences • First Patient First Visit 4Q26 • Clinical Trial Complete • Last Patient Last Visit 4Q26/1Q27 • Top Line Results
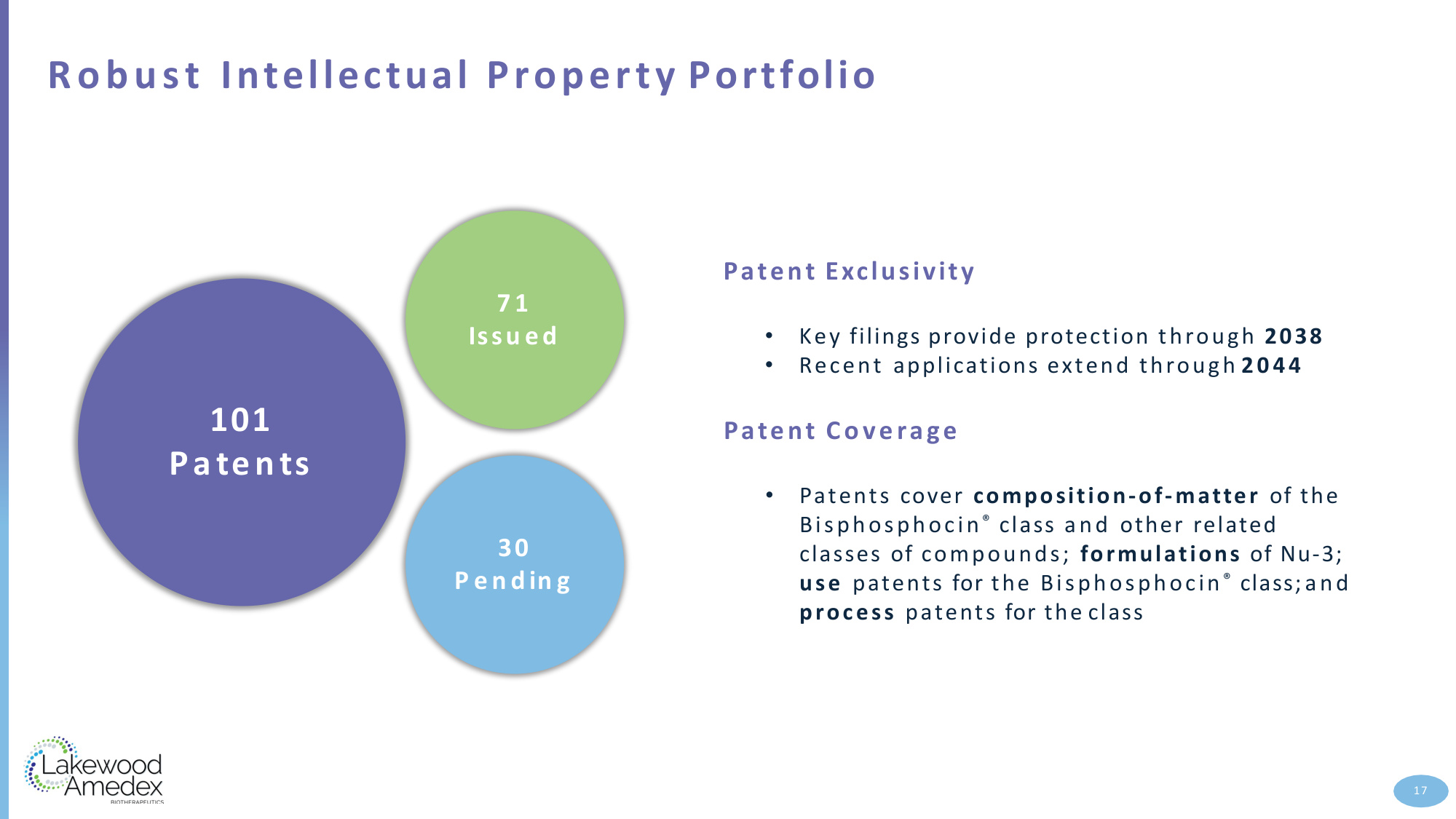
Robust Intellectual Property Portfolio 71 Issu ed 30 P e ndin g 101 Patents 17 Patent Exclusivity • Key filings provide protection through 2038 • Recent applications extend through 2044 Patent Coverage • Patents cover composition-of-matter of the Bisphosphocin ® class and other related classes of compounds; formulations of Nu-3; use patents for the Bisphosphocin ® class; and process patents for the class
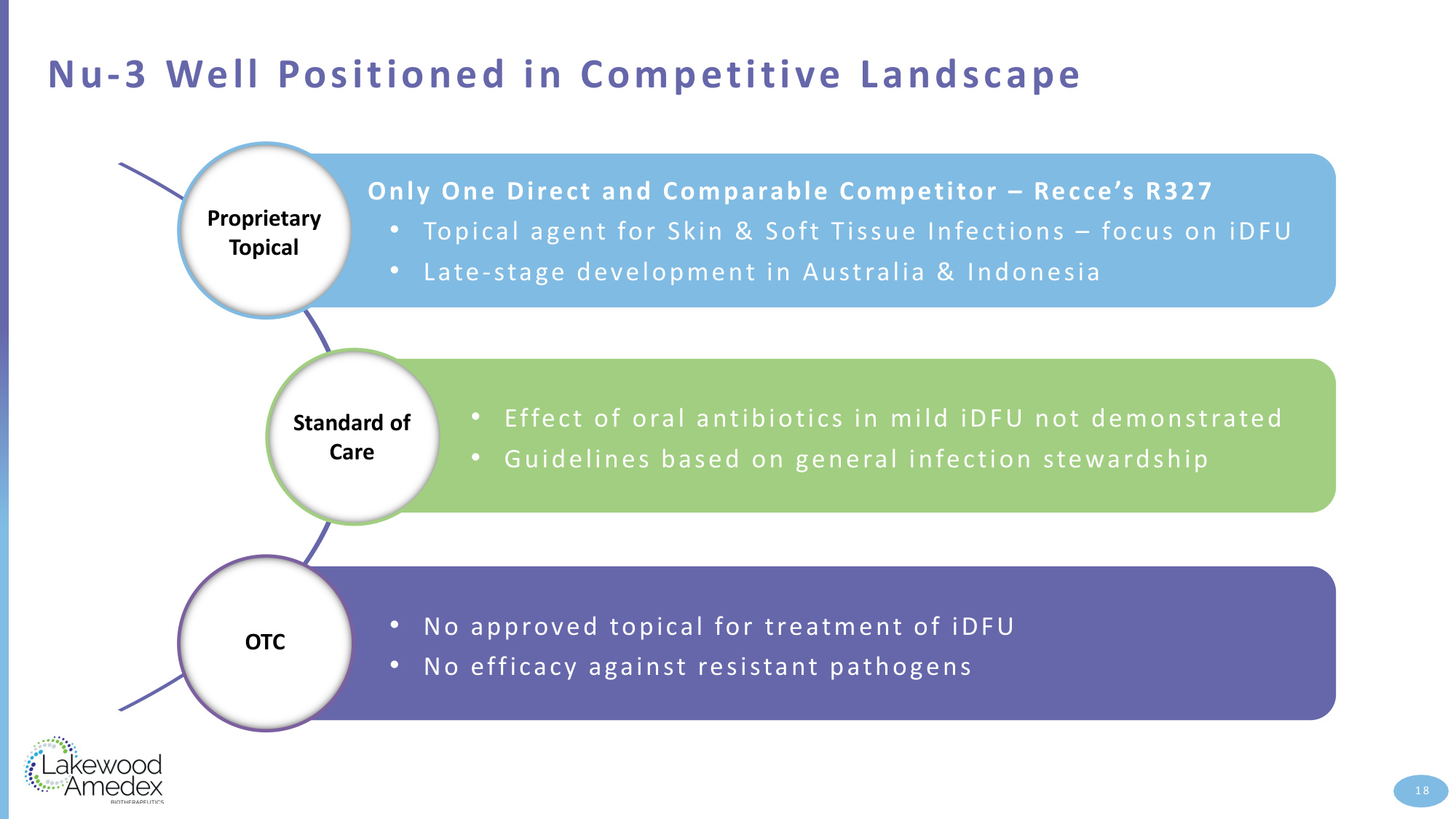
Nu-3 Well Positioned in Competitive Landscape 18 Only One Direct and Comparable Competitor – Recce's R327 • Topical agent for Skin & Soft Tissue Infections – focus on iDFU • Late-stage development in Australia & Indonesia • No approved topical for treatment of iDFU • No efficacy against resistant pathogens Proprietary Topical Standard of Care OTC • Effect of oral antibiotics in mild iDFU not demonstrated • Guidelines based on general infection stewardship

Experienced Management with Industry Depth Kelvin Cooper, Ph.D. Chief Executive Officer • 45 Years in the Pharmaceutical Industry • 30 years at Pfizer • Executive Leadership roles in D r u g Discovery, D r u g Development, Manufacturing, and Commercial Peter C e c ca c c i Chief Financial Officer • More than 25 years of experience as a Senior Executive with comprehensive experience in accounting, finance, strategy, compliance, and m a n a g e m e n t T h o m a s Balzer, M.D., Ph.D. Chief Medical Officer • 30 Years in the Pharmaceutical Industry at Schering AG, Bayer US, Exact Sciences • Executive Leadership roles in Global Clinical Development and Global Medical Affairs at Bayer U S L eadership B o ard Kelvin Cooper, Ph.D. Chief Executive Officer L eonard J. D e R o m a Director D o u g Manion, M.D., F RC P ( C ) Chairman J o s e p h Tucker, Ph.D. Director 19

Pioneering Innovations to Com bat Drug-Resistant Infections Clinical-stage biotechnology co m p a ny developing a novel class of fast-acting, broad-spectrum antimicrobials — Bisphosphocin ® comp ou n d s — to treat infectious diseases a n d reduce the threat posed by antibiotic-resistant microbes Phase 2-ready lead product, Nu-3, is a topically delivered antimicrobial gel for the treatment of infected diabetic foot ulcers (iDFU) Pre-clinical or early clinical data demonstrate broad, fast-acting activity (incl. resistant strains) with low resistance risk, a favorable safety profile, and effective local action Potential first-in-class infection therapy for the treatment of iDFU Near-term milestones include the initiation of a planned Phase 2a clinical trial evaluating the safety and efficacy of Nu-3 in iDFU Robust intellectual property estate with key filings providing protection through 2038 and recent applications extending through 2044 20

21