
Exhibit 99.2 Neoadjuvant BOT+BAL in MSS Colon Cancer Agenus PIPE Financing Announcement July 13, 2026

Agenus Speakers Garo H. Armen, PhD Robin Taylor, PhD Steven O’Day, MD Zack Armen Founder, Chairman & CEO Chief Commercial Officer Chief Medical Officer VP, Corporate Dev & IR 2

Industry Thought Leaders Professor Myriam Chalabi, MD Pashtoon Kasi, MD, MS Medical Oncologist Medical Oncologist Netherlands Cancer Institute, Amsterdam NL Rad Family Chair in Gastrointestinal Oncology 2026 Innovators in Science Award City of Hope, Irvine CA 3
Forward-Looking Statements This presentation contains forward-looking statements that are made pursuant to the safe harbor provisions of the federal securities laws. These forward- looking statements include, but are not limited to, express or implied statements relating to the Company’s expectations, hopes, beliefs, intentions or strategies regarding the future of its pipeline and business; the Company’s strategic prioritization of BOT+BAL for the neoadjuvant treatment of MSS colon cancer; the potential benefits of treatment with the Company’s product candidates, including without limitation BOT+BAL and the Company’s other balstilimab, botensilimab, zalifrelimab, AGEN1777, AGEN2373 and AGEN1571 programs; the timing of the regulatory submission, design, enrollment, indication selection, dosing, timing of initiation, progress and timing of readouts and results of the Company’s ongoing and planned clinical trials, including without limitation the Company’s Phase 2 NEST and UNICORN trials and the Company’s planned Phase 3 ROBBIN trial; anticipated safety, efficacy, potency, activity, superior response and durability outcomes with respect to the Company’s ongoing and planned clinical trials; the Company’s plans to discontinue financial support for the ongoing BATTMAN Phase 3 trial; expected regulatory timelines and filings; the Company’s commercialization plans and anticipated commercial market opportunities (including partnering and licensing opportunities); the Company’s ability to meet manufacturing demands; the closing of the Private Placement; the Company’s agreement to register the resale of the securities sold in the Private Placement; the expected amount of proceeds from the Private Placement; and the Company’s anticipated cash runway. Statements containing the words may, believes, expects, anticipates, hopes, intends, plans, will, “potential,” or the negative of these terms and other similar words or expressions, are intended to identify forward-looking statements, although not all forward- looking statements contain these identifying words. These forward-looking statements are subject to risks and uncertainties that could cause actual results to differ materially from those expressed or implied in any forward-looking statement. These risks and uncertainties include, among others, the factors described under the Risk Factors section of Annual Report on Form 10-K for the fiscal year ended December 31, 2025, and our subsequent Quarterly Reports on Form 10- Q filed with the Securities and Exchange Commission and made available on our website at www.agenusbio.com. Agenus cautions investors not to place considerable reliance on the forward-looking statements contained in this presentation. Agenus makes no express or implied representation or warranty as to the completeness of forward-looking statements or, in the case of projections, as to their attainability or the accuracy and completeness of the assumptions from which they are derived. These statements speak only as of the date of this presentation, and Agenus undertakes no obligation to update or revise the statements, other than to the extent required by law. All forward-looking statements are expressly qualified in their entirety by this cautionary statement. Information that may be important to investors will be routinely posted on our website and social media channels. 4
Welcome Garo Armen, Ph.D. Founder, Chairman & CEO 5
Fully Funded, FDA-aligned Phase 3 Trial Testing Neoadjuvant BOT+BAL in MSS Colon Cancer, a Multi Billion-Dollar Opportunity in the US • Financing of $85M upfront and up to $340M in total, focused on BOT+BAL opportunity in high-risk Stage II 1 and Stage III MSS Colon Cancer, >$7 Billion TAM in the US • Capital will be directed to an FDA-aligned pivotal Phase 3 study (“ROBBIN”) of neoadjuvant BOT+BAL for MSS Colon Cancer (n=850, Randomized 1:1, Primary Endpoint EFS) • To focus company resources, Agenus is discontinuing support for the ongoing BATTMAN Phase 3 study • Key upcoming catalysts for ROBBIN Phase 3 Trial (Neoadjuvant BOT+BAL): • ROBBIN first patient dosed: anticipated Q1 of 2027 • Interim pathologic response data: anticipated second half of 2027 • Interim analysis of EFS: anticipated second half of 2029 • Final analysis of EFS: anticipated second half of 2030 1. Epidemiology analysis based on data from SEER, CDC, and Clarivate; assumes 38,000 eligible patient population annually * $200K for a course of neoadjuvant treatment. 6
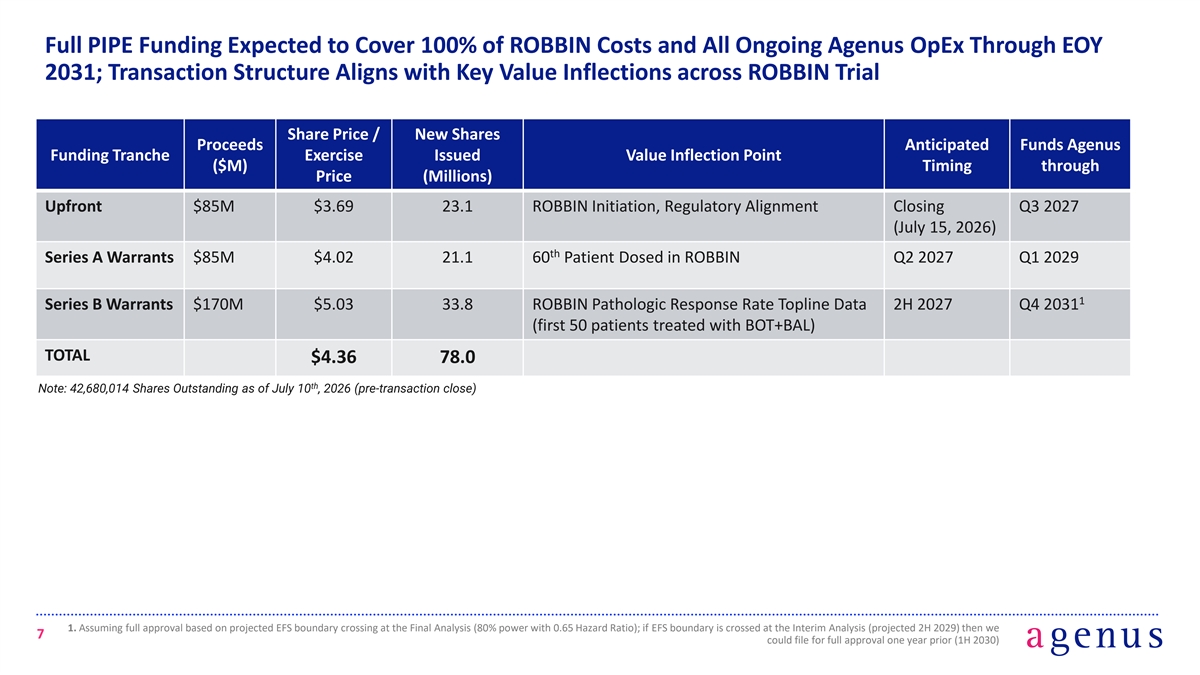
Full PIPE Funding Expected to Cover 100% of ROBBIN Costs and All Ongoing Agenus OpEx Through EOY 2031; Transaction Structure Aligns with Key Value Inflections across ROBBIN Trial Share Price / New Shares Proceeds Anticipated Funds Agenus Funding Tranche Exercise Issued Value Inflection Point ($M) Timing through Price (Millions) Upfront $85M $3.69 23.1 ROBBIN Initiation, Regulatory Alignment Closing Q3 2027 (July 15, 2026) th Series A Warrants $85M $4.02 21.1 60 Patient Dosed in ROBBIN Q2 2027 Q1 2029 1 Series B Warrants $170M $5.03 33.8 ROBBIN Pathologic Response Rate Topline Data 2H 2027 Q4 2031 (first 50 patients treated with BOT+BAL) TOTAL $4.36 78.0 th Note: 42,680,014 Shares Outstanding as of July 10 , 2026 (pre-transaction close) 1. Assuming full approval based on projected EFS boundary crossing at the Final Analysis (80% power with 0.65 Hazard Ratio); if EFS boundary is crossed at the Interim Analysis (projected 2H 2029) then we 7 could file for full approval one year prior (1H 2030)
Colorectal Cancer (CRC) Faces Two Urgent Challenges: Rising Burden of Disease and Limited Innovation – Especially in Microsatellite Stable (MSS) Disease Most CRC lacks effective 1 Rising CRC Burden 2 immunotherapy options • Colorectal cancer (CRC) is now the • Microsatellite stable (MSS) accounts 5,6 leading cause of cancer-related death for ~85% of early-stage CRC cases 1 among Americans under 50 • No major advances in treatment of 2 6 • ~155,000 new cases annually in U.S. MSS colon cancer in >20 years 3 • ~2M new cases annually worldwide • MSS CRC remains unaddressed by 6 first-generation ICI 1. Siegel RL, et al. JAMA. 2026;335(7):632-634. 2. Siegel RL, et al. CA Cancer J Clin. 2025;75(1):10-45. 3. Bray F, et al. CA Cancer J Clin. 2024;74(3):229-263. 4. National Cancer Institute. SEER Cancer Stat Facts: 8 Colorectal Cancer. Bethesda, MD: National Cancer Institute. Available at: https://seer.cancer.gov/statfacts/html/colorect.html. 5. Buchler T. Front Oncol. 2022;12:888181. 6. Guven DC, et al. Oncologist. 2024;29(5):e580-e600.
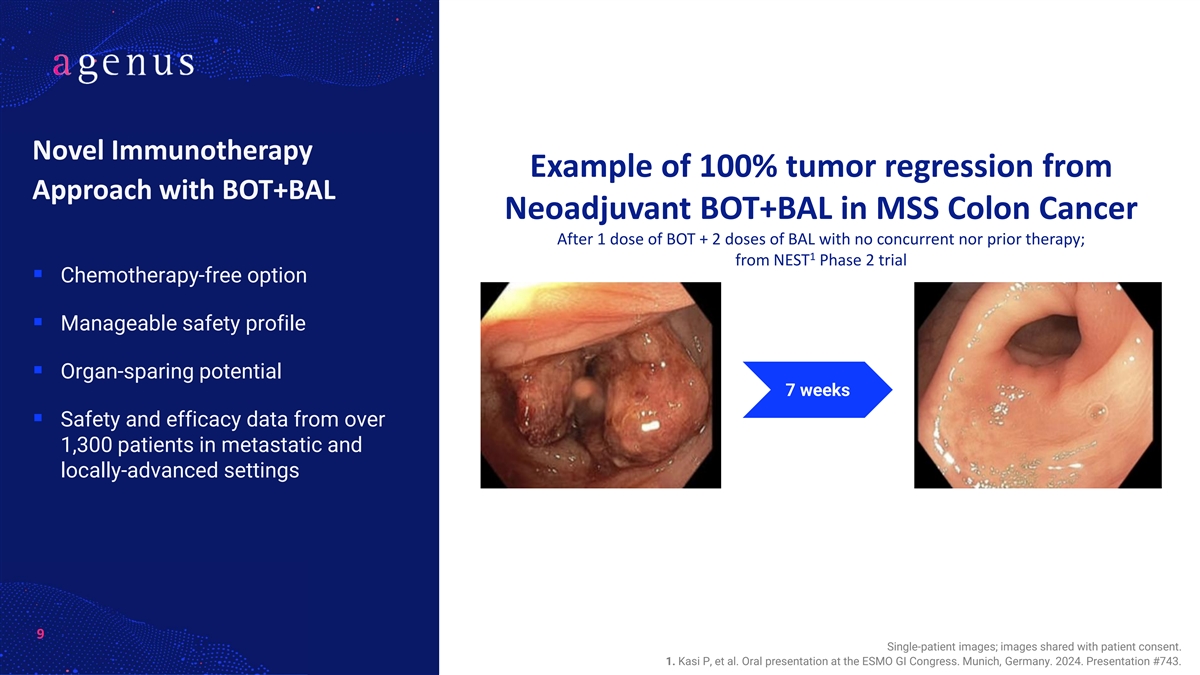
Novel Immunotherapy Example of 100% tumor regression from Approach with BOT+BAL Neoadjuvant BOT+BAL in MSS Colon Cancer After 1 dose of BOT + 2 doses of BAL with no concurrent nor prior therapy; 1 from NEST Phase 2 trial ▪ Chemotherapy-free option ▪ Manageable safety profile ▪ Organ-sparing potential 7 weeks ▪ Safety and efficacy data from over 1,300 patients in metastatic and locally-advanced settings 9 Single-patient images; images shared with patient consent. 1. Kasi P, et al. Oral presentation at the ESMO GI Congress. Munich, Germany. 2024. Presentation #743. CONFIDENTIAL
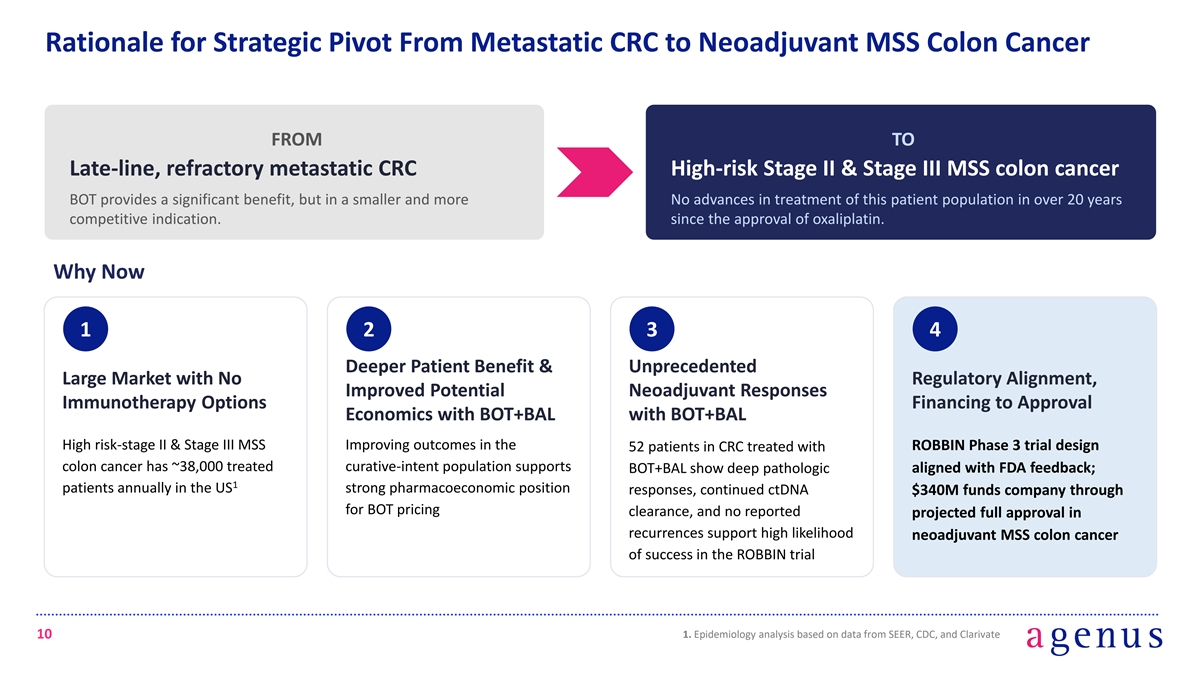
Rationale for Strategic Pivot From Metastatic CRC to Neoadjuvant MSS Colon Cancer FROM TO Late-line, refractory metastatic CRC High-risk Stage II & Stage III MSS colon cancer BOT provides a significant benefit, but in a smaller and more No advances in treatment of this patient population in over 20 years competitive indication. since the approval of oxaliplatin. Why Now 1 2 3 4 Deeper Patient Benefit & Unprecedented Large Market with No Regulatory Alignment, Improved Potential Neoadjuvant Responses Immunotherapy Options Financing to Approval Economics with BOT+BAL with BOT+BAL High risk-stage II & Stage III MSS Improving outcomes in the ROBBIN Phase 3 trial design 52 patients in CRC treated with colon cancer has ~38,000 treated curative-intent population supports aligned with FDA feedback; BOT+BAL show deep pathologic 1 patients annually in the US strong pharmacoeconomic position responses, continued ctDNA $340M funds company through for BOT pricing clearance, and no reported projected full approval in recurrences support high likelihood neoadjuvant MSS colon cancer of success in the ROBBIN trial 1. Epidemiology analysis based on data from SEER, CDC, and Clarivate 10
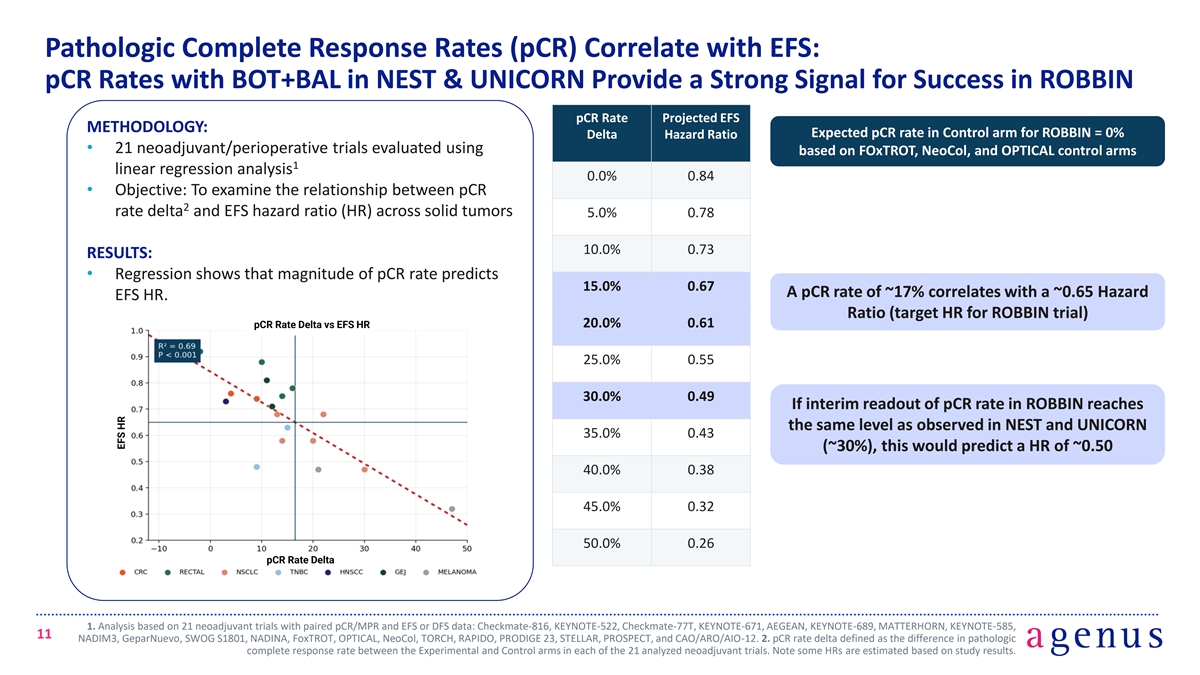
Pathologic Complete Response Rates (pCR) Correlate with EFS: pCR Rates with BOT+BAL in NEST & UNICORN Provide a Strong Signal for Success in ROBBIN pCR Rate Projected EFS METHODOLOGY: Expected pCR rate in Control arm for ROBBIN = 0% Delta Hazard Ratio • 21 neoadjuvant/perioperative trials evaluated using based on FOxTROT, NeoCol, and OPTICAL control arms 1 linear regression analysis 0.0% 0.84 • Objective: To examine the relationship between pCR 2 rate delta and EFS hazard ratio (HR) across solid tumors 5.0% 0.78 10.0% 0.73 RESULTS: • Regression shows that magnitude of pCR rate predicts 15.0% 0.67 A pCR rate of ~17% correlates with a ~0.65 Hazard EFS HR. Ratio (target HR for ROBBIN trial) 20.0% 0.61 pCR Rate Delta vs EFS HR 25.0% 0.55 30.0% 0.49 If interim readout of pCR rate in ROBBIN reaches the same level as observed in NEST and UNICORN 35.0% 0.43 (~30%), this would predict a HR of ~0.50 40.0% 0.38 45.0% 0.32 50.0% 0.26 pCR Rate Delta 1. Analysis based on 21 neoadjuvant trials with paired pCR/MPR and EFS or DFS data: Checkmate-816, KEYNOTE-522, Checkmate-77T, KEYNOTE-671, AEGEAN, KEYNOTE-689, MATTERHORN, KEYNOTE-585, 11 NADIM3, GeparNuevo, SWOG S1801, NADINA, FoxTROT, OPTICAL, NeoCol, TORCH, RAPIDO, PRODIGE 23, STELLAR, PROSPECT, and CAO/ARO/AIO-12. 2. pCR rate delta defined as the difference in pathologic complete response rate between the Experimental and Control arms in each of the 21 analyzed neoadjuvant trials. Note some HRs are estimated based on study results. EFS HR
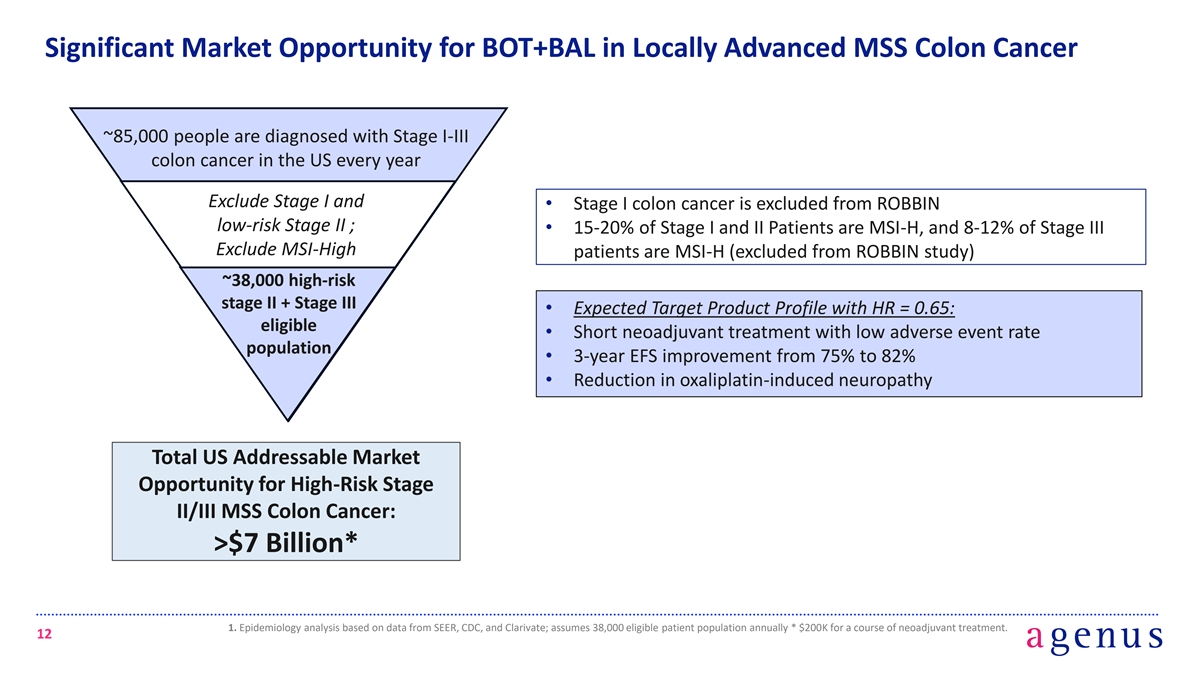
Significant Market Opportunity for BOT+BAL in Locally Advanced MSS Colon Cancer ~85,000 people are diagnosed with Stage I-III colon cancer in the US every year Exclude Stage I and • Stage I colon cancer is excluded from ROBBIN low-risk Stage II ; • 15-20% of Stage I and II Patients are MSI-H, and 8-12% of Stage III Exclude MSI-High patients are MSI-H (excluded from ROBBIN study) ~38,000 high-risk stage II + Stage III • Expected Target Product Profile with HR = 0.65: eligible • Short neoadjuvant treatment with low adverse event rate population • 3-year EFS improvement from 75% to 82% • Reduction in oxaliplatin-induced neuropathy Total US Addressable Market Opportunity for High-Risk Stage II/III MSS Colon Cancer: >$7 Billion* 1. Epidemiology analysis based on data from SEER, CDC, and Clarivate; assumes 38,000 eligible patient population annually * $200K for a course of neoadjuvant treatment. 12
Prior Neoadjuvant Studies in CRC: FOxTROT & NICHE Myriam Chalabi, MD Netherlands Cancer Institute, Amsterdam, NL 13
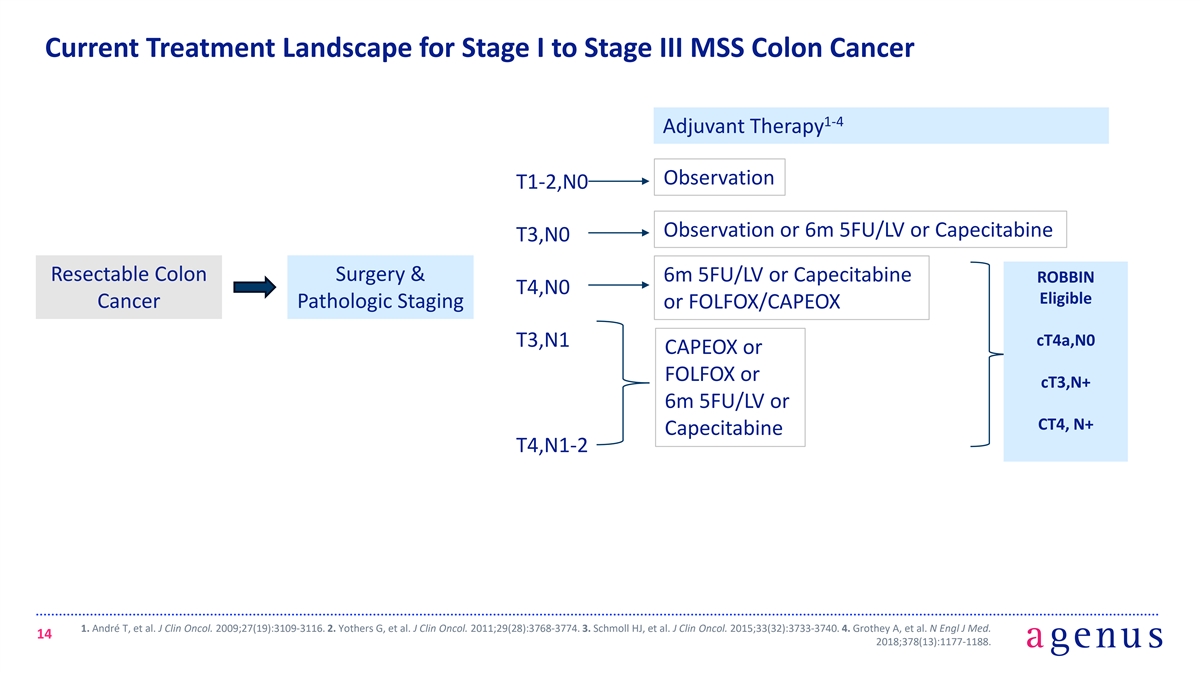
Current Treatment Landscape for Stage I to Stage III MSS Colon Cancer 1-4 Adjuvant Therapy Observation T1-2,N0 Observation or 6m 5FU/LV or Capecitabine T3,N0 Resectable Colon Surgery & 6m 5FU/LV or Capecitabine ROBBIN T4,N0 Eligible Cancer Pathologic Staging or FOLFOX/CAPEOX cT4a,N0 T3,N1 CAPEOX or FOLFOX or cT3,N+ 6m 5FU/LV or CT4, N+ Capecitabine T4,N1-2 1. André T, et al. J Clin Oncol. 2009;27(19):3109-3116. 2. Yothers G, et al. J Clin Oncol. 2011;29(28):3768-3774. 3. Schmoll HJ, et al. J Clin Oncol. 2015;33(32):3733-3740. 4. Grothey A, et al. N Engl J Med. 14 2018;378(13):1177-1188.
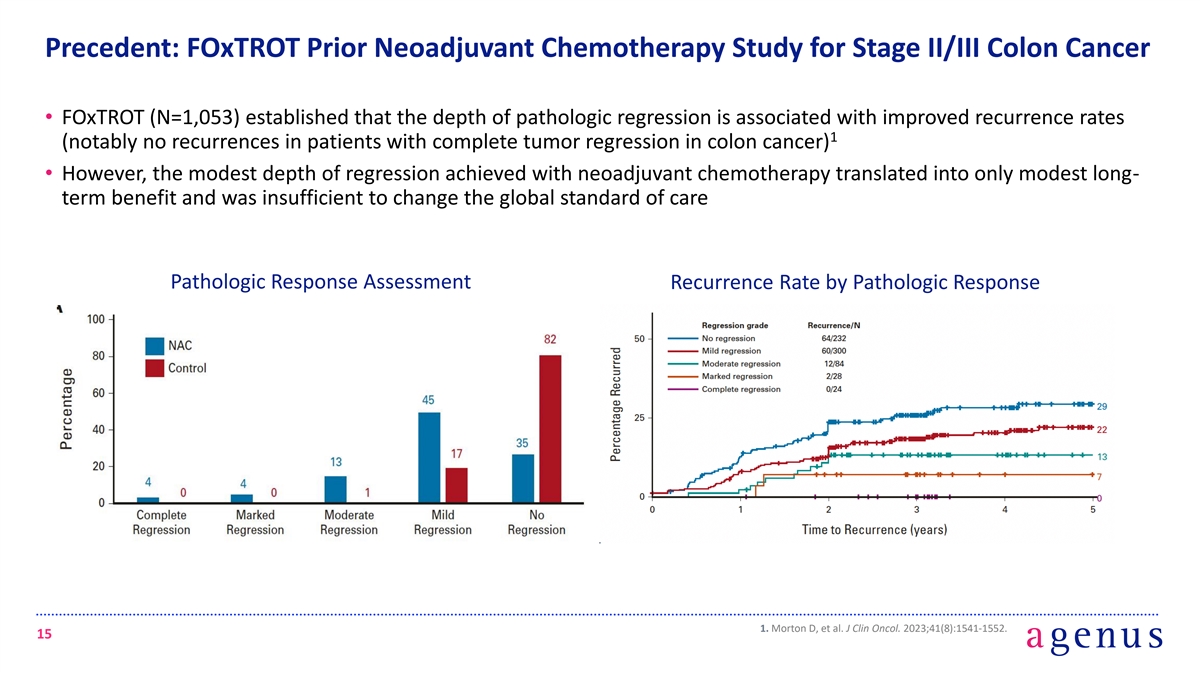
Precedent: FOxTROT Prior Neoadjuvant Chemotherapy Study for Stage II/III Colon Cancer • FOxTROT (N=1,053) established that the depth of pathologic regression is associated with improved recurrence rates 1 (notably no recurrences in patients with complete tumor regression in colon cancer) • However, the modest depth of regression achieved with neoadjuvant chemotherapy translated into only modest long- term benefit and was insufficient to change the global standard of care Pathologic Response Assessment Recurrence Rate by Pathologic Response 1. Morton D, et al. J Clin Oncol. 2023;41(8):1541-1552. 15
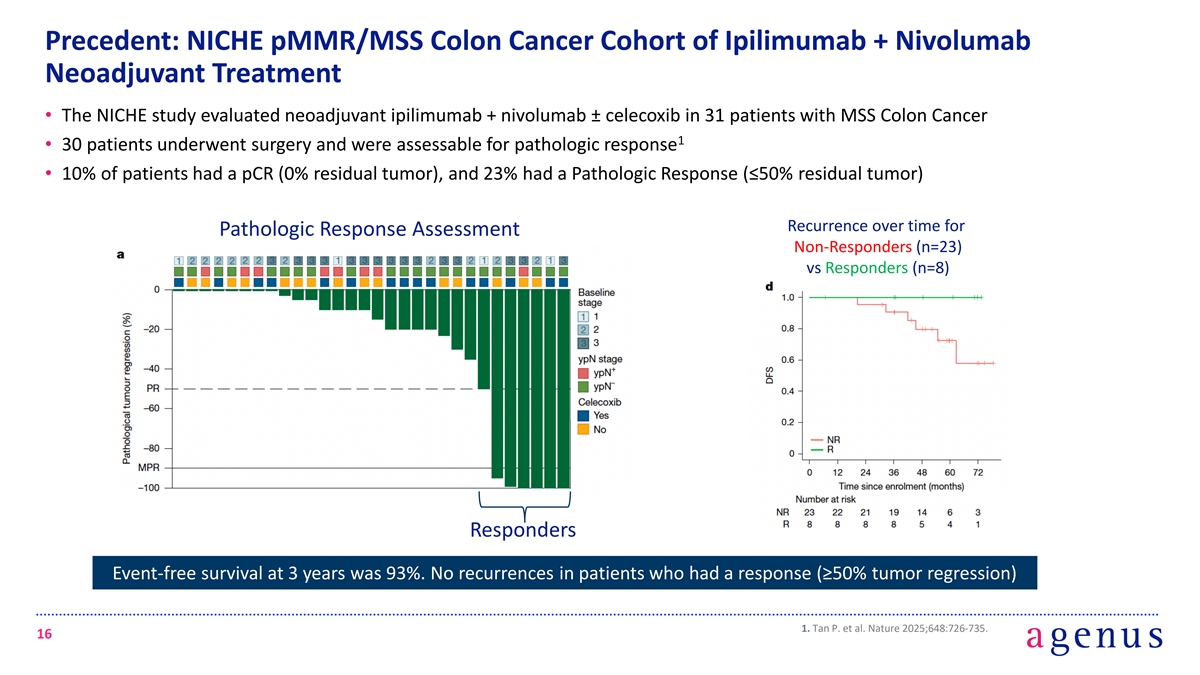
Precedent: NICHE pMMR/MSS Colon Cancer Cohort of Ipilimumab + Nivolumab Neoadjuvant Treatment • The NICHE study evaluated neoadjuvant ipilimumab + nivolumab ± celecoxib in 31 patients with MSS Colon Cancer 1 • 30 patients underwent surgery and were assessable for pathologic response • 10% of patients had a pCR (0% residual tumor), and 23% had a Pathologic Response (≤50% residual tumor) Recurrence over time for Pathologic Response Assessment Non-Responders (n=23) vs Responders (n=8) Responders Event-free survival at 3 years was 93%. No recurrences in patients who had a response (≥50% tumor regression) 1. Tan P. et al. Nature 2025;648:726-735. 16
NEST & UNICORN Phase 2 Studies of Neoadjuvant BOT + BAL Pashtoon Kasi, MD, MS City of Hope, Irvine, CA 17
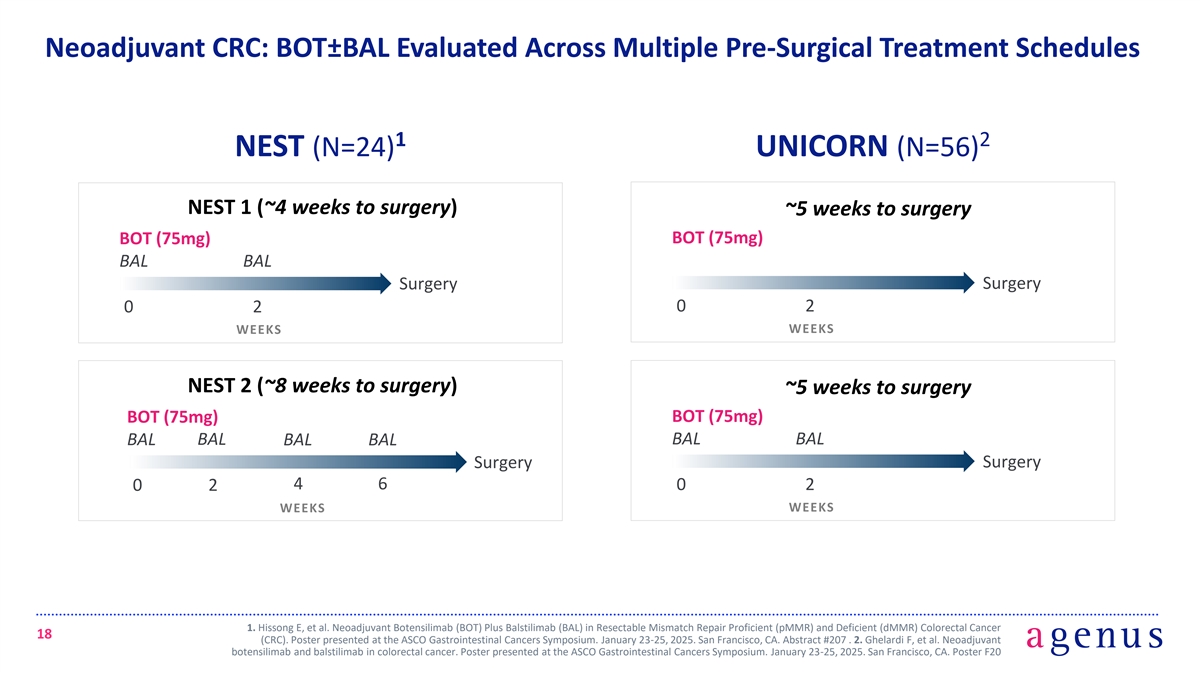
Neoadjuvant CRC: BOT±BAL Evaluated Across Multiple Pre-Surgical Treatment Schedules 1 2 NEST (N=24) UNICORN (N=56) NEST 1 (~4 weeks to surgery) ~5 weeks to surgery BOT (75mg) BOT (75mg) BAL BAL Surgery Surgery 0 2 0 2 WEEKS WEEKS NEST 2 (~8 weeks to surgery) ~5 weeks to surgery BOT (75mg) BOT (75mg) BAL BAL BAL BAL BAL BAL Surgery Surgery 4 6 0 2 0 2 WEEKS WEEKS 1. Hissong E, et al. Neoadjuvant Botensilimab (BOT) Plus Balstilimab (BAL) in Resectable Mismatch Repair Proficient (pMMR) and Deficient (dMMR) Colorectal Cancer 18 (CRC). Poster presented at the ASCO Gastrointestinal Cancers Symposium. January 23-25, 2025. San Francisco, CA. Abstract #207 . 2. Ghelardi F, et al. Neoadjuvant botensilimab and balstilimab in colorectal cancer. Poster presented at the ASCO Gastrointestinal Cancers Symposium. January 23-25, 2025. San Francisco, CA. Poster F20
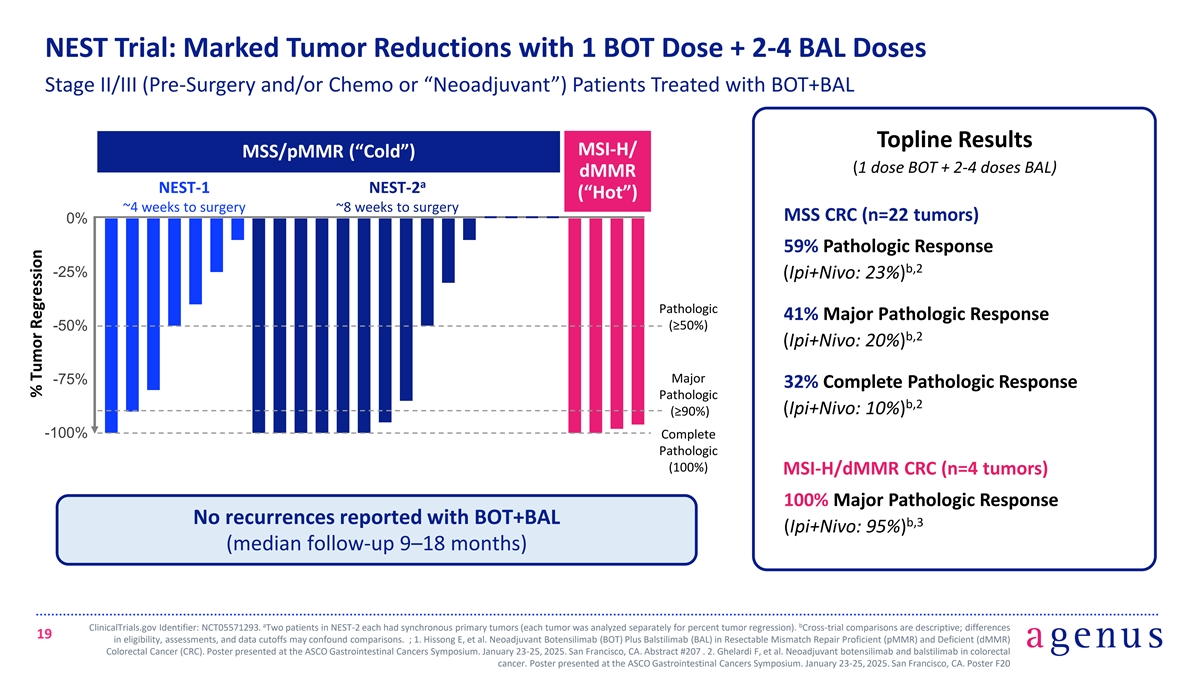
NEST Trial: Marked Tumor Reductions with 1 BOT Dose + 2-4 BAL Doses Stage II/III (Pre-Surgery and/or Chemo or “Neoadjuvant”) Patients Treated with BOT+BAL Topline Results MSI-H/ MSS/pMMR (“Cold”) (1 dose BOT + 2-4 doses BAL) dMMR a NEST-1 NEST-2 (“Hot”) ~4 weeks to surgery ~8 weeks to surgery MSS CRC (n=22 tumors) 0% 59% Pathologic Response b,2 -25% (Ipi+Nivo: 23%) Pathologic 41% Major Pathologic Response (≥50%) -50% b,2 (Ipi+Nivo: 20%) Major -75% 32% Complete Pathologic Response Pathologic b,2 (Ipi+Nivo: 10%) (≥90%) -100% Complete Pathologic (100%) MSI-H/dMMR CRC (n=4 tumors) 100% Major Pathologic Response No recurrences reported with BOT+BAL b,3 (Ipi+Nivo: 95%) (median follow-up 9–18 months) a b ClinicalTrials.gov Identifier: NCT05571293. Two patients in NEST-2 each had synchronous primary tumors (each tumor was analyzed separately for percent tumor regression). Cross-trial comparisons are descriptive; differences 19 in eligibility, assessments, and data cutoffs may confound comparisons. ; 1. Hissong E, et al. Neoadjuvant Botensilimab (BOT) Plus Balstilimab (BAL) in Resectable Mismatch Repair Proficient (pMMR) and Deficient (dMMR) Colorectal Cancer (CRC). Poster presented at the ASCO Gastrointestinal Cancers Symposium. January 23-25, 2025. San Francisco, CA. Abstract #207 . 2. Ghelardi F, et al. Neoadjuvant botensilimab and balstilimab in colorectal cancer. Poster presented at the ASCO Gastrointestinal Cancers Symposium. January 23-25, 2025. San Francisco, CA. Poster F20 . % Tumor Regression
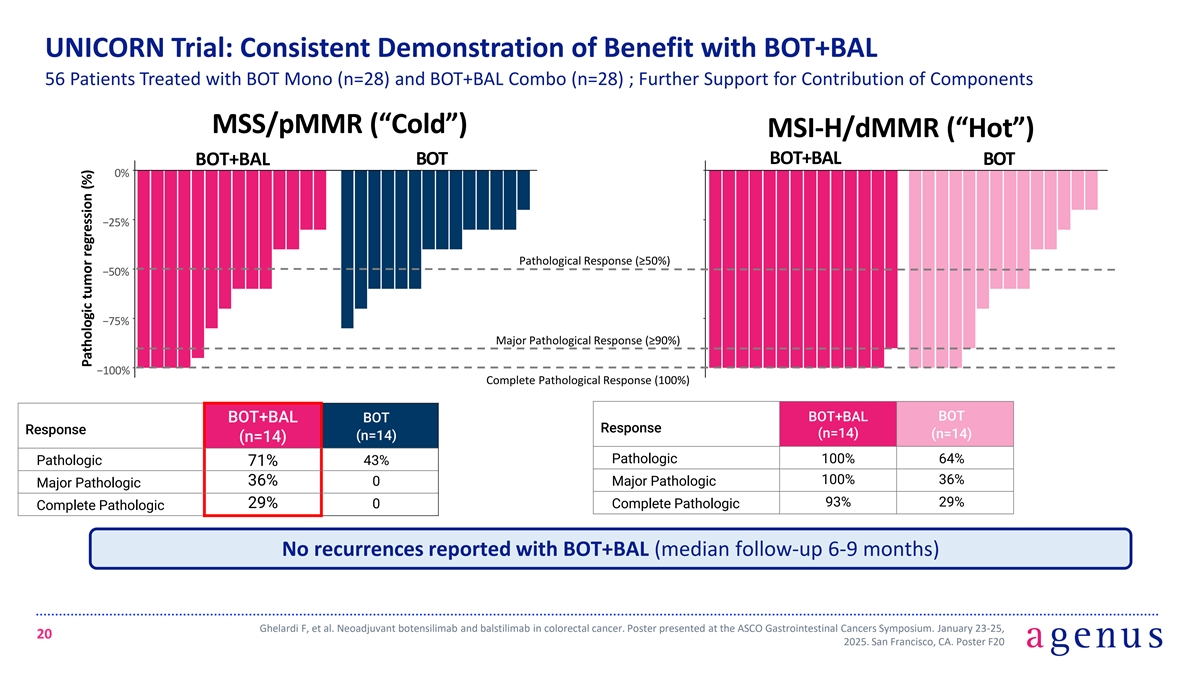
UNICORN Trial: Consistent Demonstration of Benefit with BOT+BAL 56 Patients Treated with BOT Mono (n=28) and BOT+BAL Combo (n=28) ; Further Support for Contribution of Components MSS/pMMR (“Cold”) MSI-H/dMMR (“Hot”) BOT+BAL BOT+BAL BOT BOT 0% −25% Pathological Response (≥50%) −50% −75% Major Pathological Response (≥90%) −100% Complete Pathological Response (100%) BOT+BAL BOT BOT+BAL BOT Response Response (n=14) (n=14) (n=14) (n=14) Pathologic 100% 64% Pathologic 43% 71% 100% 36% 36% 0 Major Pathologic Major Pathologic 93% 29% 29% 0 Complete Pathologic Complete Pathologic No recurrences reported with BOT+BAL (median follow-up 6-9 months) Ghelardi F, et al. Neoadjuvant botensilimab and balstilimab in colorectal cancer. Poster presented at the ASCO Gastrointestinal Cancers Symposium. January 23-25, 20 2025. San Francisco, CA. Poster F20 Pathologic tumor regression (%)
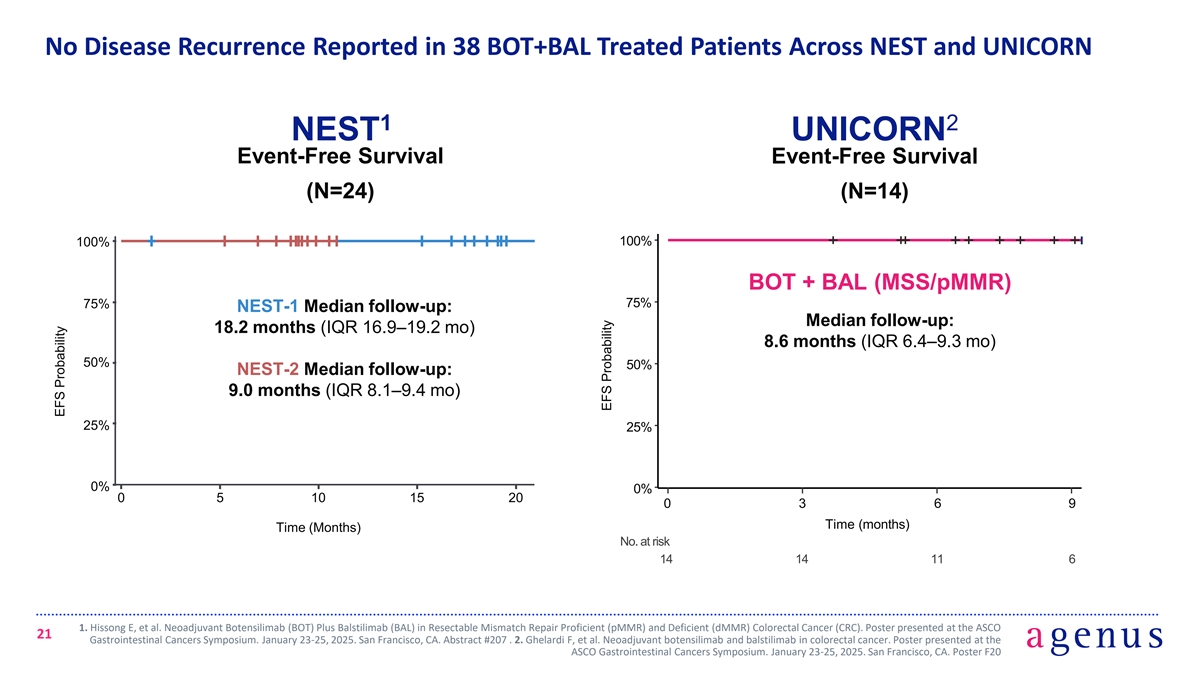
No Disease Recurrence Reported in 38 BOT+BAL Treated Patients Across NEST and UNICORN 1 2 NEST UNICORN Event-Free Survival Event-Free Survival (N=24) (N=14) 100% 100% BOT + BAL (MSS/pMMR) 75% 75% NEST-1 Median follow-up: Median follow-up: 18.2 months (IQR 16.9–19.2 mo) 8.6 months (IQR 6.4–9.3 mo) 50% 50% NEST-2 Median follow-up: 9.0 months (IQR 8.1–9.4 mo) 25% 25% 0% 0% 0 5 10 15 20 0 3 6 9 Time (months) Time (Months) No. at risk 14 14 11 6 1. Hissong E, et al. Neoadjuvant Botensilimab (BOT) Plus Balstilimab (BAL) in Resectable Mismatch Repair Proficient (pMMR) and Deficient (dMMR) Colorectal Cancer (CRC). Poster presented at the ASCO 21 Gastrointestinal Cancers Symposium. January 23-25, 2025. San Francisco, CA. Abstract #207 . 2. Ghelardi F, et al. Neoadjuvant botensilimab and balstilimab in colorectal cancer. Poster presented at the ASCO Gastrointestinal Cancers Symposium. January 23-25, 2025. San Francisco, CA. Poster F20 EFS Probability EFS Probability

No ctDNA Recurrences Observed in NEST NEST ctDNA Levels 100% 75% pre-surgical sample post-surgical sample 50% 25% 0% 0 100 200 300 400 500 Time post treatment (days) 1. Hissong E, et al. Neoadjuvant Botensilimab (BOT) Plus Balstilimab (BAL) in Resectable Mismatch Repair Proficient (pMMR) and Deficient (dMMR) Colorectal Cancer (CRC). Poster presented at the ASCO 22 Gastrointestinal Cancers Symposium. January 23-25, 2025. San Francisco, CA. Abstract #207 ctDNA (MTM/ml)
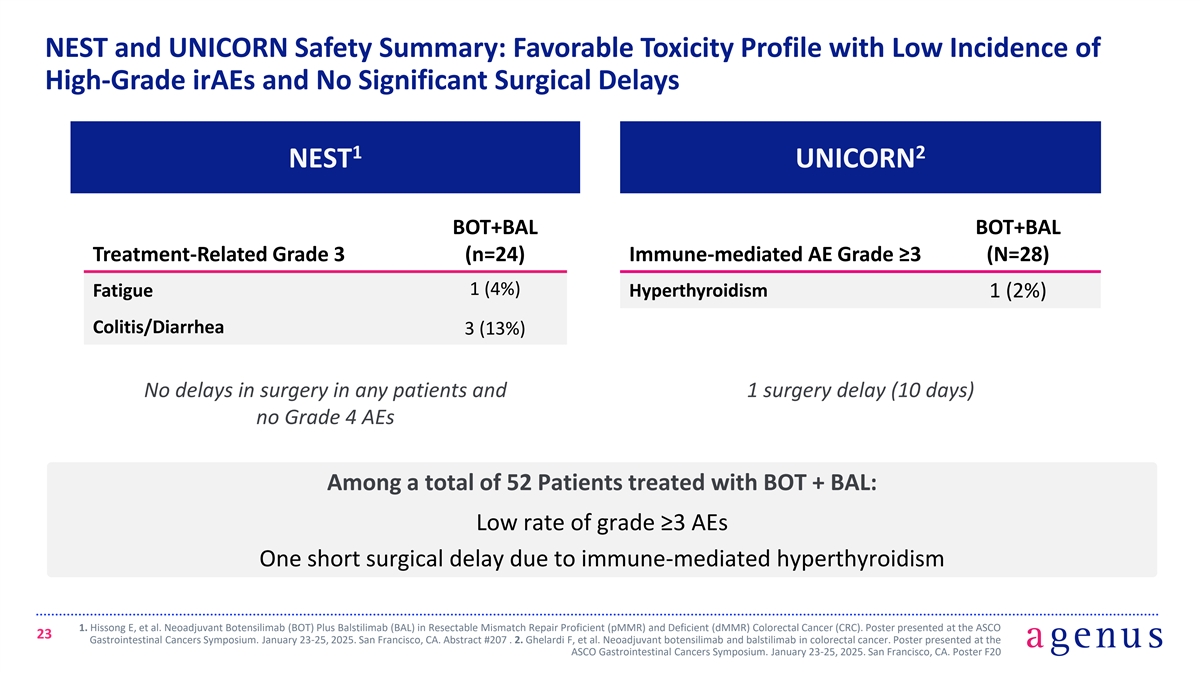
NEST and UNICORN Safety Summary: Favorable Toxicity Profile with Low Incidence of High-Grade irAEs and No Significant Surgical Delays 1 2 NEST UNICORN BOT+BAL BOT+BAL Treatment-Related Grade 3 (n=24) Immune-mediated AE Grade ≥3 (N=28) 1 (4%) Fatigue Hyperthyroidism 1 (2%) Colitis/Diarrhea 3 (13%) No delays in surgery in any patients and 1 surgery delay (10 days) no Grade 4 AEs Among a total of 52 Patients treated with BOT + BAL: Low rate of grade ≥3 AEs One short surgical delay due to immune-mediated hyperthyroidism 1. Hissong E, et al. Neoadjuvant Botensilimab (BOT) Plus Balstilimab (BAL) in Resectable Mismatch Repair Proficient (pMMR) and Deficient (dMMR) Colorectal Cancer (CRC). Poster presented at the ASCO 23 Gastrointestinal Cancers Symposium. January 23-25, 2025. San Francisco, CA. Abstract #207 . 2. Ghelardi F, et al. Neoadjuvant botensilimab and balstilimab in colorectal cancer. Poster presented at the ASCO Gastrointestinal Cancers Symposium. January 23-25, 2025. San Francisco, CA. Poster F20
ROBBIN*: Phase 3, Randomized Controlled Study of Neoadjuvant BOT+BAL in High-Risk Stage II and Stage III MSS Colon Cancer Steven O’Day, MD Chief Medical Officer, Agenus *A Phase 3 Randomized, Open-Label Study of Botensilimab Plus Balstilimab In the Neoadjuvant Setting followed by Standard of Care Versus Standard of Care Alone in Previously Untreated High-Risk Stage II and Stage III Non–MSI-H/dMMR Colon Cancer (ROBBIN Study) 24
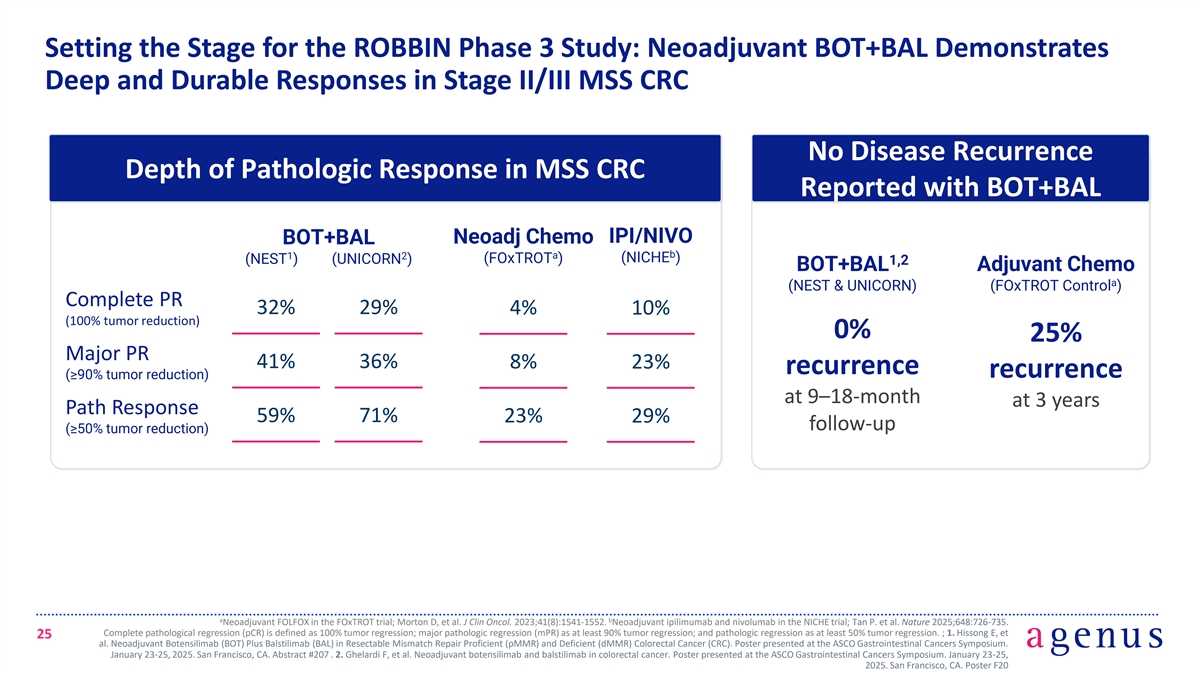
Setting the Stage for the ROBBIN Phase 3 Study: Neoadjuvant BOT+BAL Demonstrates Deep and Durable Responses in Stage II/III MSS CRC No Disease Recurrence Depth of Pathologic Response in MSS CRC Reported with BOT+BAL IPI/NIVO Neoadj Chemo BOT+BAL b a 1 2 (NICHE ) (NEST ) (UNICORN ) (FOxTROT ) 1,2 BOT+BAL Adjuvant Chemo a (NEST & UNICORN) (FOxTROT Control ) Complete PR 32% 29% 4% 10% (100% tumor reduction) 0% 25% Major PR 41% 36% 8% 23% recurrence recurrence (≥90% tumor reduction) at 9–18-month at 3 years Path Response 59% 71% 23% 29% follow-up (≥50% tumor reduction) a b Neoadjuvant FOLFOX in the FOxTROT trial; Morton D, et al. J Clin Oncol. 2023;41(8):1541-1552. Neoadjuvant ipilimumab and nivolumab in the NICHE trial; Tan P. et al. Nature 2025;648:726-735. Complete pathological regression (pCR) is defined as 100% tumor regression; major pathologic regression (mPR) as at least 90% tumor regression; and pathologic regression as at least 50% tumor regression. ; 1. Hissong E, et 25 al. Neoadjuvant Botensilimab (BOT) Plus Balstilimab (BAL) in Resectable Mismatch Repair Proficient (pMMR) and Deficient (dMMR) Colorectal Cancer (CRC). Poster presented at the ASCO Gastrointestinal Cancers Symposium. January 23-25, 2025. San Francisco, CA. Abstract #207 . 2. Ghelardi F, et al. Neoadjuvant botensilimab and balstilimab in colorectal cancer. Poster presented at the ASCO Gastrointestinal Cancers Symposium. January 23-25, 2025. San Francisco, CA. Poster F20
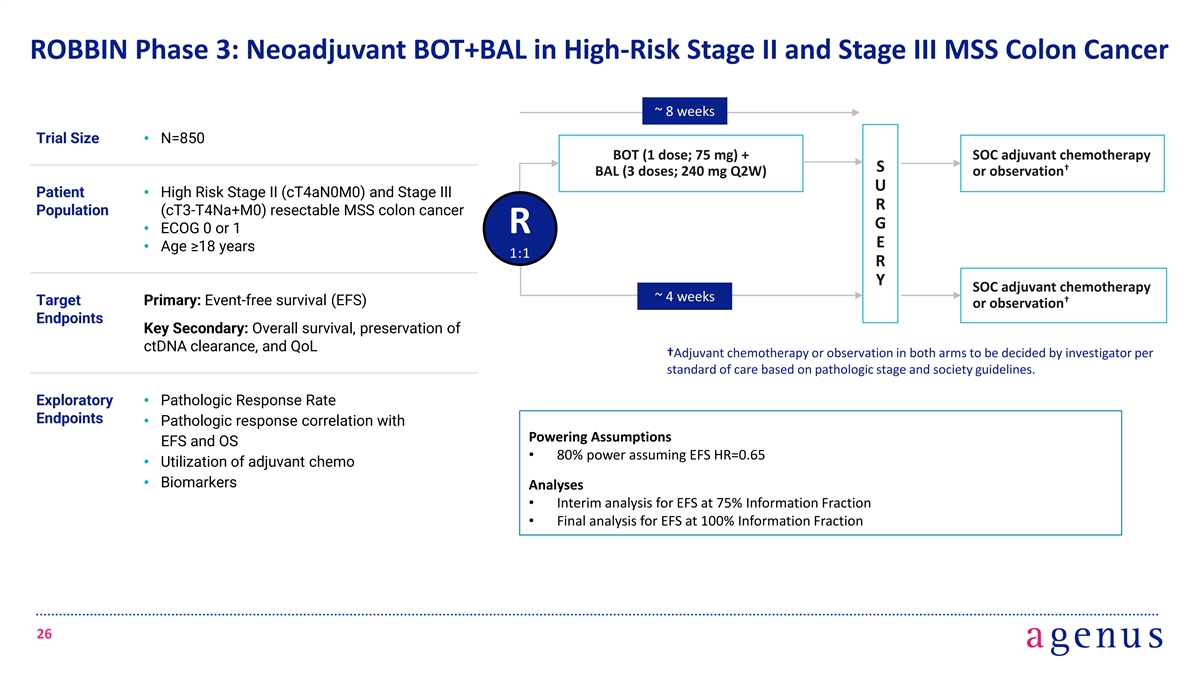
ROBBIN Phase 3: Neoadjuvant BOT+BAL in High-Risk Stage II and Stage III MSS Colon Cancer ~ 8 weeks Trial Size• N=850 BOT (1 dose; 75 mg) + SOC adjuvant chemotherapy † S BAL (3 doses; 240 mg Q2W) or observation U Patient • High Risk Stage II (cT4aN0M0) and Stage III R Population (cT3-T4Na+M0) resectable MSS colon cancer G • ECOG 0 or 1 R E • Age ≥18 years 1:1 R Y SOC adjuvant chemotherapy ~ 4 weeks † Target Primary: Event-free survival (EFS) or observation Endpoints Key Secondary: Overall survival, preservation of ctDNA clearance, and QoL †Adjuvant chemotherapy or observation in both arms to be decided by investigator per standard of care based on pathologic stage and society guidelines. Exploratory • Pathologic Response Rate Endpoints • Pathologic response correlation with Powering Assumptions EFS and OS • 80% power assuming EFS HR=0.65 • Utilization of adjuvant chemo • Biomarkers Analyses • Interim analysis for EFS at 75% Information Fraction • Final analysis for EFS at 100% Information Fraction 26
ROBBIN Phase 3 Trial Aligned with FDA Feedback The following key elements of the Phase 3 study are aligned with FDA feedback: • The proposed patient population of Stage II (cT4aN0M0) and Stage III (cT3-T4Na+M0) Colon Cancer that is not MSI-H/dMMR • The proposed experimental arm of neoadjuvant BOT and BAL followed by surgery and guideline- directed adjuvant chemotherapy based on pathologic staging • The control arm based on the current standard of care of surgery followed by guideline-directed adjuvant chemotherapy based on pathologic staging • The primary endpoint of EFS and the proposed interim analysis plan 27
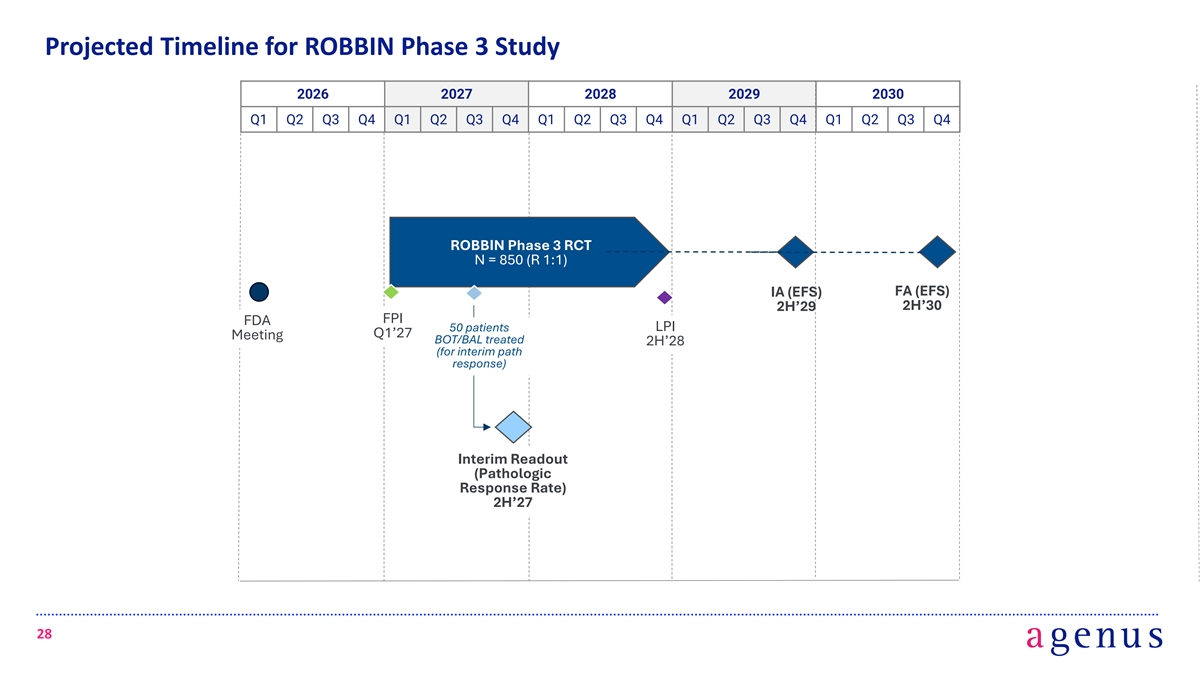
Projected Timeline for ROBBIN Phase 3 Study 2026 2027 2028 2029 2030 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 ROBBIN Phase 3 RCT N = 850 (R 1:1) IA (EFS) FA (EFS) 2H’30 2H’29 FPI FDA 50 patients LPI Q1’27 Meeting BOT/BAL treated 2H’28 (for interim path response) Interim Readout (Pathologic Response Rate) 2H’27 28
Fully Funded, FDA-aligned Phase 3 Trial Testing Neoadjuvant BOT+BAL in MSS Colon Cancer, a Multi Billion-Dollar Opportunity in the US • Financing of $85M upfront and up to $340M in total, focused on BOT+BAL opportunity in high-risk Stage II and Stage III MSS Colon Cancer, >$7 Billion TAM in the US • Capital will be directed to an FDA-aligned pivotal Phase 3 study (“ROBBIN”) of neoadjuvant BOT+BAL for MSS Colon Cancer (n=850, Randomized 1:1, Primary Endpoint EFS) • To focus company resources, Agenus is discontinuing support for the ongoing BATTMAN Phase 3 study • Key upcoming catalysts for ROBBIN Phase 3 Trial (Neoadjuvant BOT+BAL): • ROBBIN first patient dosed: anticipated Q1 of 2027 • Interim pathologic response data: anticipated second half of 2027 • Interim analysis of EFS: anticipated second half of 2029 • Final analysis of EFS: anticipated second half of 2030 1. Epidemiology analysis based on data from SEER, CDC, and Clarivate; assumes 38,000 eligible patient population annually * $200K for a course of neoadjuvant treatment. 29
Q&A 30

agenusbio.com