Exhibit 99.1 SIGNAL-AA Part B 36-Week Topline Results July 2026
Forward Looking Statements This presentation has been prepared by Q32 Bio Inc. (“we”, “us,” “our,” “Q32” or the “Company”) and is made for informational purposes only. The information set forth herein does not purport to be complete or contain all of the information you may desire. Statements contained herein are made as of the date of this presentation unless stated otherwise, and this presentation shall not under any circumstances create an implication that the information contained herein is correct as of any time after such date or that information will be updated or revised to reflect information that subsequently becomes available or changes occurring after the date hereof. This presentation contains forward-looking statements within the meaning of the U.S. Private Securities Litigation Reform Act of 1995, as amended. Forward-looking statements can be identified by words such as “may,” “will,” “should,” “would,” “expect,” “anticipate,” “plan,” “likely,” “believe,” “estimate,” “project,” “intend,” “potential,” and similar expressions regarding future periods. These forward-looking statements include, but are not limited to, our beliefs, observations, expectations and assumptions regarding the topline data from Part B of the SIGNAL-AA Phase 2a clinical trial and the safety, tolerability, clinical activity including biomarker data, potential efficacy and potential benefits of bempikibart, plans and expectations for Part B of the SIGNAL-AA Phase 2a clinical trial, the expectations surrounding the potential, safety, efficacy, and regulatory and clinical progress of Q32’s product candidates, including bempikibart, and anticipated milestones, timing of anticipated registrational trials, data readouts and timing, and the US Alopecia Areata market size and potential commercial opportunities, among others. Statements that are not historical facts are forward-looking statements. Forward-looking statements are based on current beliefs and assumptions that are subject to risks and uncertainties and are not guarantees of future performance. Actual results could differ materially from those contained in any forward-looking statement as a result of various factors, including, without limitation: the Company’s need for additional funding, which may not be available; failure to identify additional product candidates and develop or commercialize marketable products; the early stage of the Company’s development efforts; potential unforeseen events during clinical trials could cause delays or other adverse consequences; risks relating to the regulatory approval process; interim, topline and preliminary data may change as more patient data become available, and are subject to audit and verifica tion procedures that could result in material changes in the final data; Q32’s product candidates may cause serious adverse side effects; inability to maintain our collaborations, or the failure of these collaborations; our reliance on third parties, including for the manufacture of materials for our research programs, preclinical and clinical studies; failure to obtain U.S . or international marketing approval; ongoing regulatory obligations; effects of significant competition; unfavorable pricing regulations, third-party reimbursement practices or healthcare reform initiatives; product liability lawsuits; securities class action litigation; the impact of global pandemics or public health emergencies and general economic conditions on our business and operations, including our preclinical studies and clinical trials; the possibility of system failures or security breaches; risks relating to intellectual property and our ability to protect our patents and other proprietary rights; significant costs incurred as a result of operating as a public company; as well as those risk and uncertainties set forth more fully under the caption “Risk Factors” in our Annual Report on Form 10-K for the year ended December 31, 2025 as well as other risks detailed in our subsequent filings with the United States Securities and Exchange Commission. Any forward-looking statement made by us is based only on information currently available to us and speaks only as of the date on which it is made. We undertake no obligation to publicly update any forward-looking statement, whether written or oral, that may be made from time to time, whether as a result of new information or future developments nor otherwise, unless required by law. Certain information contained in this presentation relates to or is based on studies, publications, analyses, surveys and other data obtained from third-party sources and the Company’s own internal estimates and research. While the Company believes these third-party sources to be reliable as of the date of this presentation, it has not independently verified, and makes no representation as to the adequacy, fairness, accuracy or completeness of, any information obtained from third-party sources. In addition, all of the market data included in this presentation involves a number of assumptions and limitations, and there can be no guarantee as to the accuracy or reliability of such assumptions. Finally, while we believe our own internal research is reliable, such research may not have been verified by any independent source. 2
Q32 Bio Management Joined by Renowned Alopecia Areata Key Opinion Leader TODAY’S AGENDA Q32 Bio Leadership Introduction Bempikibart Overview Jodie Morrison Shelia Violette, Ph.D. Lee Kalowski, M.B.A. SIGNAL-AA Part B Results Chief Executive Officer Founder & President & Chief Scientific Officer Chief Financial Officer and Next Steps Key Opinion Leader Alopecia Areata Unmet Need, Landscape and Commercial Opportunity Arash Mostaghimi, MD, MPA, MPH Associate Professor of Dermatology and Vice Chair of Clinical Trials and Innovation, Brigham and Women’s Hospital, Harvard Medical School Q&A 3
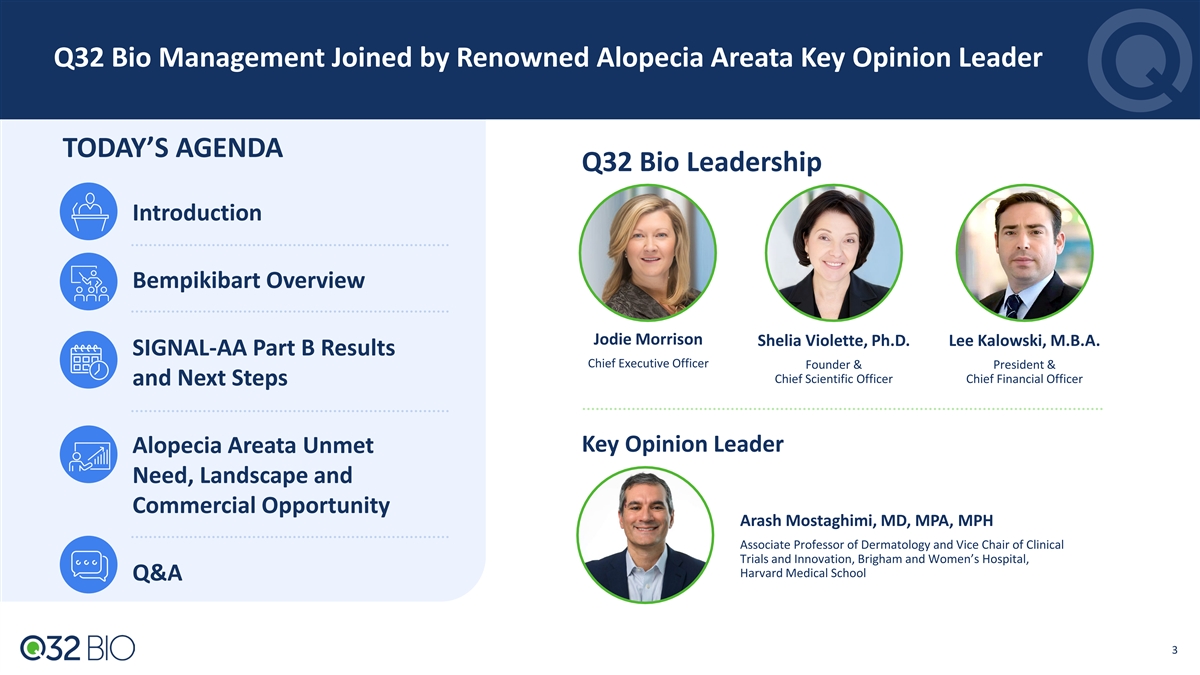
Bempikibart SIGNAL-AA: Part B Builds on Prior Proof Of Concept in Alopecia Areata Demonstrating Robust Clinical Activity at 36 Weeks Bempikibart continued to demonstrate a Robust clinical activity favorable safety profile; negligible ADA No Grade 3 or higher AEs and no new Week 36 Results safety signals Results demonstrate potential for 1 Mean SALT change (mITT analysis ) differentiated profile for the treatment 35.3% of alopecia areata Profile supports further expansion in alopecia areata (registration-directed program for SALT-20 response (mITT analysis) 40.0% severe/very severe, plans for development in adolescent, moderate alopecia areata) SALT-20 response (ITT analysis) Off-drug follow-up through Week 52 and 30.3% Part B OLE remain ongoing Note: Data cutoff as of June 30, 2026; All calculations are based on prespecified criteria defined in Part B statistical analysis plan (SAP); SALT = Severity of Alopecia Tool; mITT = Modified intent to treat population; ITT = intent to treat population; ADA = Anti-Drug Antibody; OLE = Open-Label Extension 4 4 1 Prespecified sensitivity on mean percent change from baseline in SALT score using MMRM: LS mean change is 39.1%
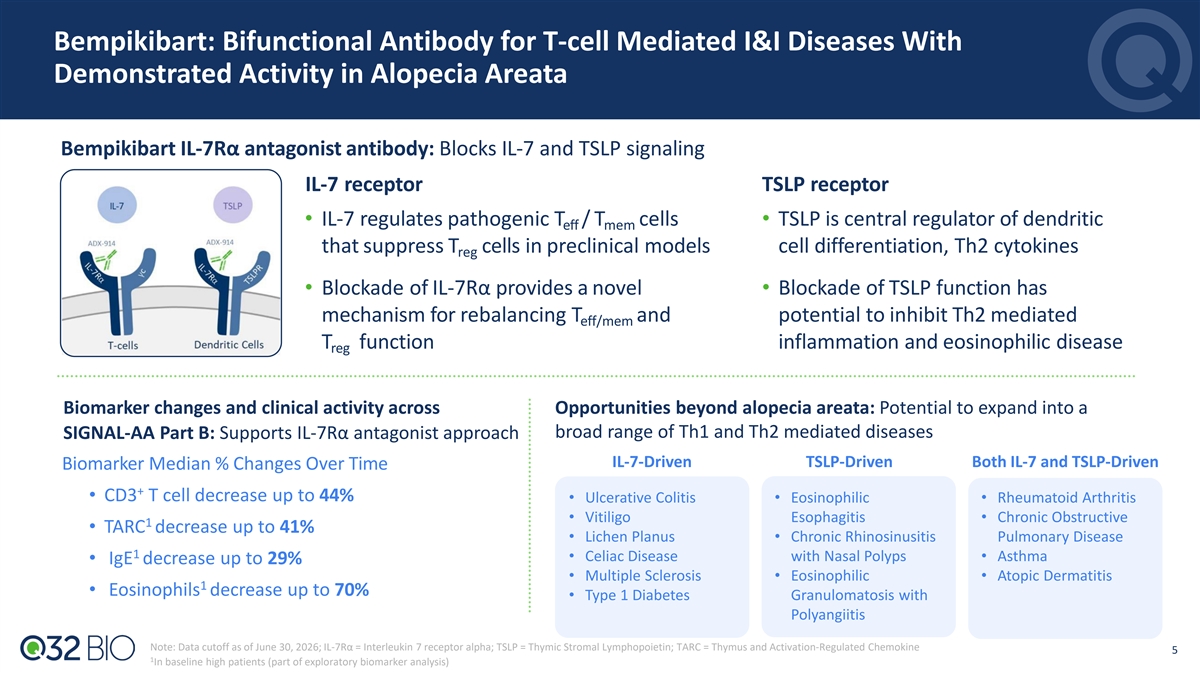
Bempikibart: Bifunctional Antibody for T-cell Mediated I&I Diseases With Demonstrated Activity in Alopecia Areata Bempikibart IL-7Rα antagonist antibody: Blocks IL-7 and TSLP signaling IL-7 receptor TSLP receptor • IL-7 regulates pathogenic T / T cells • TSLP is central regulator of dendritic eff mem that suppress T cells in preclinical models cell differentiation, Th2 cytokines reg • Blockade of IL-7Rα provides a novel • Blockade of TSLP function has mechanism for rebalancing T and potential to inhibit Th2 mediated eff/mem T function inflammation and eosinophilic disease reg Biomarker changes and clinical activity across Opportunities beyond alopecia areata: Potential to expand into a broad range of Th1 and Th2 mediated diseases SIGNAL-AA Part B: Supports IL-7Rα antagonist approach IL-7-Driven TSLP-Driven Both IL-7 and TSLP-Driven Biomarker Median % Changes Over Time + • CD3 T cell decrease up to 44% • Ulcerative Colitis • Eosinophilic • Rheumatoid Arthritis • Vitiligo Esophagitis • Chronic Obstructive 1 • TARC decrease up to 41% • Lichen Planus • Chronic Rhinosinusitis Pulmonary Disease 1 • Celiac Disease with Nasal Polyps • Asthma • IgE decrease up to 29% • Multiple Sclerosis • Eosinophilic • Atopic Dermatitis 1 • Eosinophils decrease up to 70% • Type 1 Diabetes Granulomatosis with Polyangiitis Note: Data cutoff as of June 30, 2026; IL-7Rα = Interleukin 7 receptor alpha; TSLP = Thymic Stromal Lymphopoietin; TARC = Thymus and Activation-Regulated Chemokine 5 1 In baseline high patients (part of exploratory biomarker analysis)
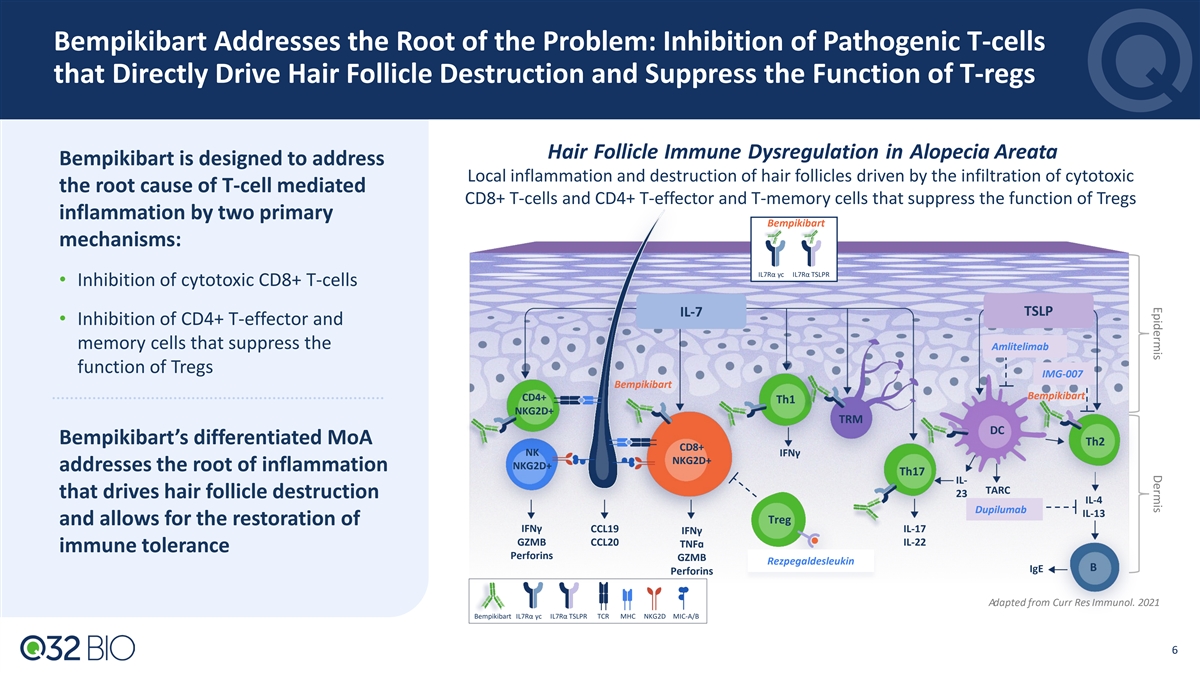
Epidermis Dermis Bempikibart Addresses the Root of the Problem: Inhibition of Pathogenic T-cells that Directly Drive Hair Follicle Destruction and Suppress the Function of T-regs Hair Follicle Immune Dysregulation in Alopecia Areata Bempikibart is designed to address Local inflammation and destruction of hair follicles driven by the infiltration of cytotoxic the root cause of T-cell mediated CD8+ T-cells and CD4+ T-effector and T-memory cells that suppress the function of Tregs inflammation by two primary Bempikibart mechanisms: IL7Rα γc IL7Rα TSLPR • Inhibition of cytotoxic CD8+ T-cells IL-7 TSLP • Inhibition of CD4+ T-effector and memory cells that suppress the Amlitelimab function of Tregs IMG-007 Bempikibart Bempikibart CD4+ Th1 NKG2D+ TRM DC Bempikibart’s differentiated MoA Th2 CD8+ NKIFNγ NKG2D+ NKG2D+ addresses the root of inflammation Th17 IL- TARC 23 that drives hair follicle destruction IL-4 Dupilumab IL-13 Treg and allows for the restoration of IFNγ CCL19 IL-17 IFNγ GZMB CCL20 IL-22 TNFɑ immune tolerance Perforins GZMB Rezpegaldesleukin B IgE Perforins Adapted from Curr Res Immunol. 2021 Bempikibart IL7Rα γc IL7Rα TSLPR TCR MHC NKG2D MIC-A/B 6
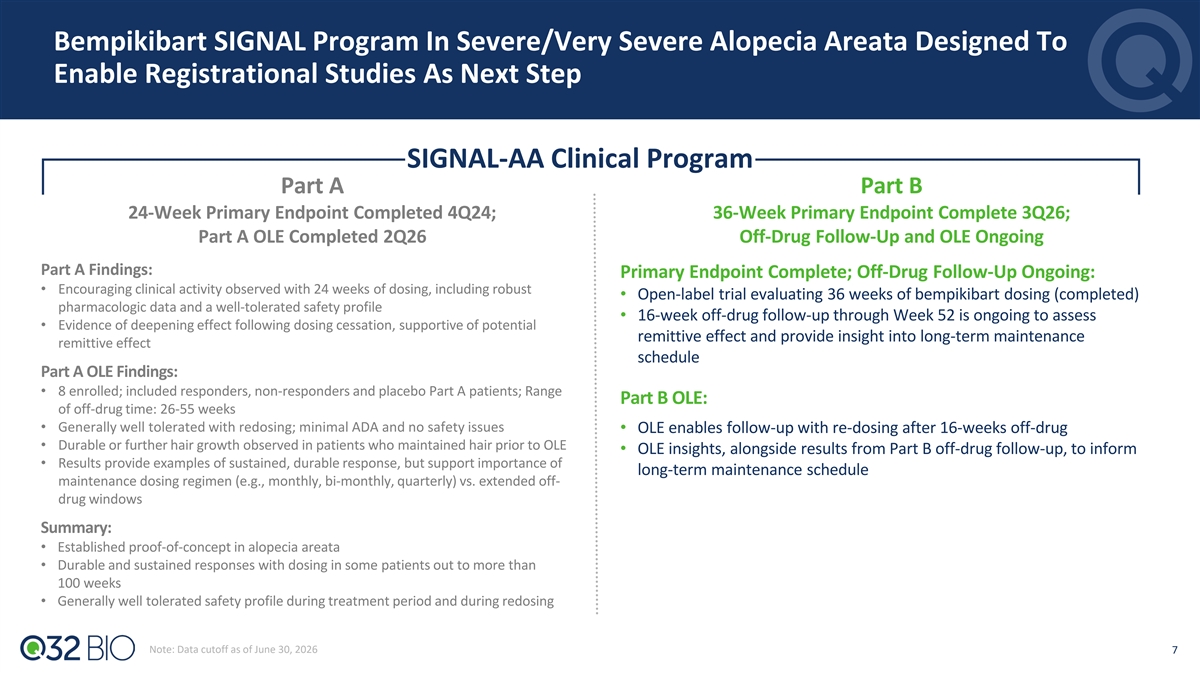
Bempikibart SIGNAL Program In Severe/Very Severe Alopecia Areata Designed To Enable Registrational Studies As Next Step Part A SIGNAL-AA Clinical Program Part A Part B 24-Week Primary Endpoint Completed 4Q24; 36-Week Primary Endpoint Complete 3Q26; Part A OLE Completed 2Q26 Off-Drug Follow-Up and OLE Ongoing Part A Findings: Primary Endpoint Complete; Off-Drug Follow-Up Ongoing: • Encouraging clinical activity observed with 24 weeks of dosing, including robust • Open-label trial evaluating 36 weeks of bempikibart dosing (completed) pharmacologic data and a well-tolerated safety profile • 16-week off-drug follow-up through Week 52 is ongoing to assess • Evidence of deepening effect following dosing cessation, supportive of potential Part A remittive effect and provide insight into long-term maintenance remittive effect schedule Part A OLE Findings: • 8 enrolled; included responders, non-responders and placebo Part A patients; Range Part B OLE: of off-drug time: 26-55 weeks • Generally well tolerated with redosing; minimal ADA and no safety issues • OLE enables follow-up with re-dosing after 16-weeks off-drug • Durable or further hair growth observed in patients who maintained hair prior to OLE • OLE insights, alongside results from Part B off-drug follow-up, to inform • Results provide examples of sustained, durable response, but support importance of long-term maintenance schedule maintenance dosing regimen (e.g., monthly, bi-monthly, quarterly) vs. extended off- drug windows Summary: • Established proof-of-concept in alopecia areata • Durable and sustained responses with dosing in some patients out to more than 100 weeks • Generally well tolerated safety profile during treatment period and during redosing Note: Data cutoff as of June 30, 2026 7
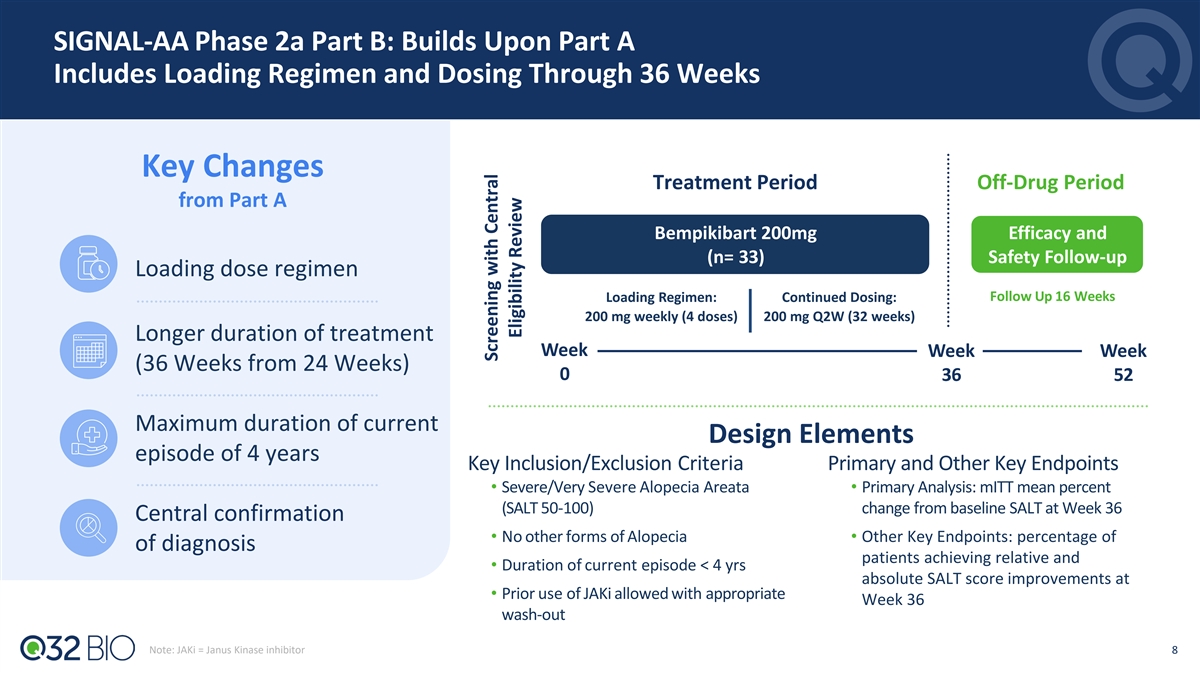
SIGNAL-AA Phase 2a Part B: Builds Upon Part A Includes Loading Regimen and Dosing Through 36 Weeks Key Changes Treatment Period Off-Drug Period from Part A Bempikibart 200mg Efficacy and (n= 33) Safety Follow-up Loading dose regimen 1 Placebo (n=8 ) Follow Up 16 Weeks Loading Regimen: Continued Dosing: 200 mg weekly (4 doses) 200 mg Q2W (32 weeks) Q2W Longer duration of treatment Week Week Week (36 Weeks from 24 Weeks) 0 36 52 Maximum duration of current Design Elements episode of 4 years Key Inclusion/Exclusion Criteria Primary and Other Key Endpoints • Severe/Very Severe Alopecia Areata • Primary Analysis: mITT mean percent (SALT 50-100) change from baseline SALT at Week 36 Central confirmation • No other forms of Alopecia • Other Key Endpoints: percentage of of diagnosis patients achieving relative and • Duration of current episode < 4 yrs absolute SALT score improvements at • Prior use of JAKi allowed with appropriate Week 36 wash-out Note: JAKi = Janus Kinase inhibitor 8 Screening with Central Eligibility Review
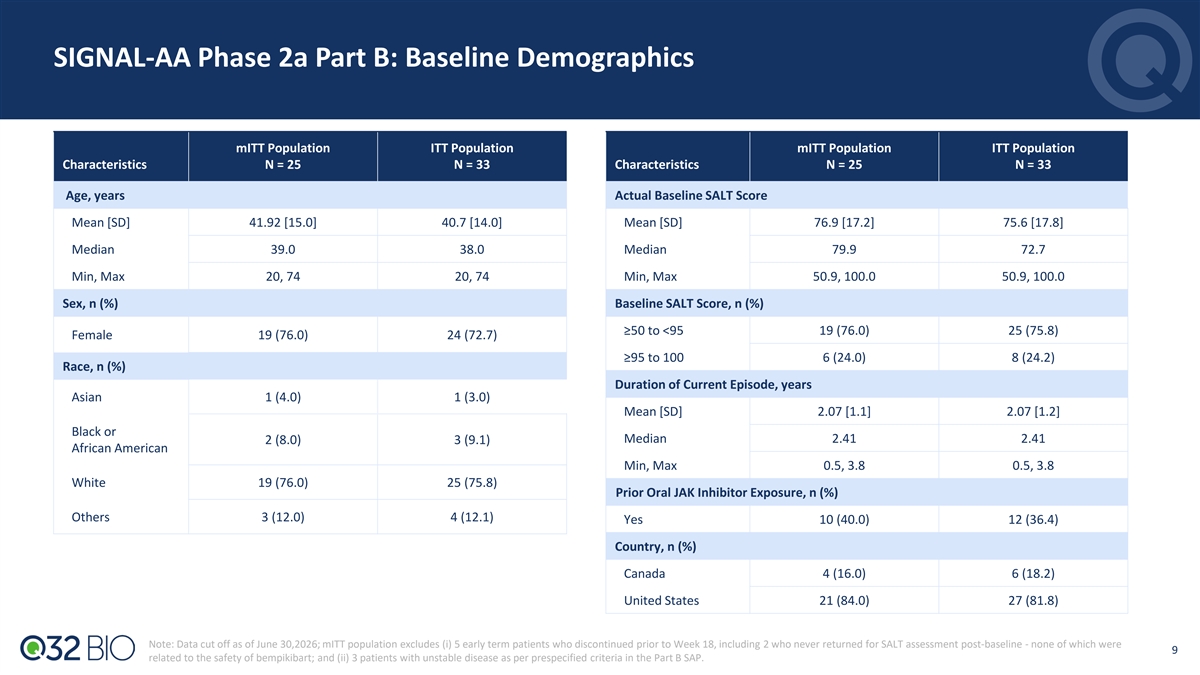
SIGNAL-AA Phase 2a Part B: Baseline Demographics mITT Population ITT Population mITT Population ITT Population Characteristics N = 25 N = 33 Characteristics N = 25 N = 33 Age, years Actual Baseline SALT Score Mean [SD] 41.92 [15.0] 40.7 [14.0] Mean [SD] 76.9 [17.2] 75.6 [17.8] Median 39.0 38.0 Median 79.9 72.7 Min, Max 20, 74 20, 74 Min, Max 50.9, 100.0 50.9, 100.0 Sex, n (%) Baseline SALT Score, n (%) ≥50 to <95 19 (76.0) 25 (75.8) Female 19 (76.0) 24 (72.7) ≥95 to 100 6 (24.0) 8 (24.2) Race, n (%) Duration of Current Episode, years Asian 1 (4.0) 1 (3.0) Mean [SD] 2.07 [1.1] 2.07 [1.2] Black or Median 2.41 2.41 2 (8.0) 3 (9.1) African American Min, Max 0.5, 3.8 0.5, 3.8 White 19 (76.0) 25 (75.8) Prior Oral JAK Inhibitor Exposure, n (%) Others 3 (12.0) 4 (12.1) Yes 10 (40.0) 12 (36.4) Country, n (%) Canada 4 (16.0) 6 (18.2) United States 21 (84.0) 27 (81.8) Note: Data cut off as of June 30,2026; mITT population excludes (i) 5 early term patients who discontinued prior to Week 18, including 2 who never returned for SALT assessment post-baseline - none of which were 9 related to the safety of bempikibart; and (ii) 3 patients with unstable disease as per prespecified criteria in the Part B SAP.
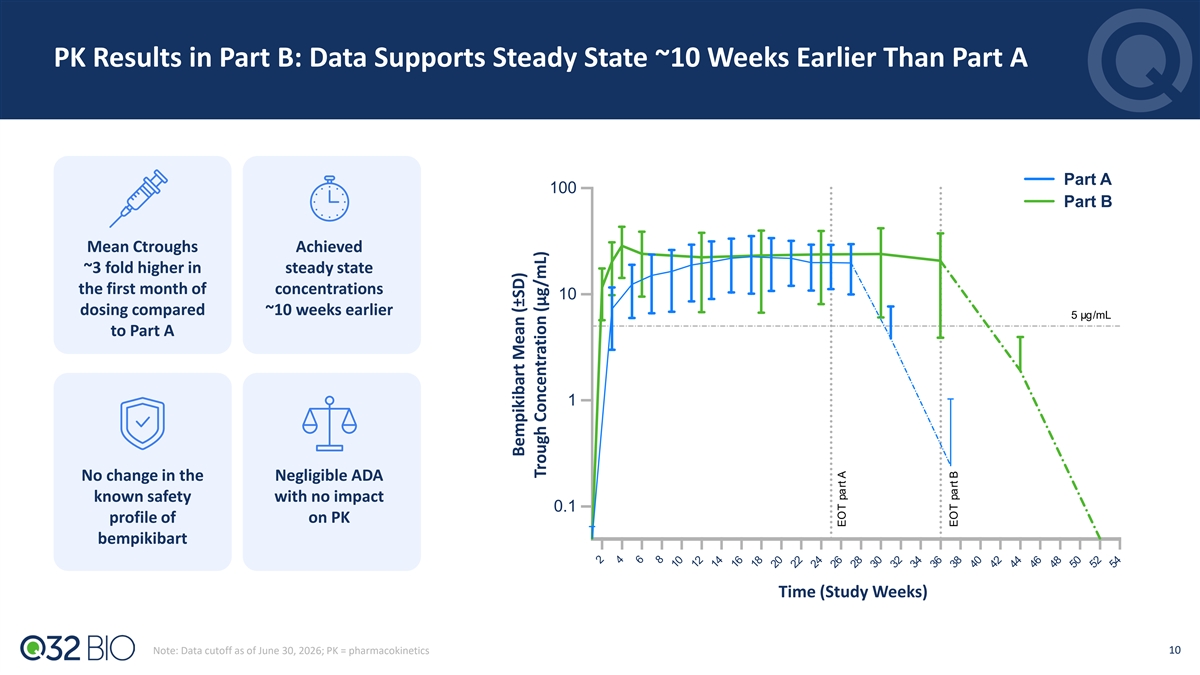
PK Results in Part B: Data Supports Steady State ~10 Weeks Earlier Than Part A Part A 100 Part B Mean Ctroughs Achieved ~3 fold higher in steady state the first month of concentrations 10 dosing compared ~10 weeks earlier 5 µg/mL to Part A 1 No change in the Negligible ADA known safety with no impact 0.1 profile of on PK bempikibart Time (Study Weeks) 10 Note: Data cutoff as of June 30, 2026; PK = pharmacokinetics Bempikibart Mean (±SD) Trough Concentrati on (µg/mL) EOT part A EOT part B
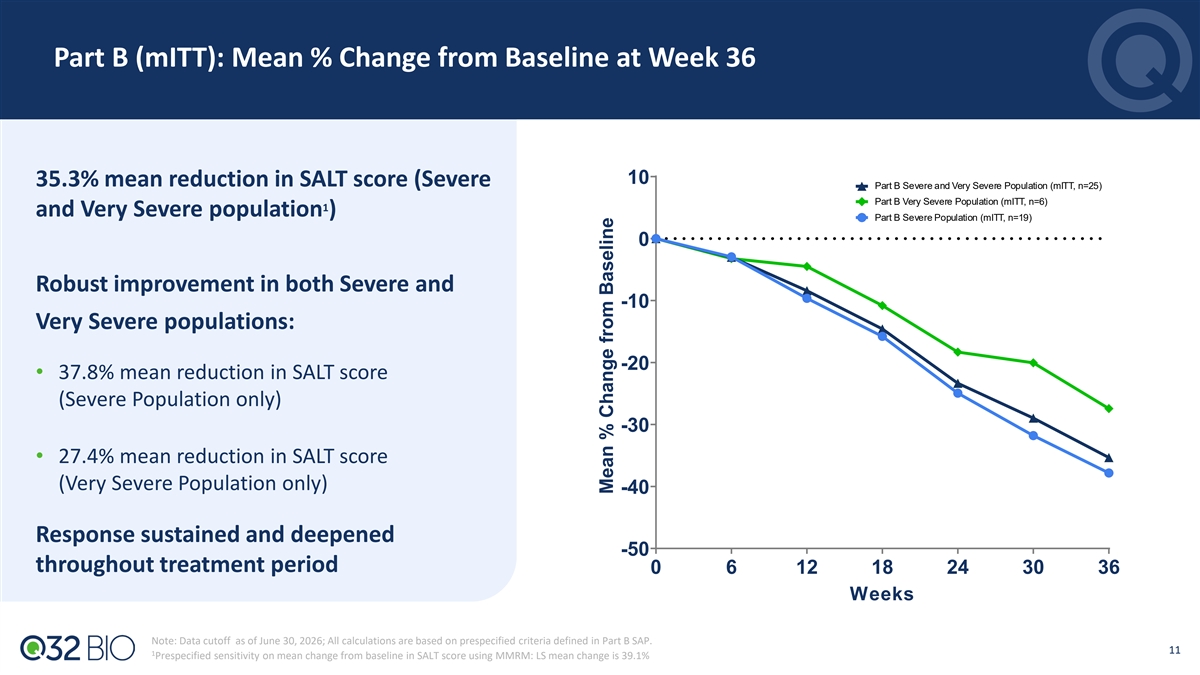
Part B (mITT): Mean % Change from Baseline at Week 36 10 35.3% mean reduction in SALT score (Severe Part B Severe and Very Severe Population (mITT, n=25) Part B Very Severe Population (mITT, n=6) 1 and Very Severe population ) Part B Severe Population (mITT, n=19) 0 Robust improvement in both Severe and -10 Very Severe populations: -20 • 37.8% mean reduction in SALT score (Severe Population only) -30 • 27.4% mean reduction in SALT score (Very Severe Population only) -40 Response sustained and deepened -50 throughout treatment period 0 6 12 18 24 30 36 Weeks Note: Data cutoff as of June 30, 2026; All calculations are based on prespecified criteria defined in Part B SAP. 11 1 Prespecified sensitivity on mean change from baseline in SALT score using MMRM: LS mean change is 39.1% Mean % Change from Baseline
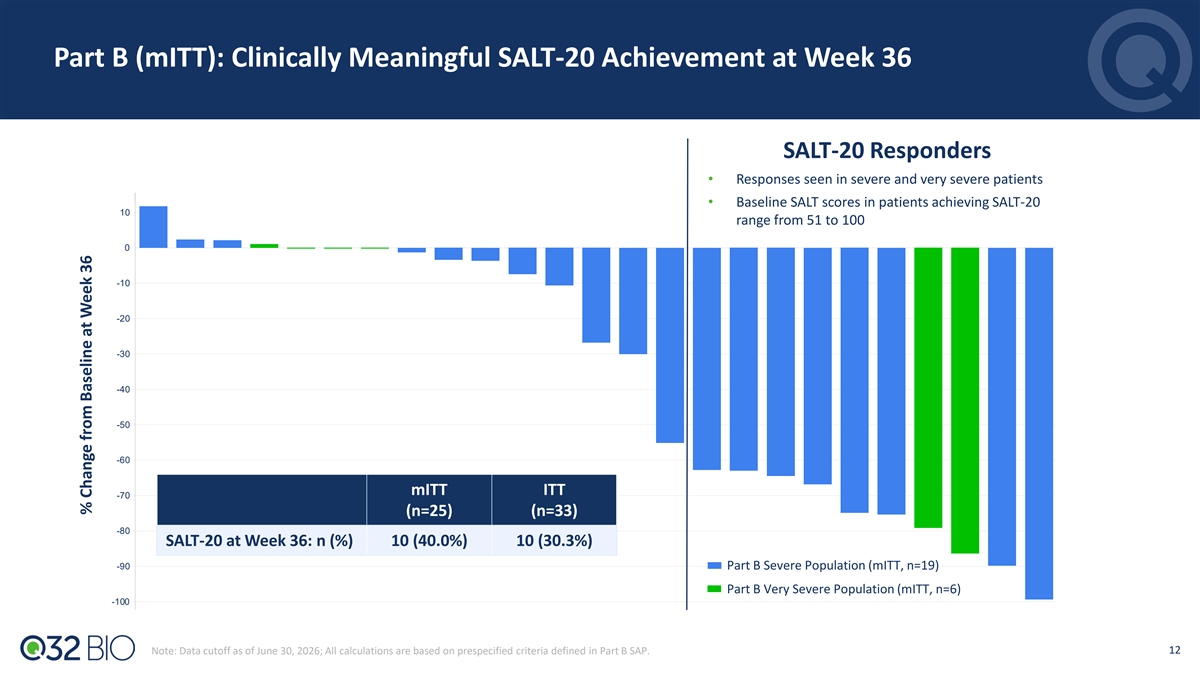
Part B (mITT): Clinically Meaningful SALT-20 Achievement at Week 36 SALT-20 Responders • Responses seen in severe and very severe patients • Baseline SALT scores in patients achieving SALT-20 10 range from 51 to 100 0 -10 -20 -30 -40 -50 -60 mITT ITT -70 (n=25) (n=33) -80 SALT-20 at Week 36: n (%) 10 (40.0%) 10 (30.3%) -90 Part B Severe Population (mITT, n=19) Part B Very Severe Population (mITT, n=6) -100 12 Note: Data cutoff as of June 30, 2026; All calculations are based on prespecified criteria defined in Part B SAP. % Change from Baseline at Week 36
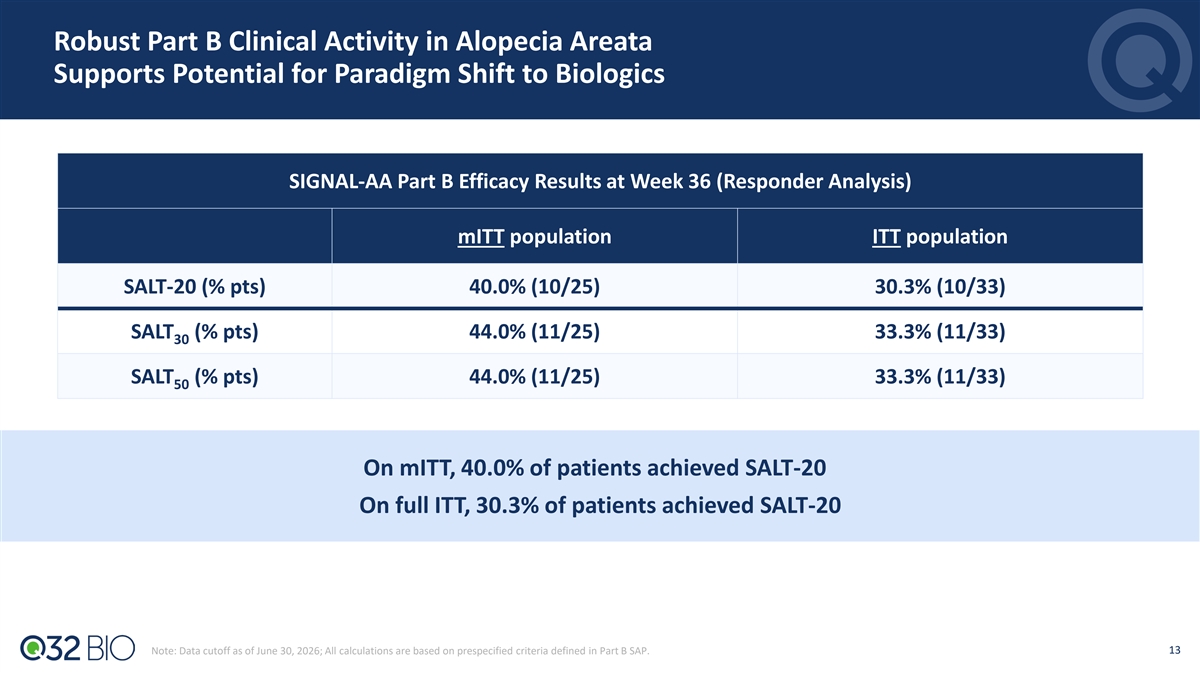
Robust Part B Clinical Activity in Alopecia Areata Supports Potential for Paradigm Shift to Biologics SIGNAL-AA Part B Efficacy Results at Week 36 (Responder Analysis) mITT population ITT population SALT-20 (% pts) 40.0% (10/25) 30.3% (10/33) SALT (% pts) 44.0% (11/25) 33.3% (11/33) 30 SALT (% pts) 44.0% (11/25) 33.3% (11/33) 50 On mITT, 40.0% of patients achieved SALT-20 On full ITT, 30.3% of patients achieved SALT-20 13 Note: Data cutoff as of June 30, 2026; All calculations are based on prespecified criteria defined in Part B SAP.
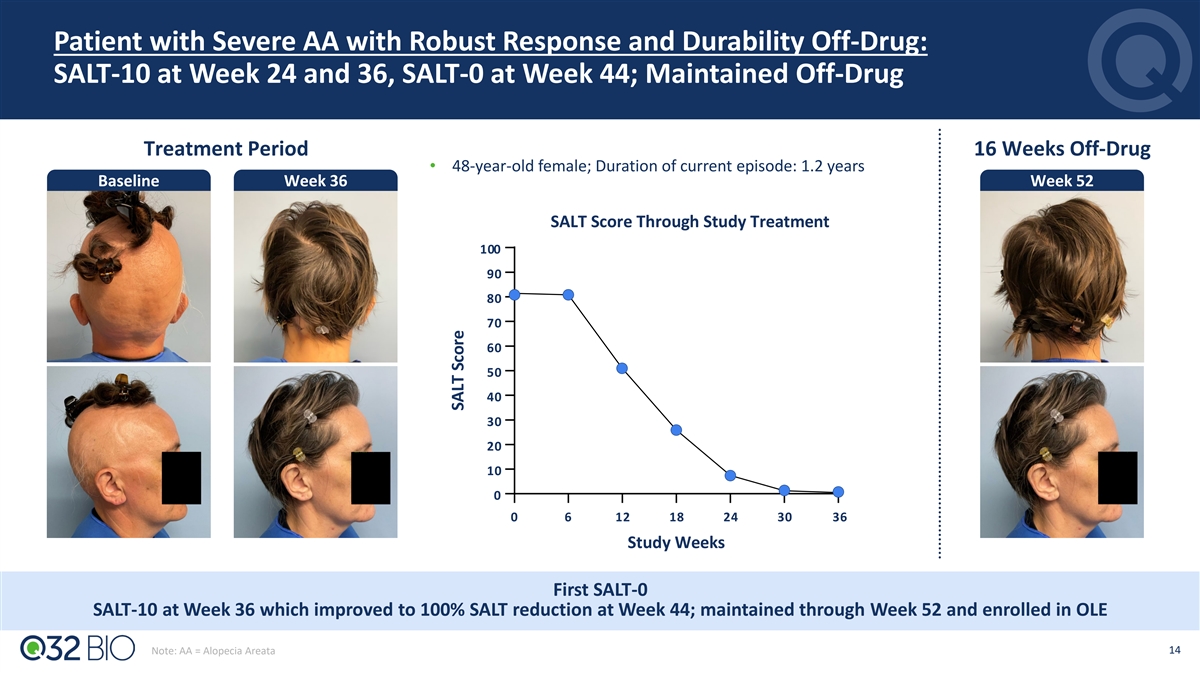
Patient with Severe AA with Robust Response and Durability Off-Drug: SALT-10 at Week 24 and 36, SALT-0 at Week 44; Maintained Off-Drug Treatment Period 16 Weeks Off-Drug • 48-year-old female; Duration of current episode: 1.2 years Baseline Week 36 Week 52 SALT Score Through Study Treatment 100 90 80 70 60 50 40 30 20 10 0 0 6 12 18 24 30 36 Study Weeks First SALT-0 SALT-10 at Week 36 which improved to 100% SALT reduction at Week 44; maintained through Week 52 and enrolled in OLE 14 Note: AA = Alopecia Areata SALT Score
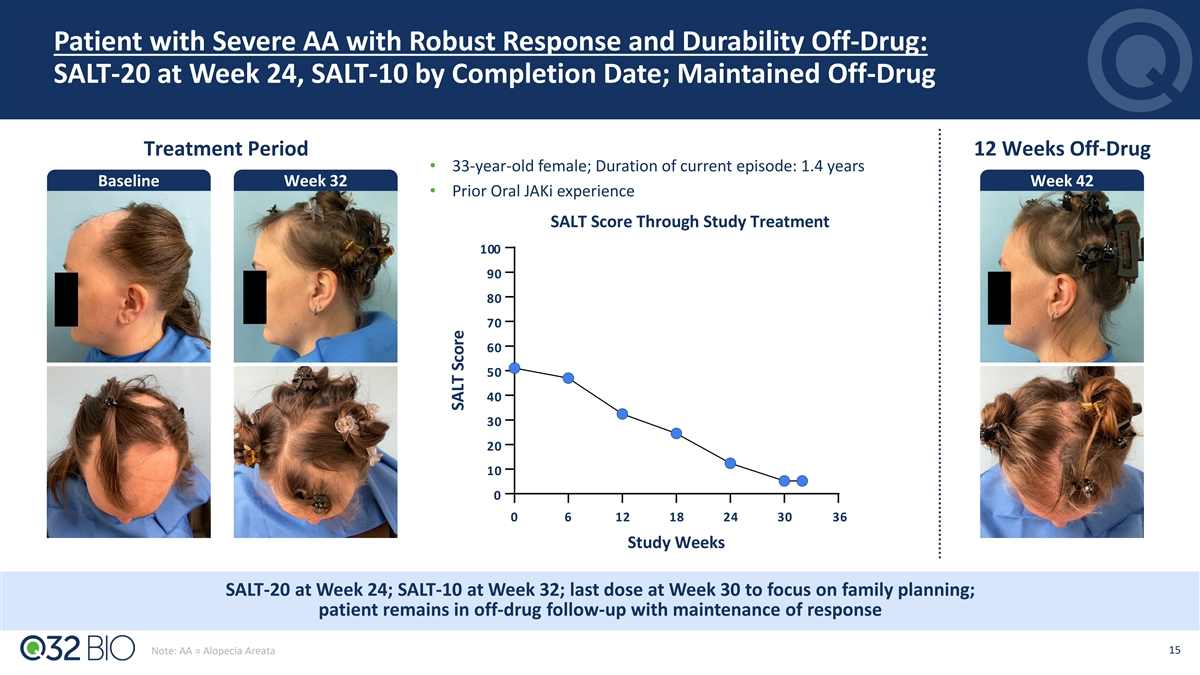
Patient with Severe AA with Robust Response and Durability Off-Drug: SALT-20 at Week 24, SALT-10 by Completion Date; Maintained Off-Drug Treatment Period 12 Weeks Off-Drug • 33-year-old female; Duration of current episode: 1.4 years Baseline Week 32 Week 42 • Prior Oral JAKi experience SALT Score Through Study Treatment 100 90 80 70 60 50 40 30 20 10 0 0 6 12 18 24 30 36 Study Weeks SALT-20 at Week 24; SALT-10 at Week 32; last dose at Week 30 to focus on family planning; patient remains in off-drug follow-up with maintenance of response 15 Note: AA = Alopecia Areata SALT Score
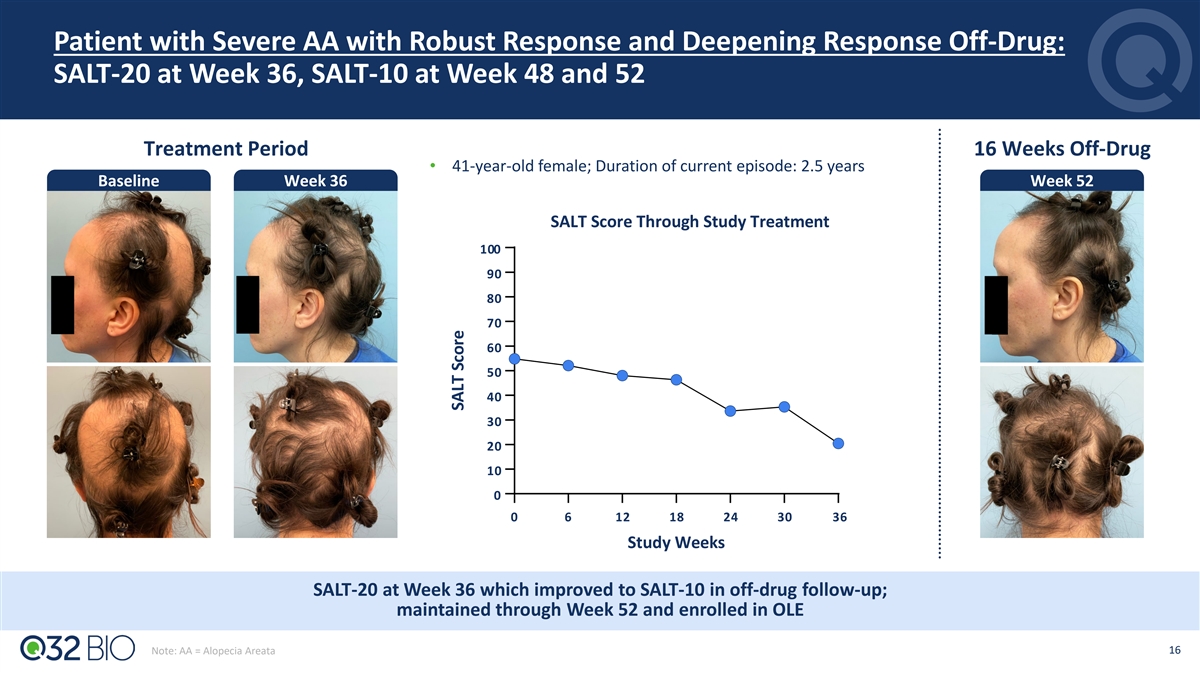
Patient with Severe AA with Robust Response and Deepening Response Off-Drug: SALT-20 at Week 36, SALT-10 at Week 48 and 52 Treatment Period 16 Weeks Off-Drug • 41-year-old female; Duration of current episode: 2.5 years Baseline Week 36 Week 52 SALT Score Through Study Treatment 100 90 80 70 60 50 40 30 20 10 0 0 6 12 18 24 30 36 Study Weeks SALT-20 at Week 36 which improved to SALT-10 in off-drug follow-up; maintained through Week 52 and enrolled in OLE 16 Note: AA = Alopecia Areata SALT Score
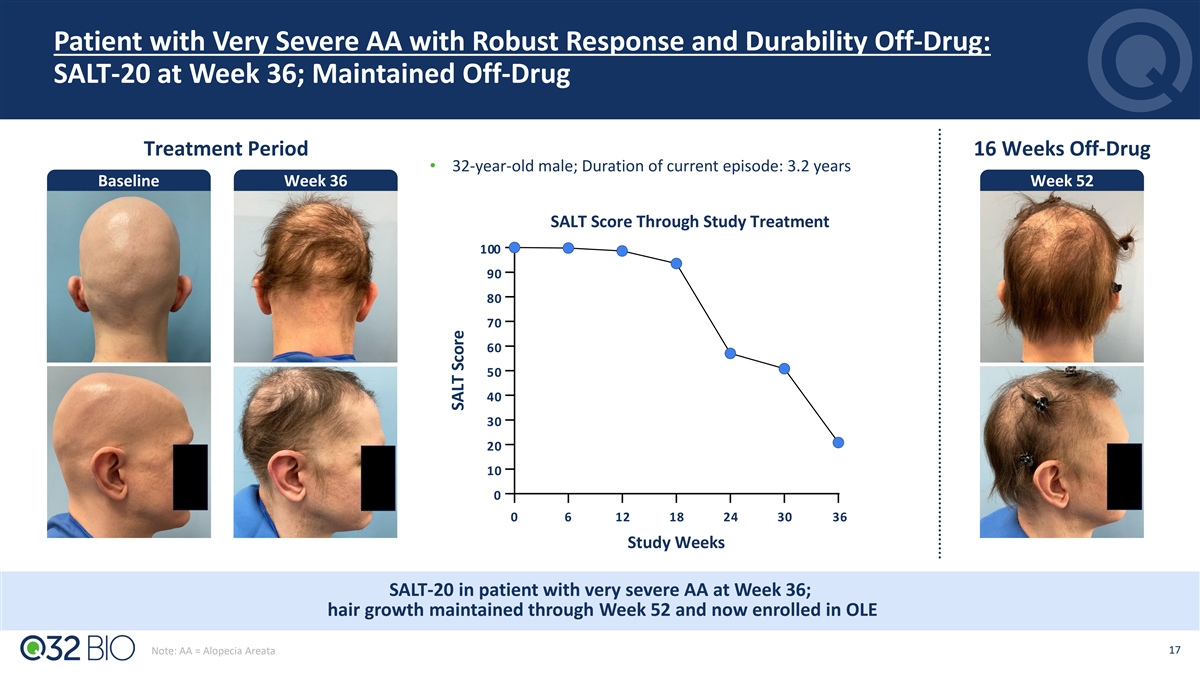
Patient with Very Severe AA with Robust Response and Durability Off-Drug: SALT-20 at Week 36; Maintained Off-Drug Treatment Period 16 Weeks Off-Drug • 32-year-old male; Duration of current episode: 3.2 years Baseline Week 36 Week 52 SALT Score Through Study Treatment 100 90 80 70 60 50 40 30 20 10 0 0 6 12 18 24 30 36 Study Weeks SALT-20 in patient with very severe AA at Week 36; hair growth maintained through Week 52 and now enrolled in OLE 17 Note: AA = Alopecia Areata SALT Score
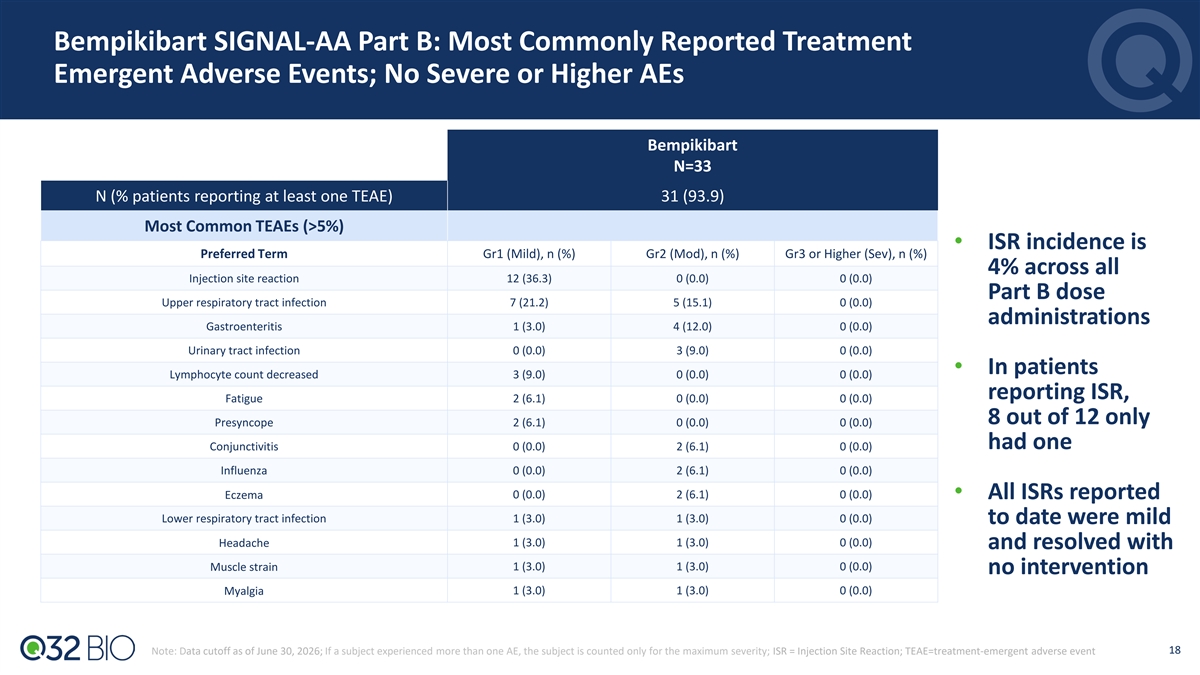
Bempikibart SIGNAL-AA Part B: Most Commonly Reported Treatment Emergent Adverse Events; No Severe or Higher AEs Bempikibart N=33 N (% patients reporting at least one TEAE) 31 (93.9) Most Common TEAEs (>5%) • ISR incidence is Preferred Term Gr1 (Mild), n (%) Gr2 (Mod), n (%) Gr3 or Higher (Sev), n (%) 4% across all Injection site reaction 12 (36.3) 0 (0.0) 0 (0.0) Part B dose Upper respiratory tract infection 7 (21.2) 5 (15.1) 0 (0.0) administrations Gastroenteritis 1 (3.0) 4 (12.0) 0 (0.0) Urinary tract infection 0 (0.0) 3 (9.0) 0 (0.0) • In patients Lymphocyte count decreased 3 (9.0) 0 (0.0) 0 (0.0) reporting ISR, Fatigue 2 (6.1) 0 (0.0) 0 (0.0) 8 out of 12 only Presyncope 2 (6.1) 0 (0.0) 0 (0.0) had one Conjunctivitis 0 (0.0) 2 (6.1) 0 (0.0) Influenza 0 (0.0) 2 (6.1) 0 (0.0) Eczema 0 (0.0) 2 (6.1) 0 (0.0) • All ISRs reported Lower respiratory tract infection 1 (3.0) 1 (3.0) 0 (0.0) to date were mild 1 (3.0) 1 (3.0) 0 (0.0) Headache and resolved with 1 (3.0) 1 (3.0) 0 (0.0) Muscle strain no intervention Myalgia 1 (3.0) 1 (3.0) 0 (0.0) 18 Note: Data cutoff as of June 30, 2026; If a subject experienced more than one AE, the subject is counted only for the maximum severity; ISR = Injection Site Reaction; TEAE=treatment-emergent adverse event
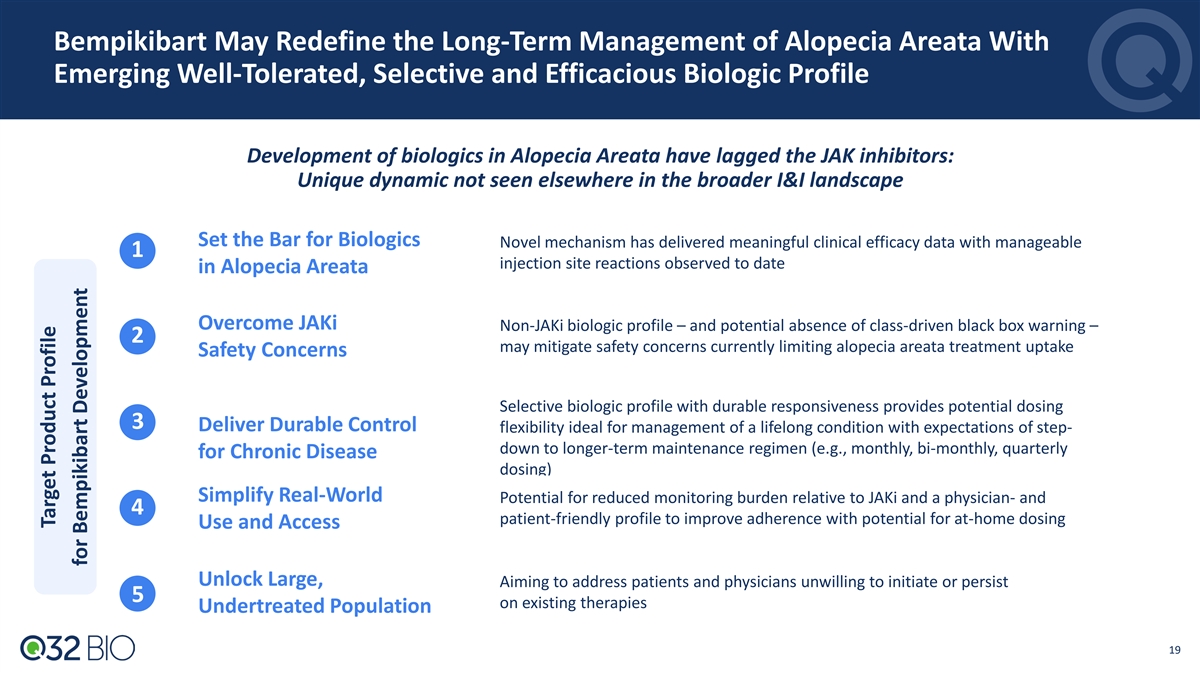
Bempikibart May Redefine the Long-Term Management of Alopecia Areata With Emerging Well-Tolerated, Selective and Efficacious Biologic Profile Development of biologics in Alopecia Areata have lagged the JAK inhibitors: Unique dynamic not seen elsewhere in the broader I&I landscape Set the Bar for Biologics Novel mechanism has delivered meaningful clinical efficacy data with manageable 1 injection site reactions observed to date in Alopecia Areata Overcome JAKi Non-JAKi biologic profile – and potential absence of class-driven black box warning – 2 may mitigate safety concerns currently limiting alopecia areata treatment uptake Safety Concerns Selective biologic profile with durable responsiveness provides potential dosing 3 Deliver Durable Control flexibility ideal for management of a lifelong condition with expectations of step- down to longer-term maintenance regimen (e.g., monthly, bi-monthly, quarterly for Chronic Disease dosing) Simplify Real-World Potential for reduced monitoring burden relative to JAKi and a physician- and 4 patient-friendly profile to improve adherence with potential for at-home dosing Use and Access Unlock Large, Aiming to address patients and physicians unwilling to initiate or persist 5 on existing therapies Undertreated Population 19 Target Product Profile for Bempikibart Development
Alopecia Areata Has Life-Altering Impact and Significant Unmet Need With Limited Treatment Options, Including JAK Inhibitors Carrying Black Box Warnings Alopecia areata unmet need persists Key Findings From Survey of 50 U.S. Dermatology Healthcare Providers “There's a large unmet need. Many patients don't 1 on Unmet Need want JAK inhibitors and there are no other advanced options for them. Improved safety profile (no black box warning) - US Dermatologist, Community Practice Minimal lab monitoring requirements “There’s no middle ground for ease of access, safety, and efficacy in current therapies—either a benign topical or a chronic pill with a black box warning—and many patients remain on subpar therapies due to More durable efficacy hesitation around JAKi side effect risks.” - US Dermatologist, Community Practice 1 20 Survey conducted by IQVIA on behalf of Company
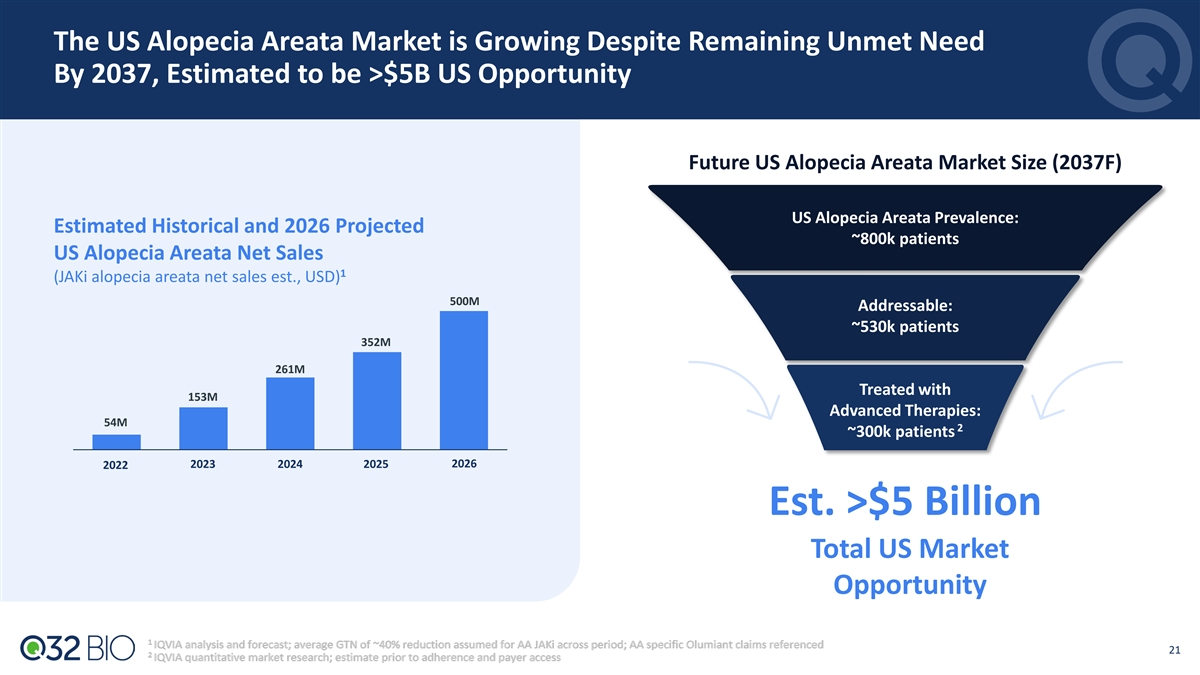
The US Alopecia Areata Market is Growing Despite Remaining Unmet Need By 2037, Estimated to be >$5B US Opportunity Future US Alopecia Areata Market Size (2037F) US Alopecia Areata Prevalence: Estimated Historical and 2026 Projected ~800k patients US Alopecia Areata Net Sales 1 (JAKi alopecia areata net sales est., USD) 500M Addressable: ~530k patients 352M 261M Treated with 153M Advanced Therapies: 54M 2 ~300k patients 2026 2022 2023 2024 2025 Est. >$5 Billion Total US Market Opportunity 21
Bempikibart SIGNAL-AA Program In Severe/Very Severe Alopecia Areata Supports Registration-Directed Program Bempikibart for Alopecia Areata Next Steps • Alopecia areata is a large and underserved • Results from ongoing Part B and totality of data from patient population with significant unmet need SIGNAL-AA program supports advancement into a registration-directed program • Proof-of-concept with durable response and safe redosing observed in SIGNAL-AA Part A • SIGNAL-AA Part B full results to be presented at a future medical meeting • Meaningful efficacy data and well-tolerated safety profile with 36-week dosing in • Q32 to engage with FDA on proposed registration- SIGNAL-AA Part B directed program with plans to initiate in 1H27 • Favorable safety and tolerability profile with • Pediatric and moderate population plans low rates of ISRs across SIGNAL-AA program under development • Evaluation of additional I&I indications ongoing Differentiated target product profile of bempikibart supports the potential to become standard of care as an efficacious, durable and safe targeted biologic therapy for the treatment of alopecia areata ISR = Injection Site Reaction 22

Q&A with Renowned Alopecia Areata Key Opinion Leader Q32 Bio Leadership Jodie Morrison Shelia Violette, Ph.D. Lee Kalowski, M.B.A. Chief Executive Officer Founder & President & Chief Scientific Officer Chief Financial Officer Key Opinion Leader Arash Mostaghimi, MD, MPA, MPH Associate Professor of Dermatology and Vice Chair of Clinical Trials and Innovation, Brigham and Women’s Hospital, Harvard Medical School 23
SIGNAL-AA Part B 36-Week Topline Results July 2026