
Exhibit 99.1
1 Nasdaq: CMPX Bringing Transformative Oncology Therapies to Patients Corporate Presentation I July 2026
2 This presentation has been prepared by Compass Therapeutics, Inc . ("we," "us," "our," or the “Company”) . Statements contained herein are made as of the date of this presentation unless stated otherwise, and this presentation shall not under any circumstances create an implication that the information contained herein is correct as of any time after such date or that information will be updated or revised to reflect information that subsequently becomes available or changes occurring after the date hereof . This presentation contains forward - looking statements. Statements in this presentation that are not purely historical are forwar d - looking statements. Such forward - looking statements include, among other things, references to Compass's financial position to continue advancing its product candidates, expectations abo ut cash runway, business and development plans, and statements regarding Compass's product candidates, including their preclinical and clinical development, therapeutic potentia l a nd tolerability profile, and clinical trial milestones such as the expected trial design, timing of enrollment, patient dosing and data readouts, regulatory plans and the timing and nature of any regulatory interactions and subsequent approval pathways for any potential indications with respect to Compass's product candidates and the therapeutic potential thereof. Actual results cou ld differ from those projected in any forward - looking statements due to numerous factors. Such factors include, among others, Compass's ability to raise the additional funding it wil l need to continue to pursue its business and product development plans, the inherent uncertainties associated with developing product candidates and operating as a development st age company, Compass's ability to identify additional product candidates for development, Compass's ability to develop, initiate and complete clinical trials for, obtain approvals for and co mmercialize any of its product candidates, competition in the industry in which Compass operates and market conditions. These forward - looking statements are made as of the date of this prese ntation, and Compass assumes no obligation to update the forward - looking statements, or to update the reasons why actual results could differ from those projected in the forward - looking statements, except as required by law. Investors should consult all of the information set forth herein and should also refer to the risk factor disclosure set forth in the reports and other documents Compass files with the U.S. Securities and Exchange Commission (SEC) available at www.sec.gov, including without limitation Compass's latest Annual Report on Form 10 - K, Quarterly R eport on Form 10 - Q and subsequent filings with the SEC. This presentation also contains estimates and other statistical data made by independent parties and by us relating to market size and growth and other data about our industry . This data involves a number of assumptions and limitations, and you are cautioned not to give undue weight to such estimates . In addition, projections, assumptions, and estimates of our future performance and the future performance of the markets in which we operate are necessarily subject to a high degree of uncertainty and risk . This presentation concerns drugs that are under clinical investigation, and which have not yet been approved for marketing by the U . S . Food and Drug Administration (FDA) . It is currently limited by Federal law to investigational use, and no representation is made as to its safety or effectiveness for the purposes for which it is being investigated . DISCLAIMER
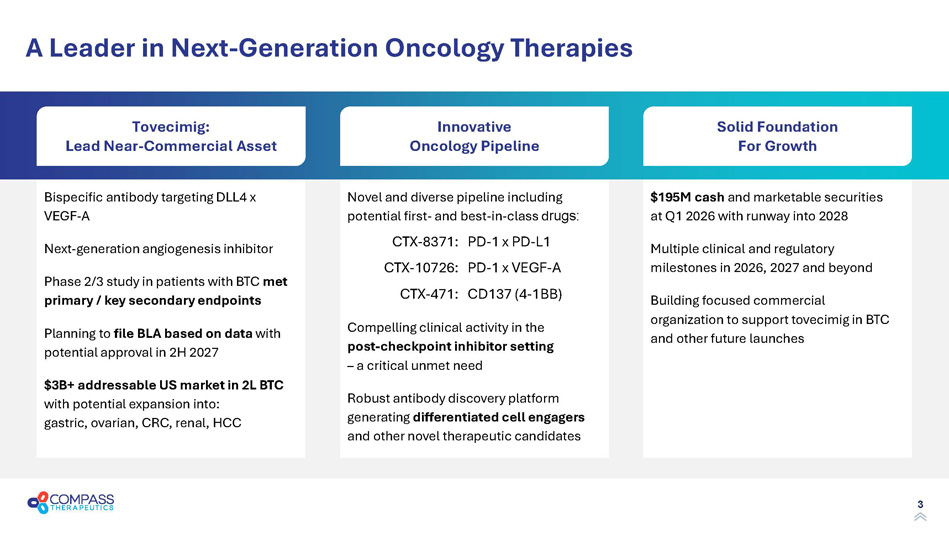
3 A Leader in Next - Generation Oncology Therapies Bispecific antibody targeting DLL4 x VEGF - A Next - generation angiogenesis inhibitor Phase 2/3 study in patients with BTC met primary / key secondary endpoints Planning to file BLA based on data with potential approval in 2H 2027 $3B+ addressable US market in 2L BTC with potential expansion into: gastric, ovarian, CRC, renal, HCC Novel and diverse pipeline including potential first - and best - in - class d rugs: CTX - 8371: PD - 1 x PD - L1 CTX - 10726: PD - 1 x VEGF - A CTX - 471: CD137 (4 - 1BB) Compelling clinical activity in the post - checkpoint inhibitor setting – a critical unmet need Robust antibody discovery platform generating differentiated cell engagers and other novel therapeutic candidates $ 195 M cash and marketable securities at Q1 2026 with runway into 2028 Multiple clinical and regulatory milestones in 2026, 2027 and beyond Building focused commercial organization to support tovecimig in BTC and other future launches Solid Foundation For Growth Innovative Oncology Pipeline Tovecimig : Lead Near - Commercial Asset
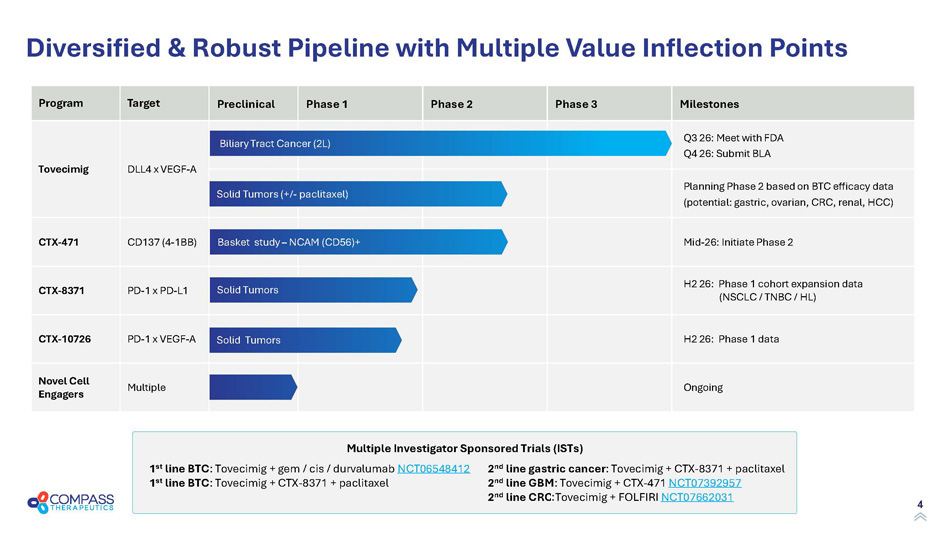
4 Milestones Phase 3 Phase 2 Phase 1 Preclinical Target Program Q3 26: Meet with FDA Q4 26: Submit BLA DLL4 x VEGF - A Tovecimig Planning Phase 2 based on BTC efficacy data (potential: g astric , ovarian, CRC, renal, HCC) Mid - 26: Initiate Phase 2 CD137 (4 - 1BB) CTX - 471 H2 26: Phase 1 cohort expansion data ( NSCLC / TNBC / HL) PD - 1 x PD - L1 CTX - 8371 H2 26: Phase 1 data PD - 1 x VEGF - A CTX - 10726 Ongoing Multiple Novel Cell Engagers Diversified & Robust Pipeline with Multiple Value Inflection Points Solid Tumors Solid Tumors (+/ - paclitaxel) Biliary Tract Cancer (2L) Solid Tumors Basket study – NCAM (CD56)+ Multiple Investigator Sponsored Trials (ISTs) 1 st line BTC : Tovecimig + gem / cis / durvalumab NCT06548412 1 st line BTC : Tovecimig + CTX - 8371 + paclitaxel 2 nd line gastric cancer : Tovecimig + CTX - 8371 + paclitaxel 2 nd line GBM : Tovecimig + CTX - 471 NCT07392957 2 nd line CRC Tovecimig + FOLFIRI NCT07662031

5 Nasdaq: CMPX Tovecimig (CTX - 009) DLL4 X VEGF - A bispecific antibody
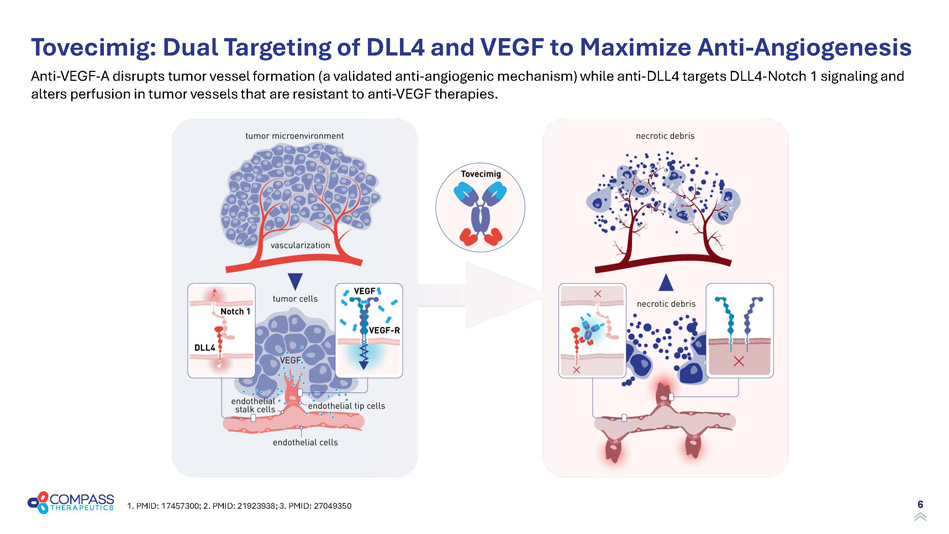
6 Tovecimig : Dual Targeting of DLL4 and VEGF to Maximize Anti - Angiogenesis 1. PMID: 17457300; 2. PMID: 21923938; 3. PMID: 27049350 Anti - VEGF - A disrupts tumor vessel formation (a validated anti - angiogenic mechanism) while anti - DLL4 targets DLL4 - Notch 1 signali ng and alters perfusion in tumor vessels that are resistant to anti - VEGF therapies.
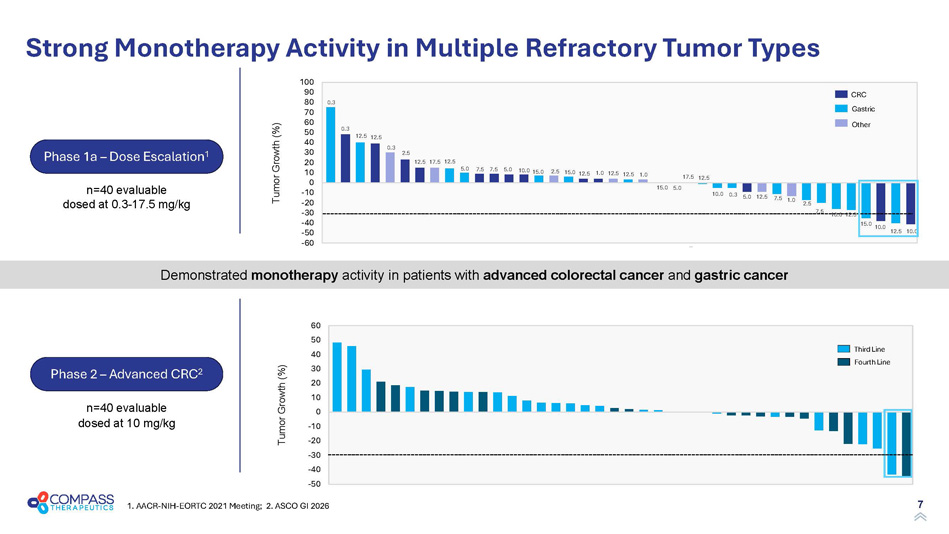
7 n=40 evaluable dosed at 0.3 - 17.5 mg/kg n=40 evaluable dosed at 10 mg/kg Demonstrated monotherapy activity in patients with advanced colorectal cancer and gastric cancer -50 -40 -30 -20 -10 0 10 20 30 40 50 60 Strong Monotherapy Activity in Multiple Refractory Tumor Types 1. AACR - NIH - EORTC 2021 Meeting; 2. ASCO GI 2026 Tumor Growth (%) Fourth Line Third Line Tumor Growth (%) -60 -50 -40 -30 -20 -10 0 10 20 30 40 50 60 70 80 90 100 12.5 12.5 10.0 0.3 5.0 12.5 7.5 10.0 12.5 10.0 15.0 12.5 10.0 7.5 1.0 2.5 12.5 12.5 0.3 2.5 12.5 17.5 12.5 5.0 7.5 7.5 5.0 10.0 15.0 2.5 15.0 12.5 1.0 1.0 15.0 5.0 17.5 12.5 0.3 0.3 CRC Gastric Other Phase 2 – Advanced CRC 2 Phase 1a – Dose Escalation 1
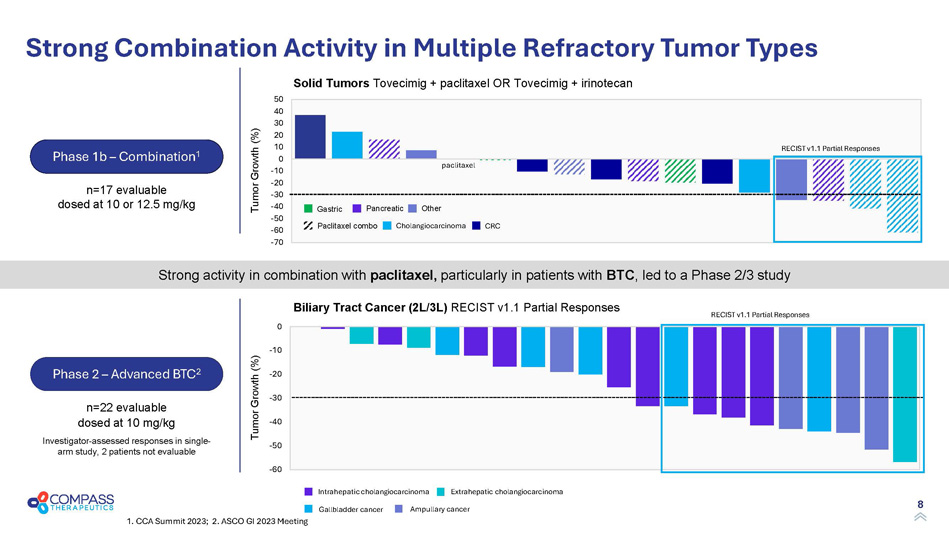
8 Strong activity in combination with paclitaxel, particularly in patients with BTC , led to a Phase 2/3 study Strong Combination Activity in Multiple Refractory Tumor Types 1. CCA Summit 2023; 2. ASCO GI 2023 Meeting Phase 2 – Advanced BTC 2 Investigator - assessed responses in single - arm study, 2 patients not evaluable Biliary Tract Cancer (2L/3L) RECIST v1.1 Partial Responses n=17 evaluable dosed at 10 or 12.5 mg/kg n=22 evaluable dosed at 10 mg/kg Tumor Growth (%) Tumor Growth (%) -70 -60 -50 -40 -30 -20 -10 0 10 20 30 40 50 Solid Tumors Tovecimig + paclitaxel OR Tovecimig + irinotecan RECIST v1.1 Partial Responses Phase 1b – Combination 1 Gastric Pancreatic Other Paclitaxel combo Cholangiocarcinoma CRC Gallbladder cancer Ampullary cancer Intrahepatic cholangiocarcinoma Extrahepatic cholangiocarcinoma RECIST v1.1 Partial Responses paclitaxel -60 -50 -40 -30 -20 -10 0
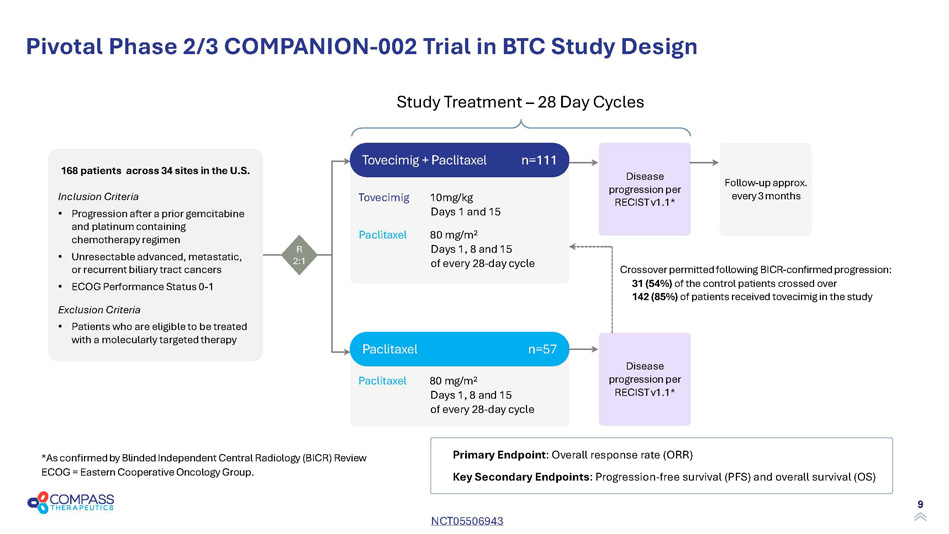
9 Paclitaxel 80 mg/m 2 Days 1, 8 and 15 of every 28 - day cycle Tovecimig 10mg/kg Days 1 and 15 Paclitaxel 80 mg/m 2 Days 1, 8 and 15 of every 28 - day cycle Pivotal Phase 2/3 COMPANION - 002 Trial in BTC Study Design * As confirmed by Blinded Independent Central Radiology (BICR) Review ECOG = Eastern Cooperative Oncology Group. Crossover permitted following BICR - confirmed progression: 31 (54%) of the control patients crossed over 142 (85%) of patients received tovecimig in the study Study Treatment – 28 Day Cycles Tovecimig + Paclitaxel n=111 Paclitaxel n=57 Disease p rogression per RECIST v 1.1 * Primary Endpoint : Overall response rate (ORR) Key S econdary E ndpoints : Progression - free survival (PFS) and overall survival (OS) R 2:1 Follow - up approx. every 3 months Disease p rogression per RECIST v 1.1 * 168 patients across 34 sites in the U.S. Inclusion Criteria • Progression after a prior gemcitabine and platinum containing chemotherapy regimen • Unresectable advanced, metastatic, or recurrent biliary tract cancers • ECOG Performance Status 0 - 1 Exclusion Criteria • Patients who are eligible to be treated with a molecularly targeted therapy NCT05506943
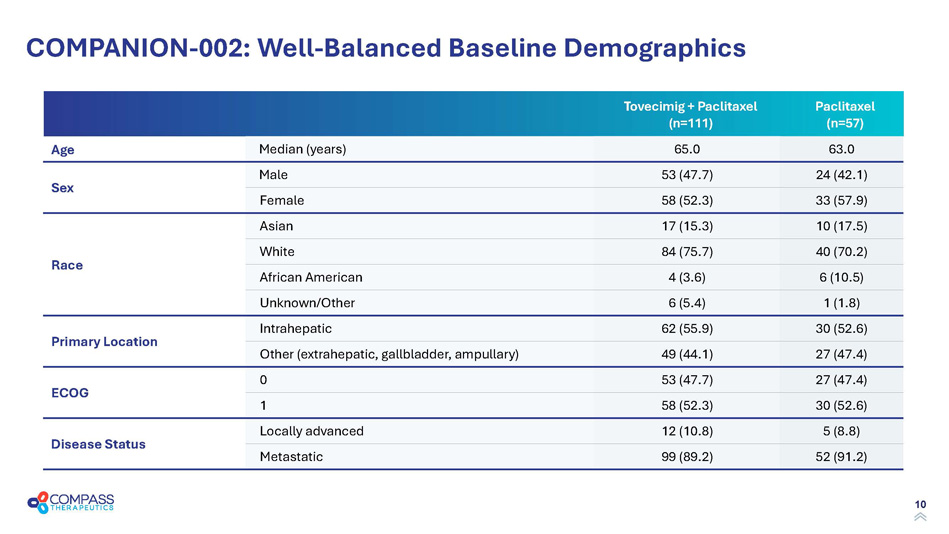
10 COMPANION - 002: Well - Balanced Baseline Demographics Paclitaxel (n=57) Tovecimig + Paclitaxel (n=111) 63.0 65.0 Median (years) Age 24 (42.1) 53 (47.7) Male Sex 33 (57.9) 58 (52.3) Female 10 (17.5) 17 (15.3) Asian Race 40 (70.2) 84 (75.7) White 6 (10.5) 4 (3.6) African American 1 (1.8) 6 (5.4) Unknown/Other 30 (52.6) 62 (55.9) Intrahepatic Primary Location 27 (47.4) 49 (44.1) Other (extrahepatic, gallbladder, ampullary) 27 (47.4) 53 (47.7) 0 ECOG 30 (52.6) 58 (52.3) 1 5 (8.8) 12 (10.8) Locally advanced Disease Status 52 (91.2) 99 (89.2) Metastatic
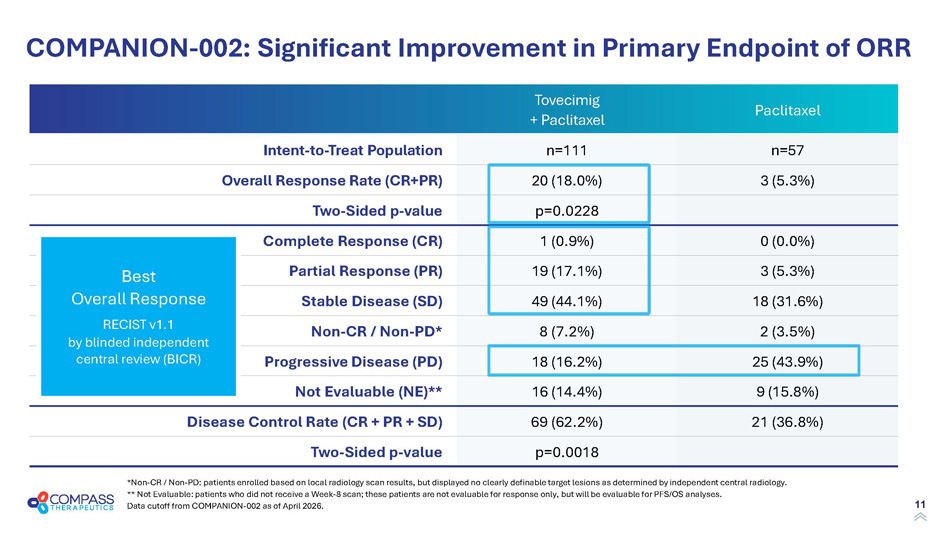
11 Paclitaxel Tovecimig + Paclitaxel n=57 n=111 Intent - to - Treat Population 3 (5.3%) 20 (18.0%) Overall Response Rate (CR+PR) p=0.0228 Two - Sided p - value 0 (0.0%) 1 (0.9%) Complete Response (CR) 3 (5.3%) 19 (17.1%) Partial Response (PR) 18 (31.6%) 49 (44.1%) Stable Disease (SD) 2 (3.5%) 8 (7.2%) Non - CR / Non - PD* 25 (43.9%) 18 (16.2%) Progressive Disease (PD) 9 (15.8%) 16 (14.4%) Not Evaluable (NE)** 21 (36.8%) 69 (62.2%) Disease Control Rate (CR + PR + SD) p=0.0018 Two - Sided p - value COMPANION - 002: Significant Improvement in Primary Endpoint of ORR *Non - CR / Non - PD: patients enrolled based on local radiology scan results, but displayed no clearly definable target lesions as determined by independent central radiology. ** Not Evaluable: patients who did not receive a Week - 8 scan; these patients are not evaluable for response only, but will be ev aluable for PFS/OS analyses. Data cutoff from COMPANION - 002 as of April 2026. Best Overall Response RECIST v1.1 by blinded independent central review (BICR)
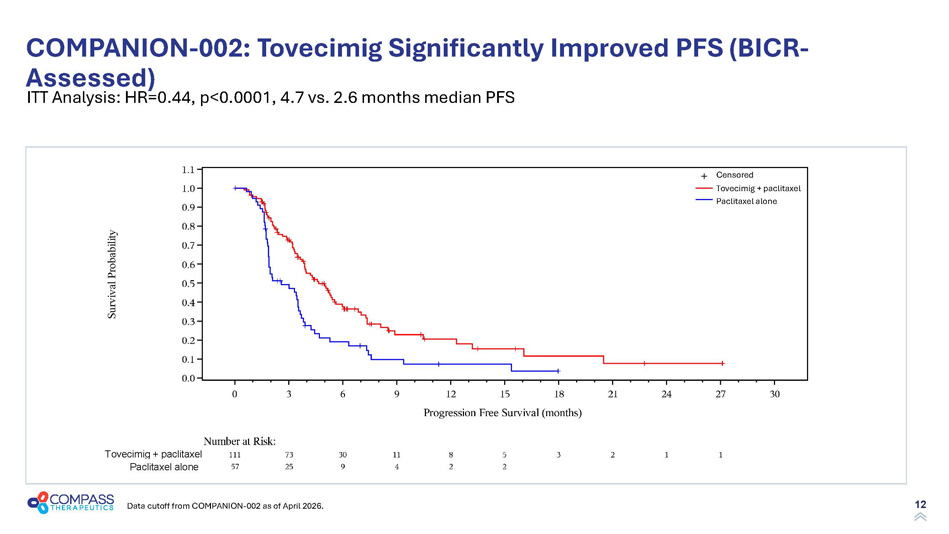
12 COMPANION - 002: Tovecimig Significantly Improved PFS (BICR - Assessed) Data cutoff from COMPANION - 002 as of April 2026. Tovecimig + paclitaxel Paclitaxel alone Censored Tovecimig + paclitaxel Paclitaxel alone ITT Analysis: HR=0.44, p<0.0001, 4.7 vs. 2.6 months median PFS
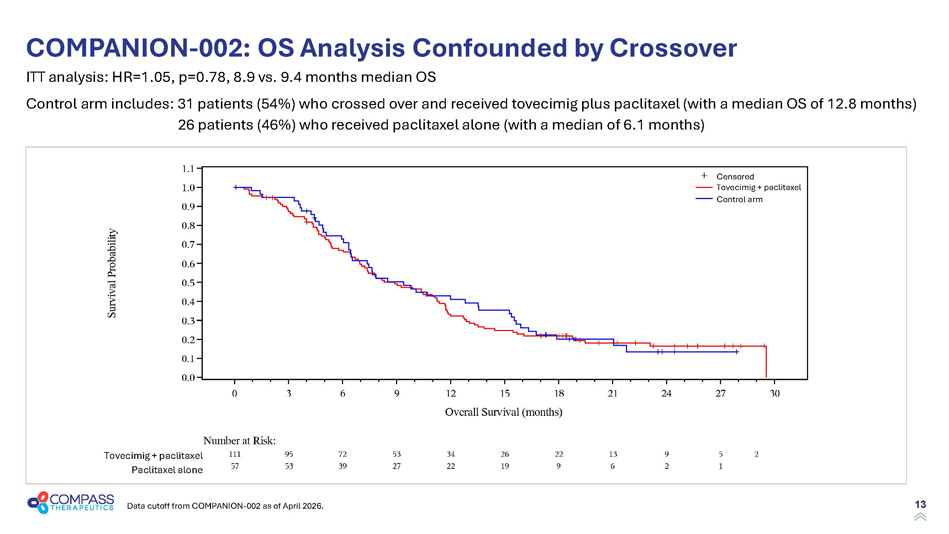
13 COMPANION - 002: OS Analysis Confounded by Crossover Data cutoff from COMPANION - 002 as of April 2026. ITT analysis: HR=1.05, p=0.78, 8.9 vs. 9.4 months median OS Control arm includes: 31 patients (54%) who crossed over and received tovecimig plus paclitaxel (with a median OS of 12.8 months) 26 patients (46%) who received paclitaxel alone (with a median of 6.1 months) Tovecimig + paclitaxel Paclitaxel alone Tovecimig + paclitaxel Control arm Censored
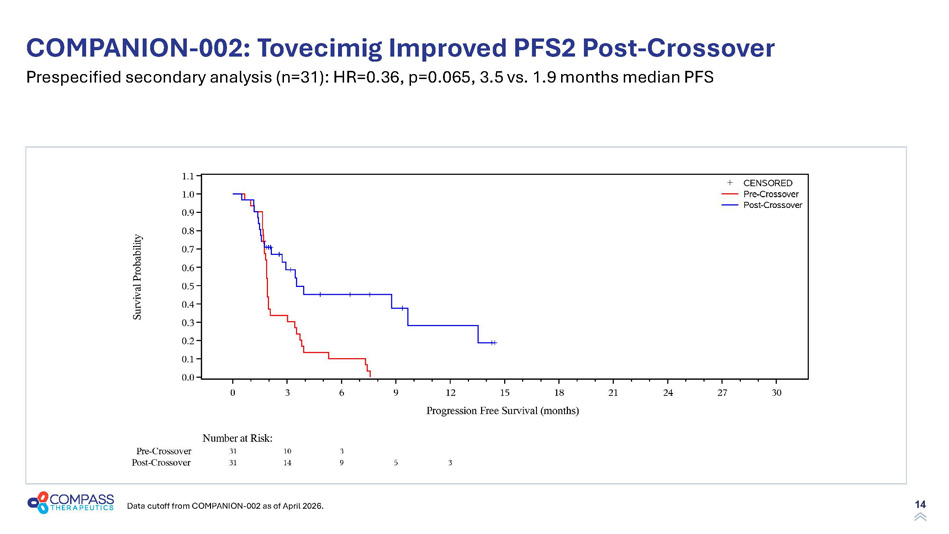
14 COMPANION - 002: Tovecimig Improved PFS2 Post - Crossover Data cutoff from COMPANION - 002 as of April 2026. Prespecified secondary analysis (n=31): HR=0.36, p =0.065, 3.5 vs. 1.9 months median PFS
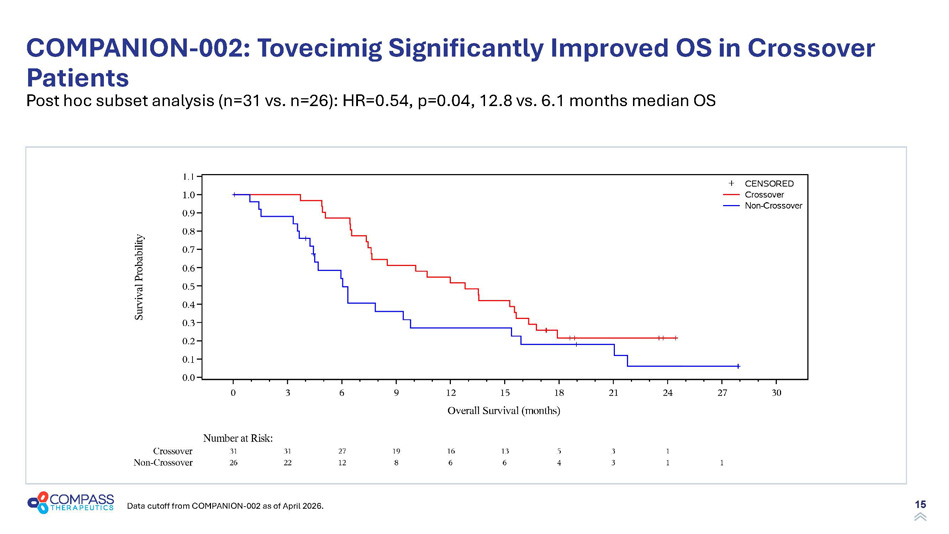
15 COMPANION - 002: Tovecimig Significantly Improved OS in Crossover Patients Data cutoff from COMPANION - 002 as of April 2026. Post hoc subset analysis (n=31 vs. n=26): HR=0.54, p=0.04, 12.8 vs. 6.1 months median OS
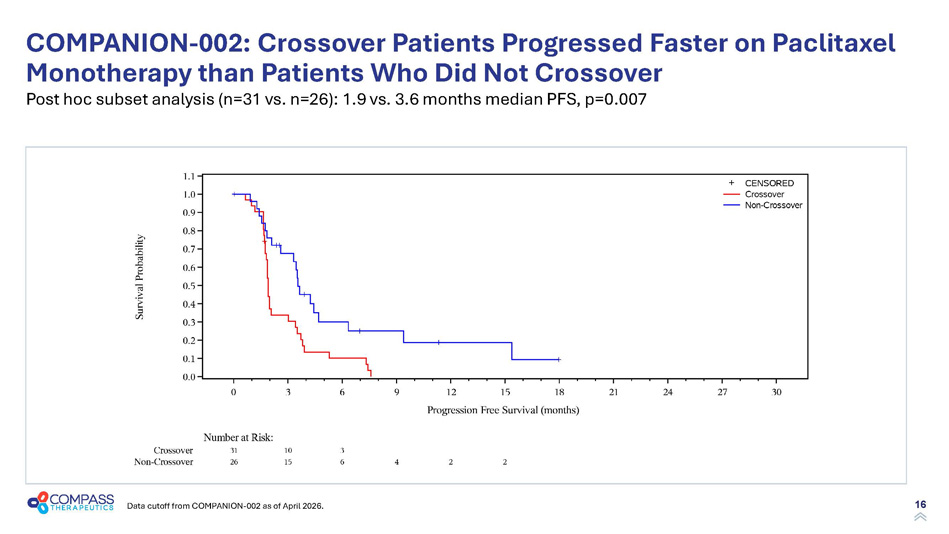
16 COMPANION - 002: Crossover Patients Progressed Faster on Paclitaxel Monotherapy than Patients Who Did Not Crossover Data cutoff from COMPANION - 002 as of April 2026. Post hoc subset analysis (n=31 vs. n=26): 1.9 vs. 3.6 months median PFS, p=0.007
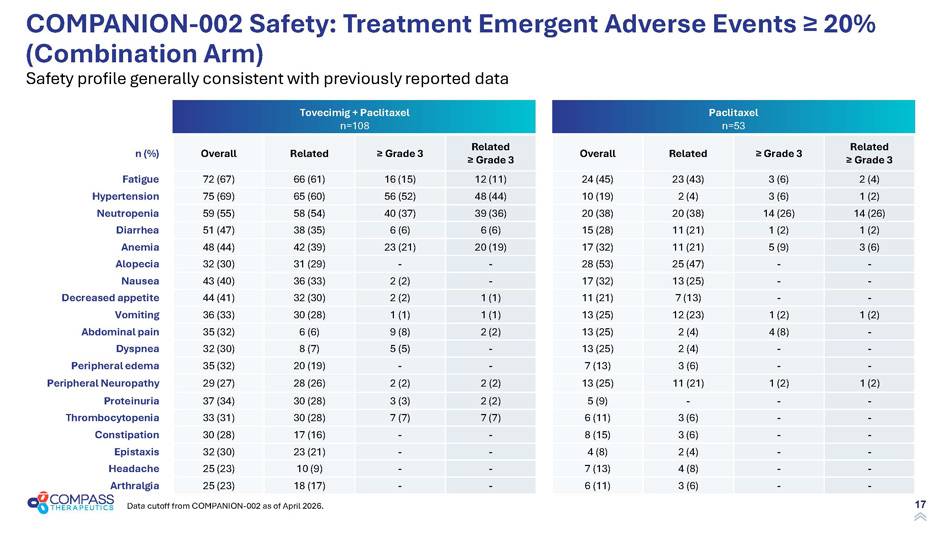
17 Paclitaxel n=53 Tovecimig + Paclitaxel n=108 Related ≥ Grade 3 ≥ Grade 3 Related Overall Related ≥ Grade 3 ≥ Grade 3 Related Overall n (%) 2 (4) 3 (6) 23 (43) 24 (45) 12 (11) 16 (15) 66 (61) 72 (67) Fatigue 1 (2) 3 (6) 2 (4) 10 (19) 48 (44) 56 (52) 65 (60) 75 (69) Hypertension 14 (26) 14 (26) 20 (38) 20 (38) 39 (36) 40 (37) 58 (54) 59 (55) Neutropenia 1 (2) 1 (2) 11 (21) 15 (28) 6 (6) 6 (6) 38 (35) 51 (47) Diarrhea 3 (6) 5 (9) 11 (21) 17 (32) 20 (19) 23 (21) 42 (39) 48 (44) Anemia - - 25 (47) 28 (53) - - 31 (29) 32 (30) Alopecia - - 13 (25) 17 (32) - 2 (2) 36 (33) 43 (40) Nausea - - 7 (13) 11 (21) 1 (1) 2 (2) 32 (30) 44 (41) Decreased appetite 1 (2) 1 (2) 12 (23) 13 (25) 1 (1) 1 (1) 30 (28) 36 (33) Vomiting - 4 (8) 2 (4) 13 (25) 2 (2) 9 (8) 6 (6) 35 (32) Abdominal pain - - 2 (4) 13 (25) - 5 (5) 8 (7) 32 (30) Dyspnea - - 3 (6) 7 (13) - - 20 (19) 35 (32) Peripheral edema 1 (2) 1 (2) 11 (21) 13 (25) 2 (2) 2 (2) 28 (26) 29 (27) Peripheral Neuropathy - - - 5 (9) 2 (2) 3 (3) 30 (28) 37 (34) Proteinuria - - 3 (6) 6 (11) 7 (7) 7 (7) 30 (28) 33 (31) Thrombocytopenia - - 3 (6) 8 (15) - - 17 (16) 30 (28) Constipation - - 2 (4) 4 (8) - - 23 (21) 32 (30) Epistaxis - - 4 (8) 7 (13) - - 10 (9) 25 (23) Headache - - 3 (6) 6 (11) - - 18 (17) 25 (23) Arthralgia COMPANION - 002 Safety: Treatment Emergent Adverse Events ≥ 20% (Combination Arm) Data cutoff from COMPANION - 002 as of April 2026. Safety profile generally consistent with previously reported data
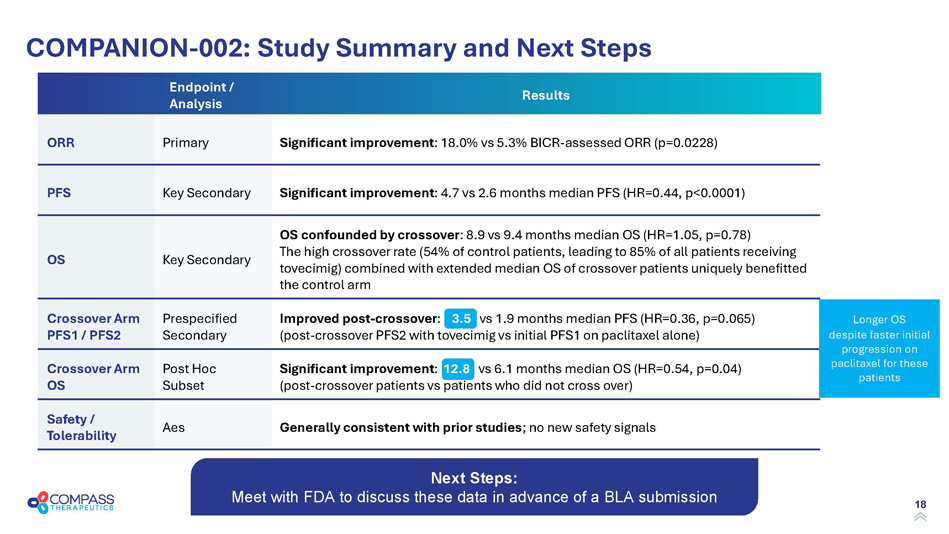
18 COMPANION - 002: Study Summary and Next Steps Results Endpoint / Analysis Significant improvement : 18.0% vs 5.3% BICR - assessed ORR (p=0.0228) Primary ORR Significant improvement : 4.7 vs 2.6 months median PFS (HR=0.44, p<0.0001) Key Secondary PFS OS confounded by crossover : 8.9 vs 9.4 months median OS (HR=1.05, p=0.78) The high crossover rate (54% of control patients, leading to 85% of all patients receiving tovecimig ) combined with extended median OS of crossover patients uniquely benefitted the control arm Key Secondary OS Improved post - crossover : 3.5 vs 1.9 months median PFS (HR=0.36, p=0.065) (post - crossover PFS2 with tovecimig vs initial PFS1 on paclitaxel alone) Prespecified Secondary Crossover Arm PFS1 / PFS2 Significant improvement : 12.8 vs 6.1 months median OS (HR=0.54, p=0.04) (post - crossover patients vs patients who did not cross over) Post Hoc Subset Crossover Arm OS Generally consistent with prior studies ; no new safety signals Aes Safety / Tolerability Longer OS despite faster initial progression on paclitaxel for these patients Next Steps: Meet with FDA to discuss these data in advance of a BLA submission
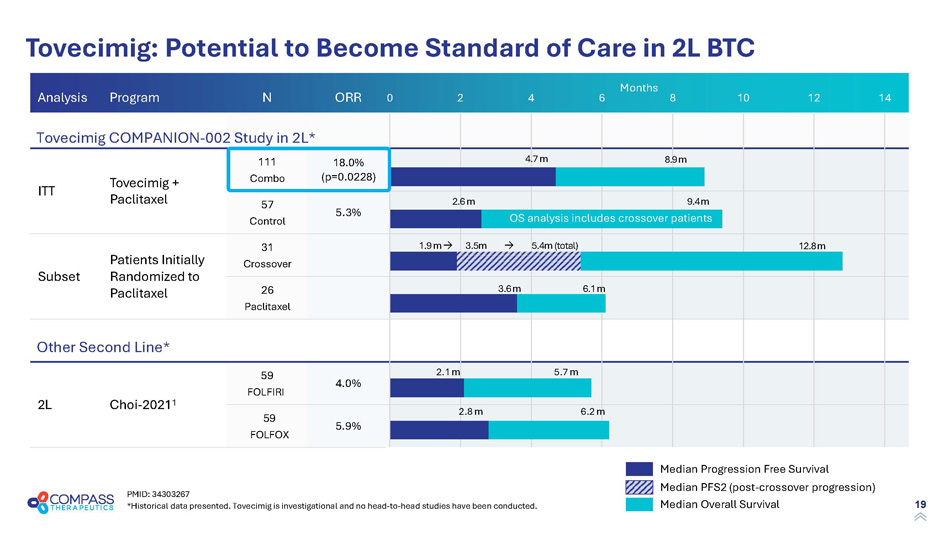
19 ORR N Program Analysis 18.0% (p=0.0228) 111 Combo Tovecimig + Paclitaxel ITT 5.3% 57 Control 31 Crossover Patients Initially Randomized to Paclitaxel Subset 26 Paclitaxel 4.0% 59 FOLFIRI Choi - 2021 1 2L 5.9% 59 FOLFOX 0 2 4 6 8 10 12 14 Tovecimig: Potential to Become Standard of Care in 2L BTC PMID: 34303267 *Historical data presented. Tovecimig is investigational and no head - to - head studies have been conducted. Months Tovecimig COMPANION - 002 Study in 2L* Other Second Line* Median Progression Free Survival Median Overall Survival Median PFS2 (post - crossover progression) 8.9 m 4.7 m 2.6 m 9.4 m 2.1 m 2.8 m 6.2 m 5.7 m 12.8 m 1.9 m 3.5m 5.4m (total) 3.6 m 6.1 m OS analysis includes crossover patients

20 Nasdaq: CMPX Tovecimig (CTX - 009) Commercial Opportunity
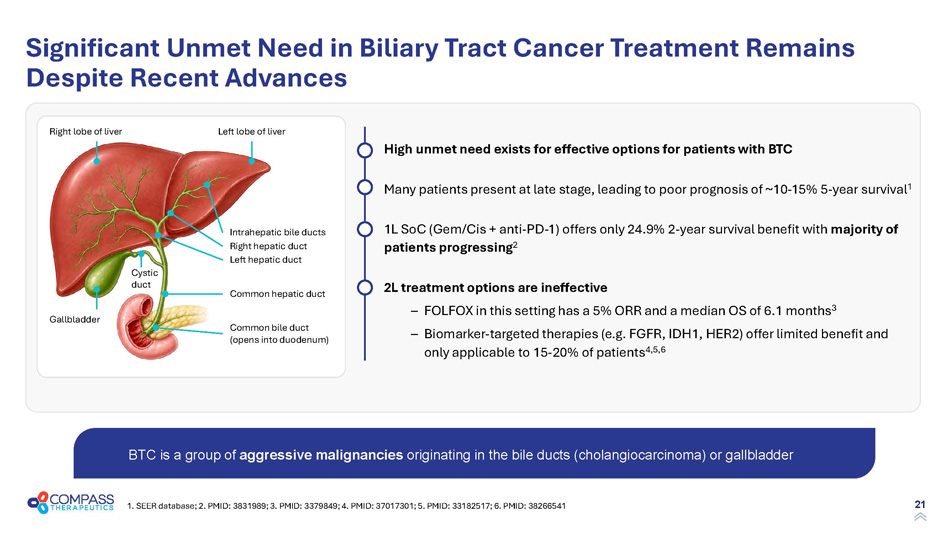
21 Significant Unmet Need in Biliary Tract Cancer Treatment Remains Despite Recent Advances BTC is a group of aggressive malignancies originating in the bile ducts (cholangiocarcinoma) or gallbladder Common hepatic duct Left hepatic duct Right hepatic duct Intrahepatic bile ducts Right lobe of liver Gallbladder Cystic duct Common bile duct (opens into duodenum) Left lobe of liver 1. SEER database; 2. PMID: 3831989; 3. PMID: 3379849; 4. PMID: 37017301; 5. PMID: 33182517; 6. PMID: 38266541 High unmet need exists for effective options for patients with BTC Many patients present at late stage, leading to poor prognosis of ~10 - 15% 5 - year survival 1 1L SoC (Gem/Cis + anti - PD - 1) offers only 24.9% 2 - year survival benefit with majority of patients progressing 2 2L treatment options are ineffective – FOLFOX in this setting has a 5% ORR and a median OS of 6.1 months 3 – Biomarker - targeted therapies (e.g. FGFR, IDH1, HER2) offer limited benefit and only applicable to 15 - 20% of patients 4,5,6
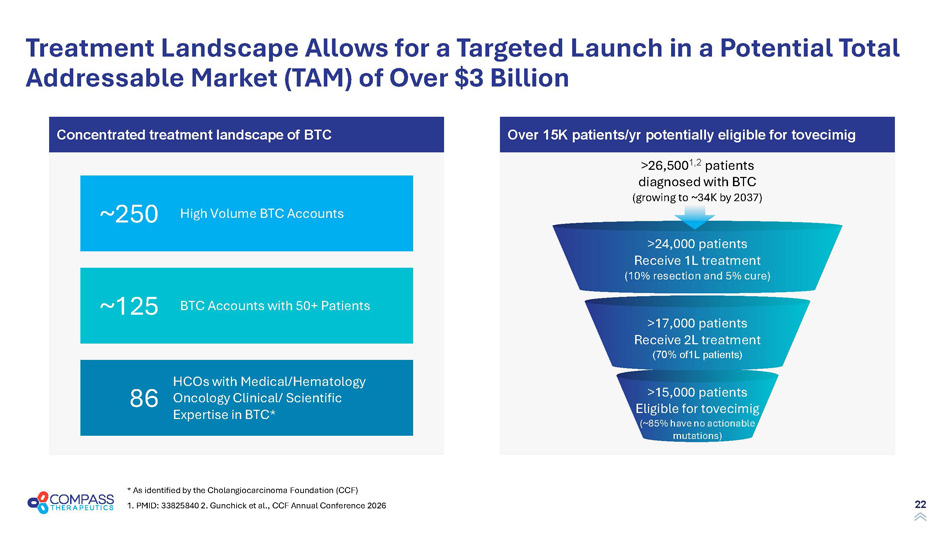
22 Treatment Landscape Allows for a Targeted Launch in a Potential Total Addressable Market (TAM) of Over $3 Billion * As identified by the Cholangiocarcinoma Foundation (CCF) Over 15K patients/yr potentially eligible for tovecimig Concentrated treatment landscape of BTC >26,500 1,2 patients diagnosed with BTC (growing to ~34K by 2037) >24,000 patients Receive 1L treatment (10% resection and 5% cure) >17,000 patients Receive 2L treatment (70% of1L patients) >15,000 patients Eligible for tovecimig (~85% have no actionable mutations) ~250 ~125 86 High Volume BTC Accounts BTC Accounts with 50+ Patients HCOs with Medical/Hematology Oncology Clinical/ Scientific Expertise in BTC* 1. PMID: 33825840 2. Gunchick et al., CCF Annual Conference 2026
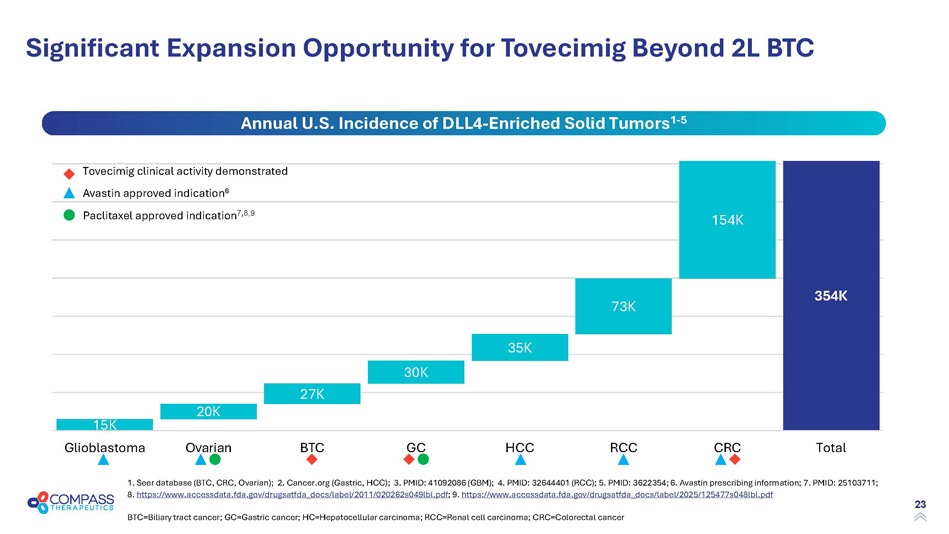
23 Significant Expansion Opportunity for Tovecimig Beyond 2L BTC 1. Seer database (BTC, CRC, Ovarian); 2. Cancer.org (Gastric, HCC); 3. PMID: 41092086 (GBM); 4. PMID: 32644401 (RCC); 5. PMID: 3622354; 6. Avastin prescribing information; 7. PM ID: 25103711; 8. https://www.accessdata.fda.gov/drugsatfda_docs/label/2011/020262s049lbl.pdf ; 9. https://www.accessdata.fda.gov/drugsatfda_docs/label/2025/125477s048lbl.pdf 15 K 20 K 27 K 30 K 35 K 73 K 154 K 354 K Glioblastoma Ovarian BTC GC HCC RCC CRC Total Annual U.S. Incidence of DLL4 - Enriched Solid Tumors 1 - 5 Tovecimig clinical activity demonstrated Avastin approved indication 6 Paclitaxel approved indication 7 , 8,9 BTC=Biliary tract cancer; GC=Gastric cancer; HC=Hepatocellular carcinoma; RCC=Renal cell carcinoma; CRC=Colorectal cancer
24 Tovecimig – Advancing to Approval in BTC and Beyond Strong Clinical Data in a Difficult Indication Robust evidence of activity in patients with BTC Generally well tolerated, with no new safety signal No approved therapeutics for most patients in 2L setting Near - Term Regulatory Milestones Expected FDA meeting in Q3 2026 BLA filing initiating in late 2026 2027 potential approval and launch Multi - $B Market / Expansion Opportunities Highly focused US BTC market; targeted launch prep underway Substantial ex - US opportunities with higher incidence Other DLL4+ indications: gastric, ovarian, CRC, renal, HCC

25 Nasdaq: CMPX CTX - 8371 PD - 1 x PD - L1 bispecific antibody
26 1. PMID: 39887747; 2. PMID: 36636451; 3. https:// www.healio.com /news/hematology - oncology/20250327/only - 1 - in - 5 - people - treated - with - immune - checkpoint - inhibitors - respond - to - therapy; 4. https://www.gminsights.com/industry - analysis/immune - checkpoint - inhibitors - market ; 5. https://www.futuremarketinsights.com/reports/checkpoint - inhibitor - refractory - cancer - market PD - 1 and PD - L1 are Validated Targets That Have Transformed Oncology, Yet Unmet Needs Remain CPIs transformed oncology ~57% of advanced cancer patients are eligible for checkpoint therapy 1 Checkpoint inhibitors (CPIs) are approved in 20+ tumor types and 80+ lines / indications 2,3 Post - CPI patients have poor prognoses and limited alternatives ~80% of CPI - treated patients do not respond or have tumors later progress 1 Increased 1L use of CPIs led to a large and growing number of patients who progress after CPI with no clear standard of care $40B+ $30B+ $60B+ estimated WW CPI refractory market potential 5 CPI U.S. sales 4 CPI WW sales 4
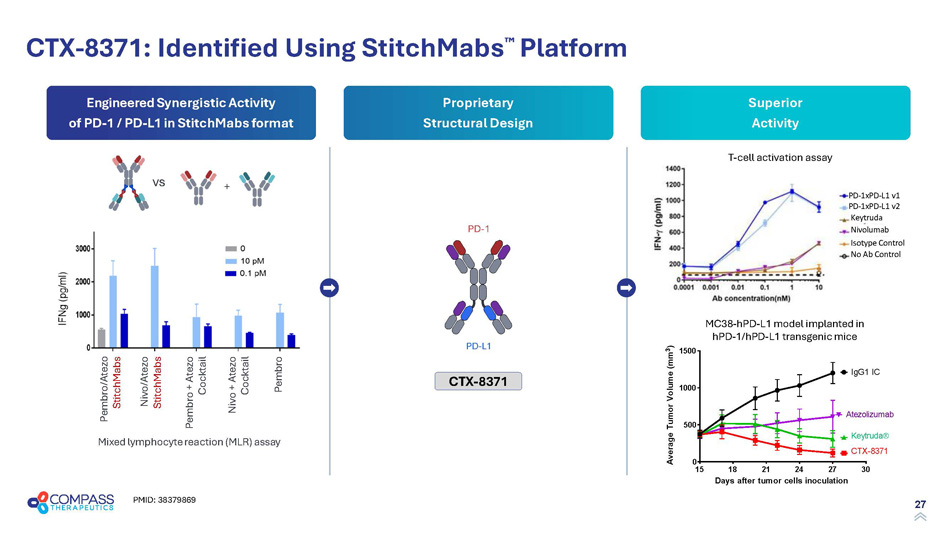
27 Superior Activity Proprietary Structural Design Engineered S ynergistic A ctivity of PD - 1 / PD - L1 in StitchMabs format CTX - 8371: Identified Using StitchMabs Platform Mixed lymphocyte reaction (MLR) assay Pembro / Atezo Stitch M ab s Nivo / Atezo Stitch M ab s Pembro + Atezo Cocktail Nivo + Atezo Cocktail Pembro vs + T - cell activation assay MC38 - hPD - L1 model implanted in hPD - 1/hPD - L1 transgenic mice PD - 1 PD - L1 CTX - 8371 PMID: 38379869
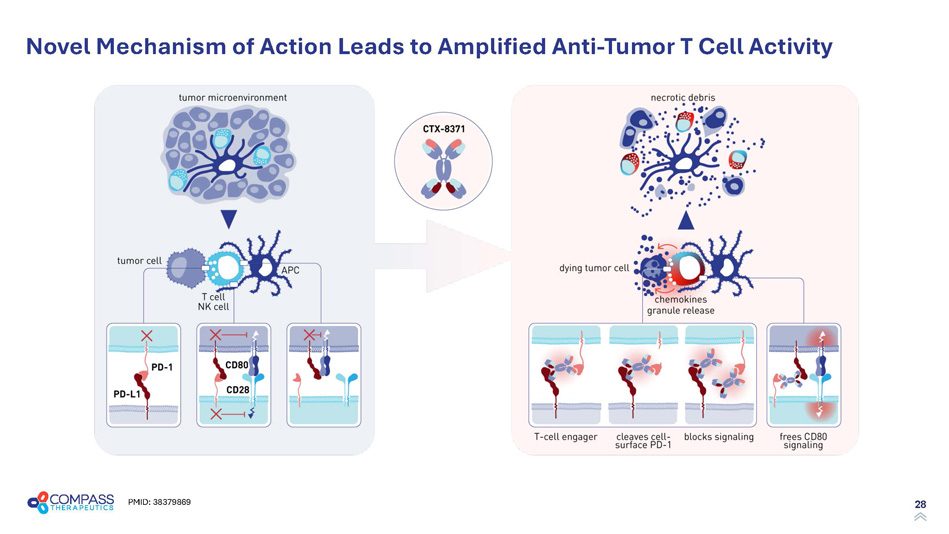
28 Novel Mechanism of Action Leads to Amplified Anti - Tumor T Cell Activity PMID: 38379869
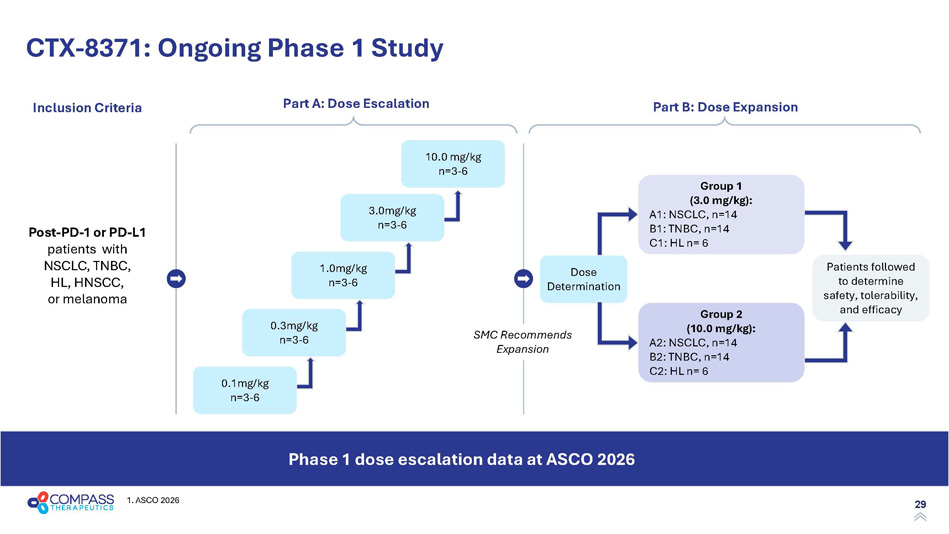
29 CTX - 8371: Ongoing Phase 1 Study Phase 1 dose escalation data at ASCO 2026 Inclusion Criteria Post - PD - 1 or PD - L1 patients with NSCLC, TNBC, HL, HNSCC, or melanoma Part A: Dose Escalation Part B: Dose Expansion 0.1mg/kg n=3 - 6 0.3mg/kg n=3 - 6 1.0mg/kg n=3 - 6 3.0mg/kg n=3 - 6 10.0 mg/kg n=3 - 6 Dose Determination Group 1 (3.0 mg/kg): A1: NSCLC, n=14 B1: TNBC, n=14 C1: HL n= 6 Group 2 (10.0 mg/kg): A2: NSCLC, n=14 B2: TNBC, n=14 C2: HL n= 6 Patients followed to determine safety, tolerability, and efficacy SMC Recommends Expansion 1. ASCO 2026
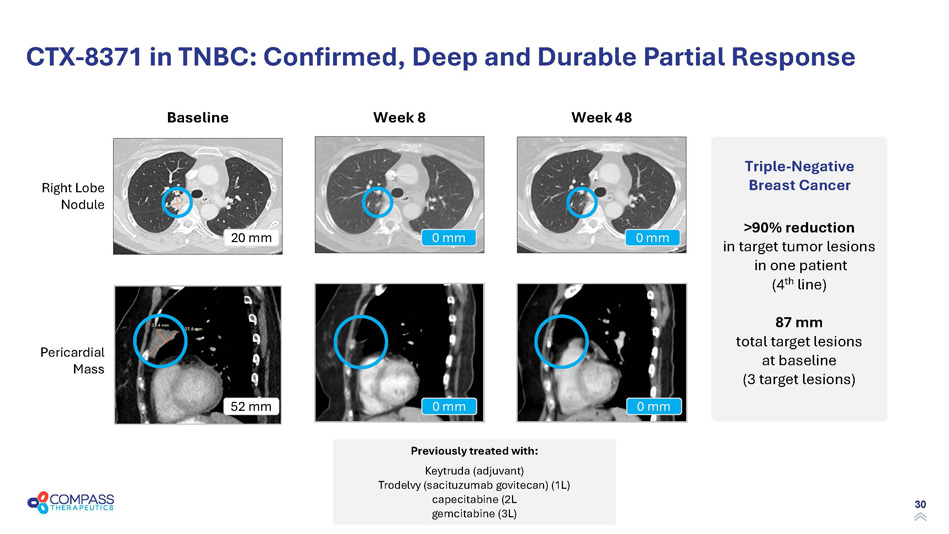
30 CTX - 8371 in TNBC: Confirmed, Deep and Durable Partial Response Right Lobe Nodule Pericardial Mass >90% reduction in target tumor lesions in one patient (4 th line) 87 mm total target lesions at baseline (3 target lesions) Triple - Negative Breast Cancer Baseline 20 mm 52 mm Week 8 0 mm 0 mm Week 48 0 mm 0 mm Previously treated with: Keytruda (adjuvant) Trodelvy ( sacituzumab govitecan ) (1L) capecitabine (2L gemcitabine (3L)
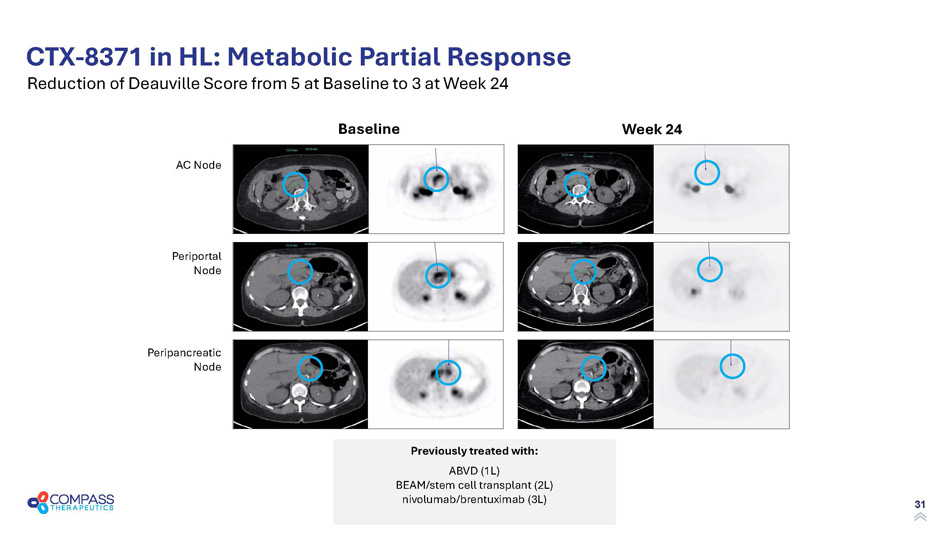
31 CTX - 8371 in HL: Metabolic Partial Response Reduction of Deauville Score from 5 at Baseline to 3 at Week 24 Periportal Node AC Node Peripancreatic Node Baseline Week 24 Previously treated with: ABVD (1L) BEAM/stem cell transplant (2L) nivolumab/brentuximab (3L)
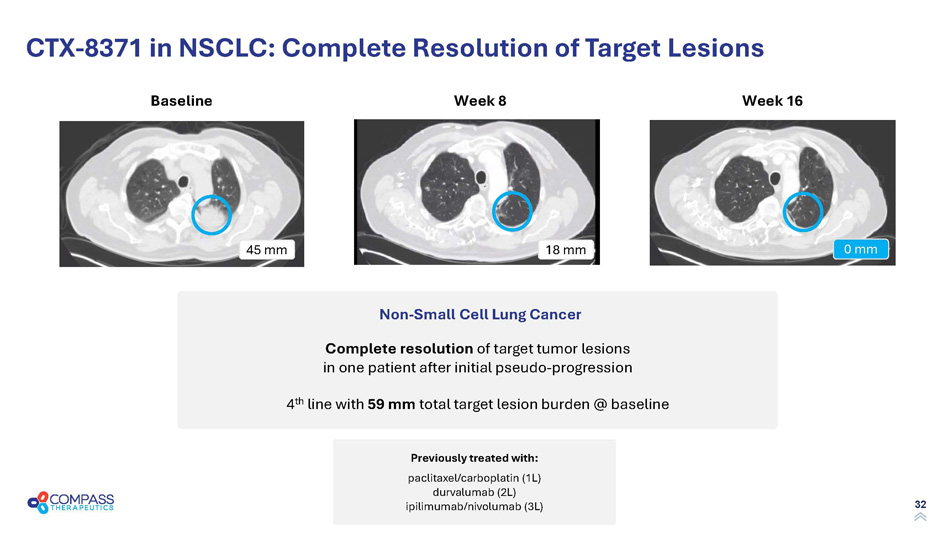
32 CTX - 8371 in NSCLC: Complete Resolution of Target Lesions Non - Small Cell Lung Cancer Complete resolution of target tumor lesions in one patient after initial pseudo - progression 4 th line with 59 mm total target lesion burden @ baseline Previously treated with: Baseline Week 8 Week 16 45 mm 18 mm Previously treated with: paclitaxel/carboplatin (1L) durvalumab (2L) ipilimumab/nivolumab (3L) 0 mm

33 Nasdaq: CMPX CTX - 10726 PD - 1 x VEGF - A bispecific antibody
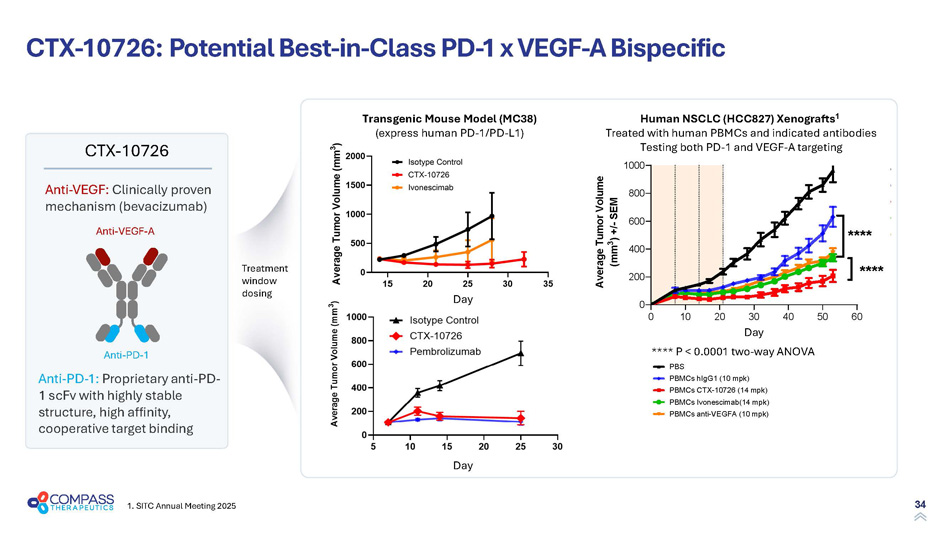
34 1. SITC Annual Meeting 2025 CTX - 10726 : Potential Best - in - Class PD - 1 x VEGF - A Bispecific Transgenic Mouse Model (MC38) (express human PD - 1/PD - L1) Human NSCLC (HCC827) Xenografts 1 Treated with human PBMCs and indicated antibodies Testing both PD - 1 and VEGF - A targeting Treatment window dosing **** P < 0.0001 two - way ANOVA Anti - PD - 1 Anti - VEGF - A Anti - PD - 1: Proprietary anti - PD - 1 scFv with highly stable structure , h igh affinity, cooperative target binding Anti - VEGF: Clinically proven mechanism (bevacizumab) CTX - 10726 Day Day Day
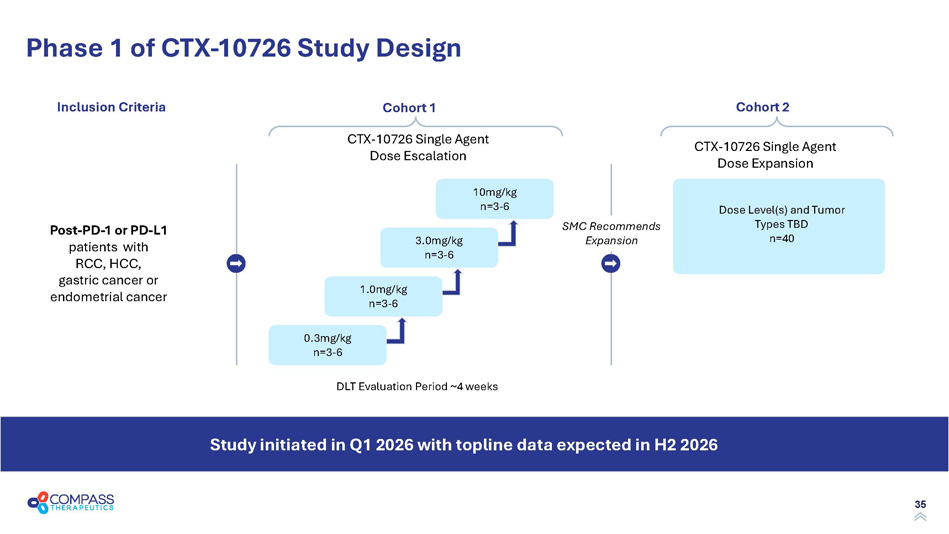
35 Phase 1 of CTX - 10726 Study Design CTX - 10726 Single Agent Dose Escalation CTX - 10726 Single Agent Dose Expansion Dose Level(s) and Tumor Types TBD n=40 Study initiated in Q1 2026 with topline data expected in H2 2026 Inclusion Criteria Cohort 1 Cohort 2 DLT Evaluation Period ~4 weeks 0.3mg/kg n=3 - 6 1.0mg/kg n=3 - 6 3.0mg/kg n=3 - 6 10mg/kg n=3 - 6 SMC Recommends Expansion Post - PD - 1 or PD - L1 patients with RCC, HCC, gastric cancer or endometrial cancer
36 Nasdaq: CMPX CTX - 471 CD137 agonist
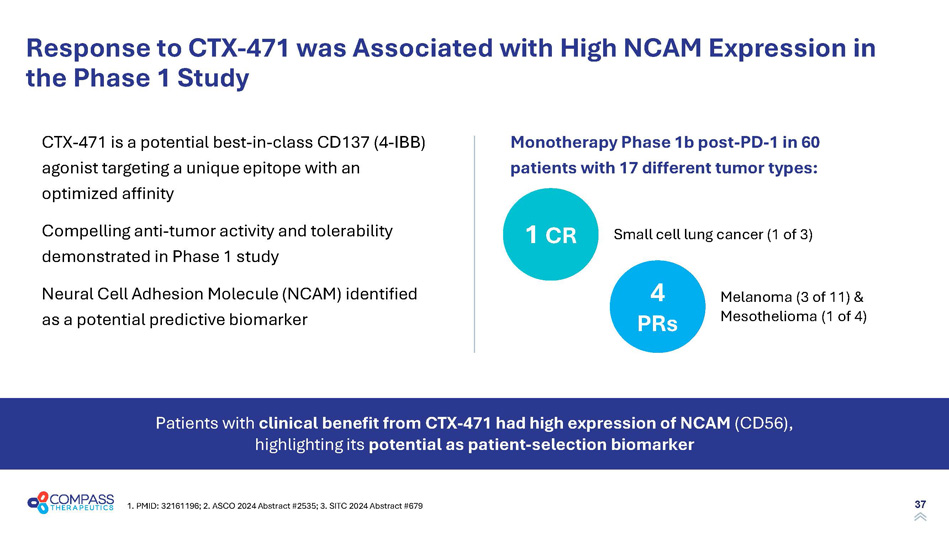
37 Response to CTX - 471 was Associated with High NCAM Expression in the Phase 1 Study 4 PRs M elanoma (3 of 11) & Mesothelioma (1 of 4) 1 CR S mall cell lung cancer (1 of 3) Patients with clinical benefit from CTX - 471 had high expression of NCAM (CD56), highlighting its potential as patient - selection biomarker CTX - 471 is a potential best - in - class CD137 (4 - IBB) agonist targeting a unique epitope with an optimized affinity Compelling anti - tumor activity and tolerability demonstrated in Phase 1 study Neural Cell Adhesion Molecule (NCAM) identified as a potential predictive biomarker Monotherapy Phase 1b post - PD - 1 in 60 patients with 17 different tumor types: 1. PMID: 32161196; 2. ASCO 2024 Abstract #2535; 3. SITC 2024 Abstract #679
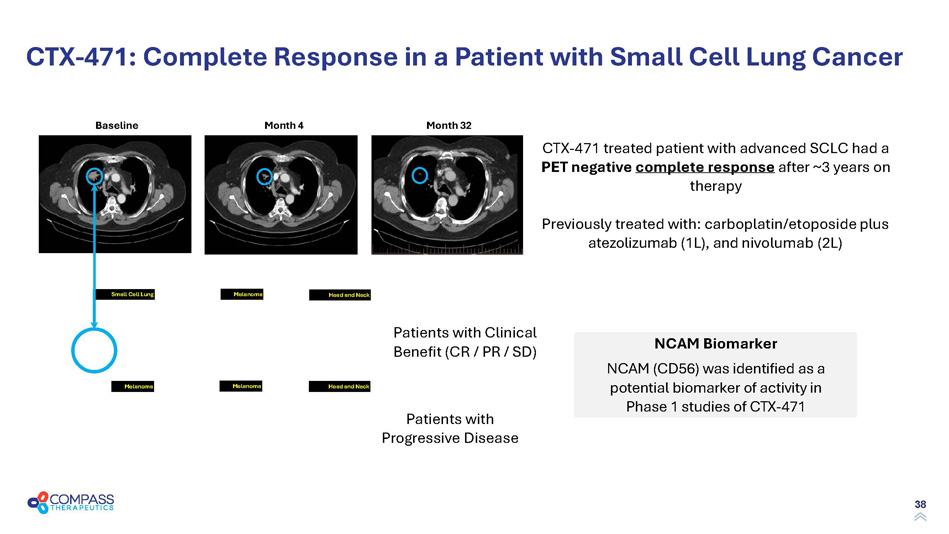
38 Small Cell Lung Melanoma Melanoma Melanoma Head and Neck Head and Neck CTX - 471: Complete Response in a Patient with Small Cell Lung Cancer CTX - 471 treated patient with advanced SCLC had a PET negative complete response after ~3 years on therapy Previously treated with: carboplatin/etoposide plus atezolizumab (1L), and nivolumab (2L) Small Cell Lung Patients with Clinical Benefit (CR / PR / SD) Patients with Progressive Disease Month 4 Month 32 Baseline NCAM Biomarker NCAM (CD56) was identified as a potential biomarker of activity in Phase 1 studies of CTX - 471
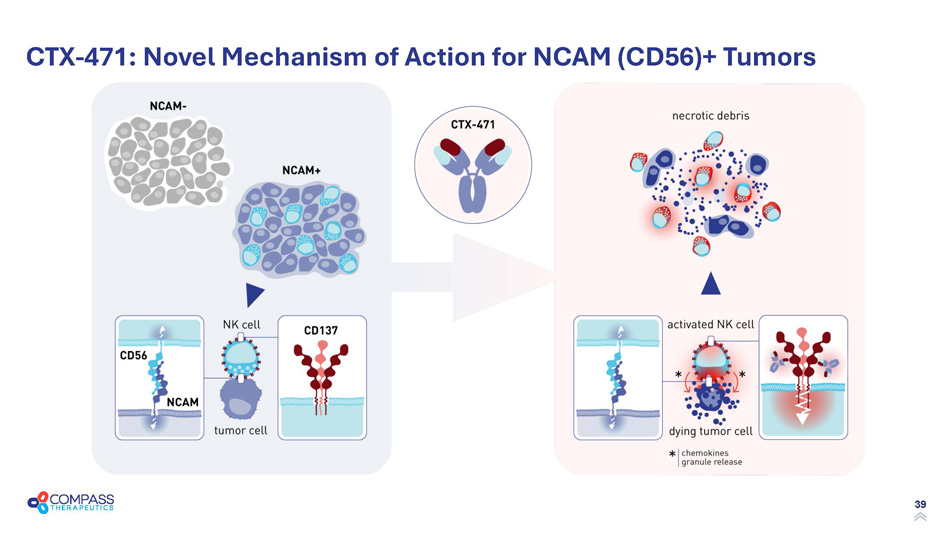
39 CTX - 471: Novel Mechanism of Action for NCAM (CD56)+ Tumors
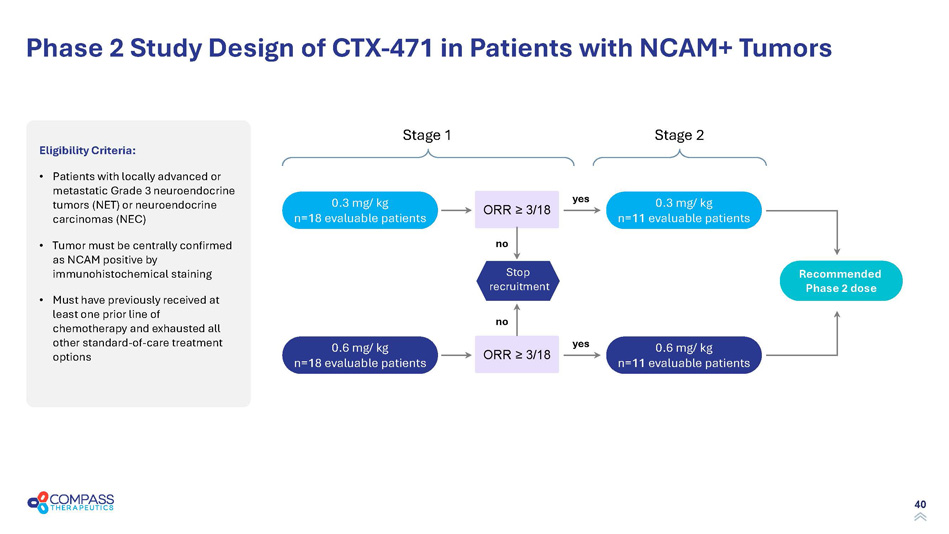
40 Phase 2 Study Design of CTX - 471 in Patients with NCAM+ Tumors Eligibility Criteria: • Patients with locally advanced or metastatic Grade 3 neuroendocrine tumors (NET) or neuroendocrine carcinomas (NEC) • Tumor must be centrally confirmed as NCAM positive by immunohistochemical staining • Must have previously received at least one prior line of chemotherapy and exhausted all other standard - of - care treatment options 0.3 mg/ kg n=18 evaluable patients Stop recruitment no Stage 1 ORR ≥ 3/18 0.6 mg/ kg n=18 evaluable patients ORR ≥ 3/18 Stage 2 0.3 mg/ kg n=11 evaluable patients 0.6 mg/ kg n=11 evaluable patients Recommended Phase 2 dose no yes yes
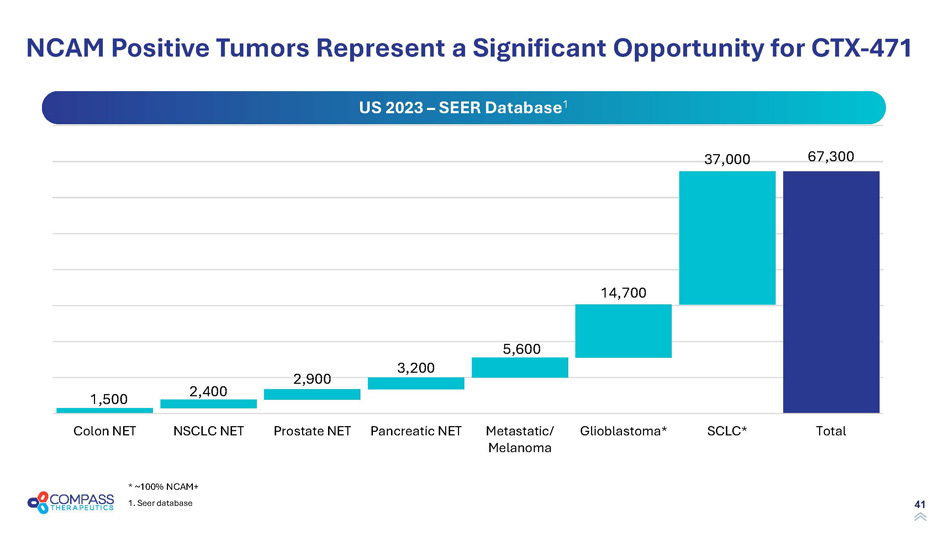
41 NCAM Positive Tumors Represent a Significant Opportunity for CTX - 471 1,500 2,400 2,900 3,200 5,600 14,700 37,000 67,300 Colon NET NSCLC NET Prostate NET Pancreatic NET Metastatic/ Melanoma Glioblastoma* SCLC* Total US 2023 – SEER Database 1 * ~100% NCAM+ 1. Seer database
42 Nasdaq: CMPX Milestones
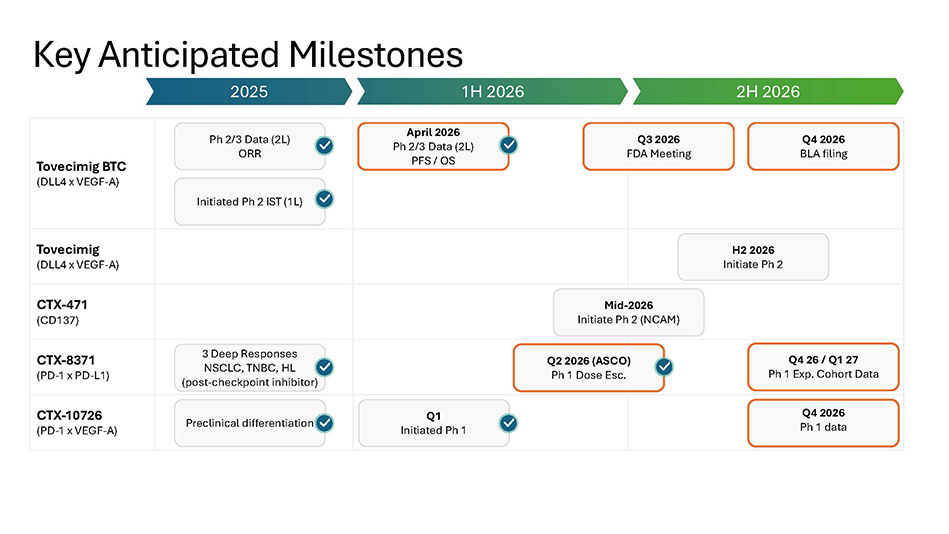
43 Key Anticipated Milestones Tovecimig BTC (DLL4 x VEGF - A) Tovecimig (DLL4 x VEGF - A) CTX - 471 (CD137) CTX - 8371 (PD - 1 x PD - L1) CTX - 10726 (PD - 1 x VEGF - A) 2025 1H 2026 2H 2026 Ph 2/3 Data (2L) ORR Initiated Ph 2 IST (1L) 3 Deep Responses NSCLC, TNBC, HL (post - checkpoint inhibitor) Preclinical differentiation April 2026 Ph 2/3 Data (2L) PFS / OS Q4 2026 BLA filing H2 2026 Initiate Ph 2 Mid - 2026 Initiate Ph 2 (NCAM) Q2 2026 (ASCO) Ph 1 Dose Esc. Q4 26 / Q1 27 Ph 1 Exp. Cohort Data Q4 2026 Ph 1 data Q1 Initiated Ph 1 Q3 2026 FDA Meeting

44 Thomas J. Schuetz, MD, PhD President, CEO, & Vice Chairman of the Board Barry Shin , J D, MBA Chief Financial Officer Arjun Prasad, MBA, MPH Chief Commercial Officer Cynthia Sirard, MD Chief Medical Officer Bing Gong, PhD Chief Scientific Officer Jon Anderman, JD General Counsel & Corporate Secretary Neil Lerner, CPA, MIM Chief Accounting Officer Leadership Team Experienced in Drug Discovery , Development, and Commercialization
45 Nasdaq: CMPX Compass Therapeutics Website: compasstherapeutics.com Nasdaq: CMPX