Exhibit 99.1
CORPORATE PRESENTATION June 2026 Advancing the Next Generation of Immuno - oncology NASDAQ/TASE : PPBT
2 Forward - looking Statements and Safe Harbor Certain statements in this presentation that are forward - looking and not statements of historical fact are forward - looking statements within the meaning of the safe harbor provisions of the Private Securities Litigation Reform Act of 1995 . Such forward - looking statements include, but are not limited to, statements that are not statements of historical fact, and may be identified by words such as believe , expect , intend , plan , may , should , could , might , seek , target , will , project , forecast , continue or anticipate or their negatives or variations of these words or other comparable words or by the fact that these statements do not relate strictly to historical matters . You should not place undue reliance on these forward - looking statements, which are not guarantees of future performance . Forward - looking statements reflect our current views, expectations, beliefs or intentions with respect to future events, and are subject to a number of assumptions, involve known and unknown risks, many of which are beyond our control, as well as uncertainties and other factors that may cause our actual results, performance or achievements to be significantly different from any future results, performance or achievements expressed or implied by the forward - looking statements . Important factors that could cause or contribute to such differences include, among others, risks relating to : the plans, strategies and objectives of management for future operations ; product development for NT 219 , CM 24 and IM 1240 ; the process by which such early stage therapeutic candidates could potentially lead to an approved drug product is long and subject to highly significant risks, particularly with respect to a joint development collaboration ; the fact that drug development and commercialization involves a lengthy and expensive process with uncertain outcomes ; our ability to successfully develop and commercialize our pharmaceutical products ; the expense, length, progress and results of any clinical trials ; the impact of any changes in regulation and legislation that could affect the pharmaceutical industry ; the difficulty in receiving the regulatory approvals necessary in order to commercialize our products ; the difficulty of predicting actions of the U . S . Food and Drug Administration or any other applicable regulator of pharmaceutical products ; the regulatory environment and changes in the health policies and regimes in the countries in which we operate ; the uncertainty surrounding the actual market reception to our pharmaceutical products once cleared for marketing in a particular market ; the introduction of competing products ; patents obtained by competitors ; dependence on the effectiveness of our patents and other protections for innovative products ; our ability to obtain, maintain and defend issued patents ; the commencement of any patent interference or infringement action against our patents, and our ability to prevail, obtain a favorable decision or recover damages in any such action ; and the exposure to litigation, including patent litigation, and/or regulatory actions ; the impact of the economic, public health, political and security situation in Israel, the U . S . and other countries in which we may operate or obtain approvals for our products or our business, and other factors that are discussed in our Annual Report on Form 20 - F for the year ended December 31 , 2025 and in our other filings with the U . S . Securities and Exchange Commission ( SEC ), including our cautionary discussion of risks and uncertainties under Risk Factors in our Registration Statements and Annual Reports . These are factors that we believe could cause our actual results to differ materially from expected results . Other factors besides those we have listed could also adversely affect us . Any forward - looking statement in this press release speaks only as of the date which it is made . We disclaim any intention or obligation to publicly update or revise any forward - looking statement or other information contained herein, whether as a result of new information, future events or otherwise, except as required by applicable law . You are advised, however, to consult any additional disclosures we make in our reports to the SEC, which are available on the SEC ’ s website, https : //www . sec . gov . The trademarks, tradenames, service marks and logos included herein are the property of the owners thereof and are used for reference purposes only . Such use should not be construed as an endorsement of the products or services of the Company

| 3 2 Lead program expected to enter the clinic in 2027 IM1240 (cappedCD3x 5T4 xNKG2A), a first - in - class CAPTN - 3 tri - specific antibody Second program, IM1305 (cappedCD3x TROP2 xNKG2A) 1 CAPTN - 3: differentiated tri - specific platform activating both innate and adaptive immune systems The only platform engaging both T cells AND NK cells while incorporating a masking technology 5 Solid tumors remain largely untreated by T cell engagers A large unmet need with no approved tri - specific option 4 Focused on key inflection point and significant market potential to create value Comparable masked TCE programs secured >$1B deals at preclinical stage. Key catalyst - results from P1 study starting from 1H 2028 FINANCIALS Cash $ 6.4 M Runway INTO H1 2027 Exchange NASDAQ + TASE PPBT As of March 31, 2026 Snapshot: Company Highlights 3 Safety and efficacy demonstrated in IND enabling Studies Strong anti - tumor activity and 300 п improved safety profile versus the non - masked comparator
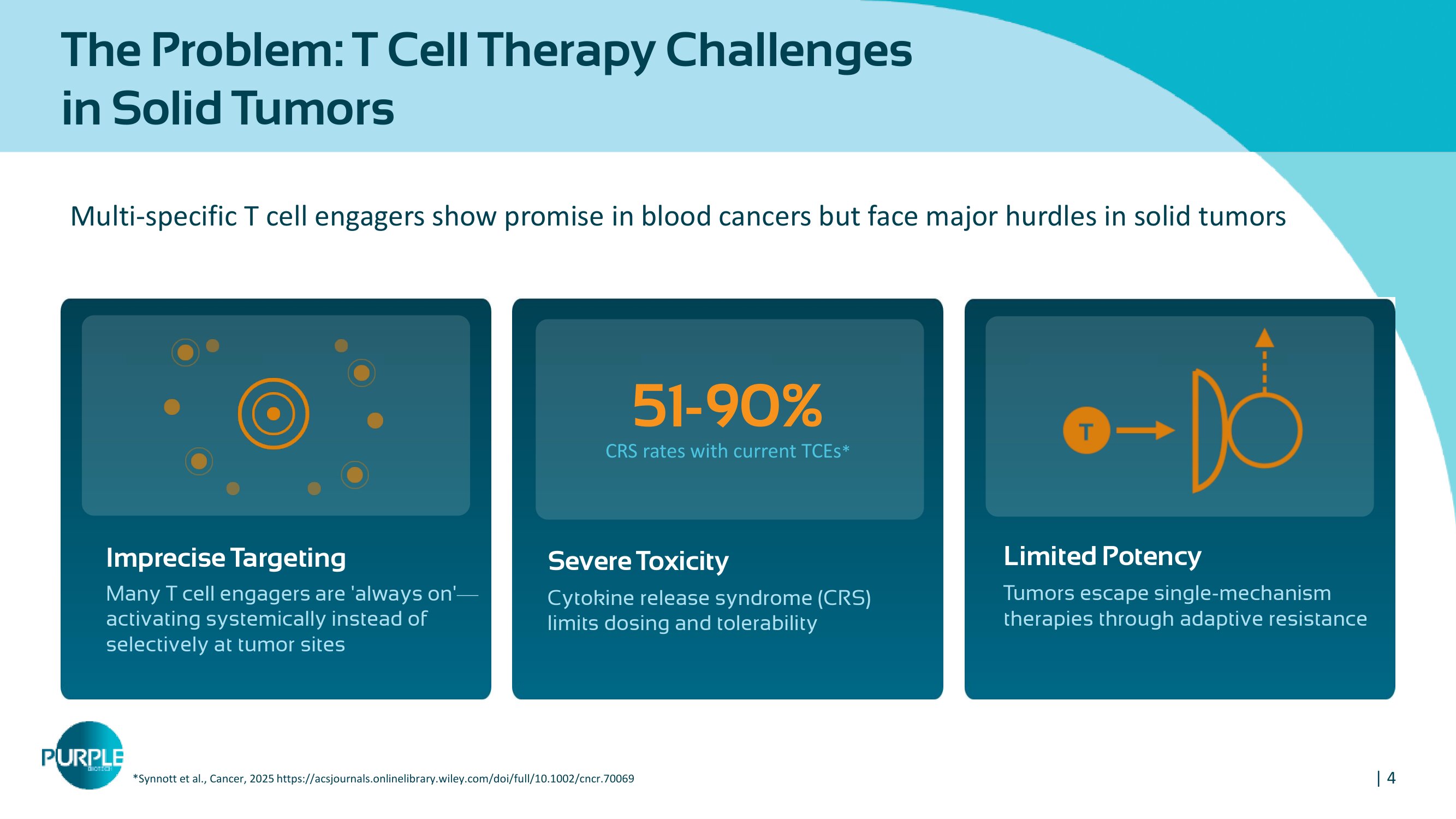
| 4 Multi - specific T cell engagers show promise in blood cancers but face major hurdles in solid tumors Imprecise Targeting Many T cell engagers are 'always on' — activating systemically instead of selectively at tumor sites Severe Toxicity Cytokine release syndrome (CRS) limits dosing and tolerability 51 - 90 % CRS rates with current TCEs * Limited Potency Tumors escape single - mechanism therapies through adaptive resistance The Problem: T Cell Therapy Challenges in Solid Tumors *Synnott et al., Cancer, 2025 https://acsjournals.onlinelibrary.wiley.com/doi/full/10.1002/cncr.70069
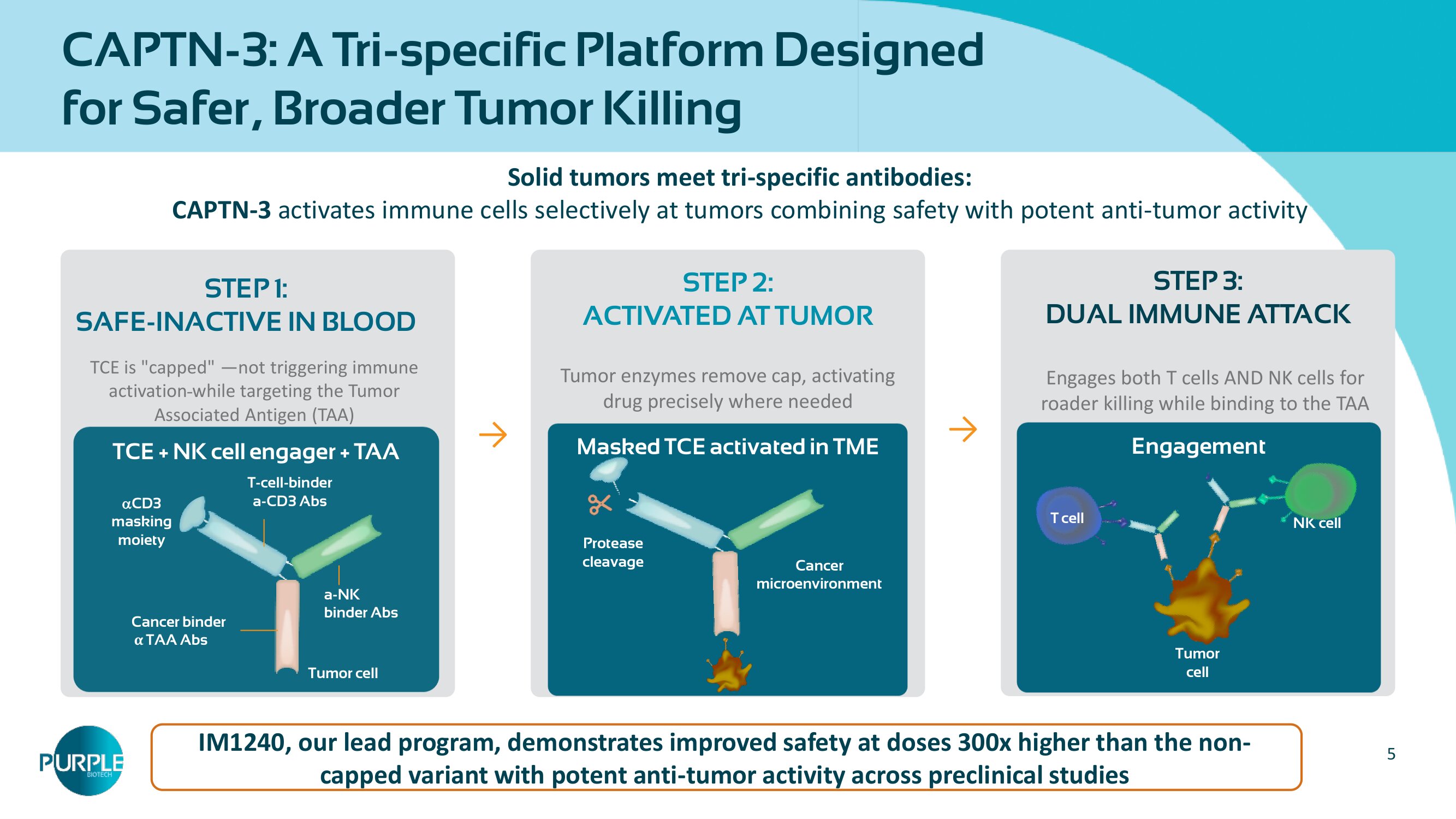
5 Solid tumors meet tri - specific antibodies: CAPTN - ϯ activates immune cells selectively at tumors combining safety with potent anti - tumor activity STEP 1: SAFE - INACTIVE IN BLOOD → STEP 2 : ACTIVATED AT TUMOR Tumor enzymes remove cap, activating drug precisely where needed → STEP 3: DUAL IMMUNE ATTACK Engages both T cells AND NK cells for roader killing while binding to the TAA IM 1240 , our lead program, demonstrates improved safety at doses 300 x higher than the non - capped variant with potent anti - tumor activity across preclinical studies TCE + NK cell engager + TAA Cancer binder α TAA Abs a - NK binder Abs T - cell - binder a - CD 3 Abs CD3 masking moiety Masked TCE activated in TME Cancer microenvironment Protease cleavage Engagement Tumor cell NK cell T cell CAPTN - 3: A Tri - specific Platform Designed for Safer, Broader Tumor Killing Tumor cell TCE is "capped" — not triggering immune activation while targeting the Tumor Associated Antigen (TAA)
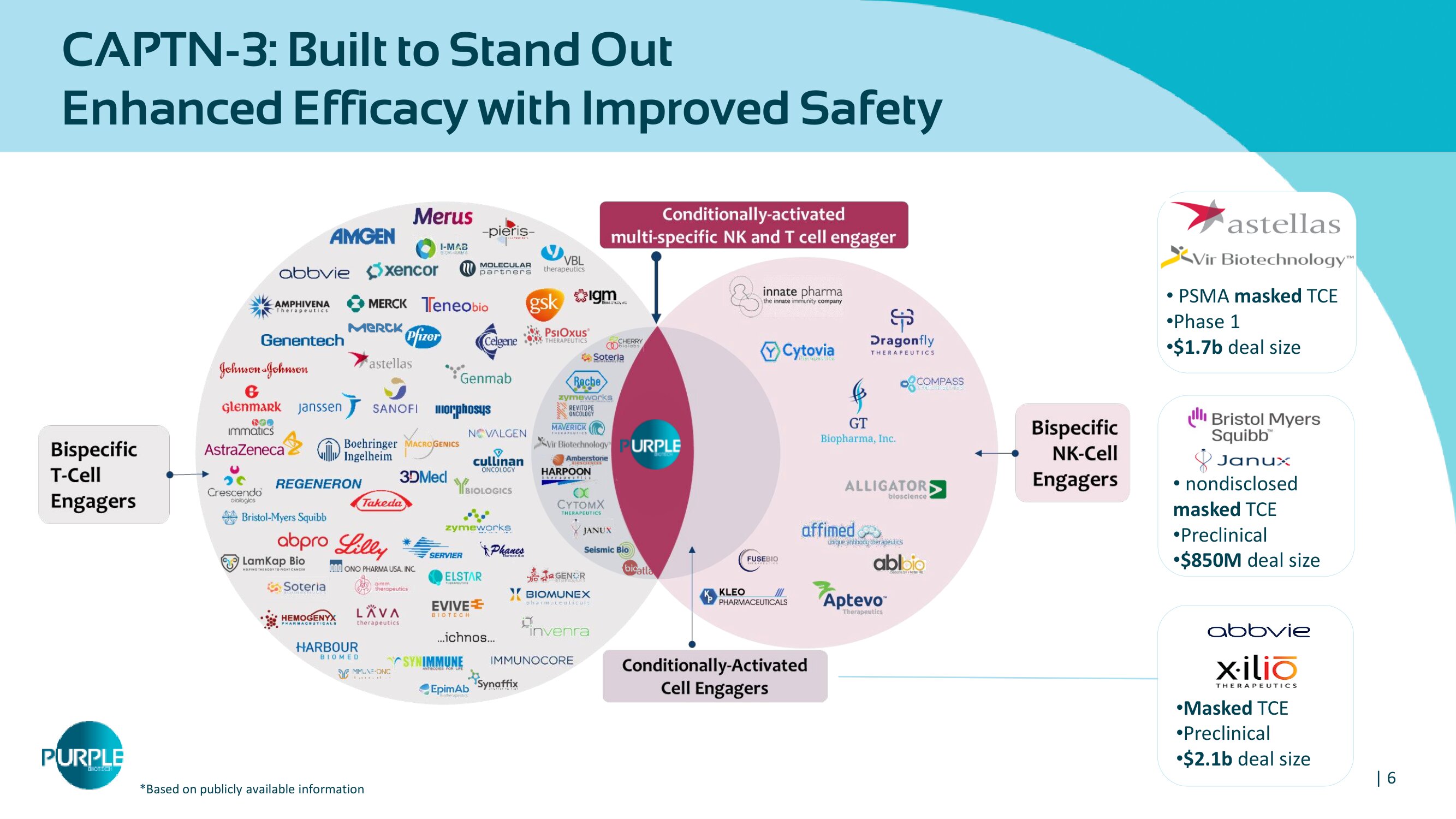
| 6 CAPTN - 3 : Built to Stand Out – Enhanced Efficacy with Improved Safety * B ased on publicly available information • Masked TCE • Preclinical • $ 2.1 b deal size 2026 • nondisclosed masked TCE • Preclinical • $ 850 M deal size • PSMA masked TCE • Phase 1 • $1.7b deal size
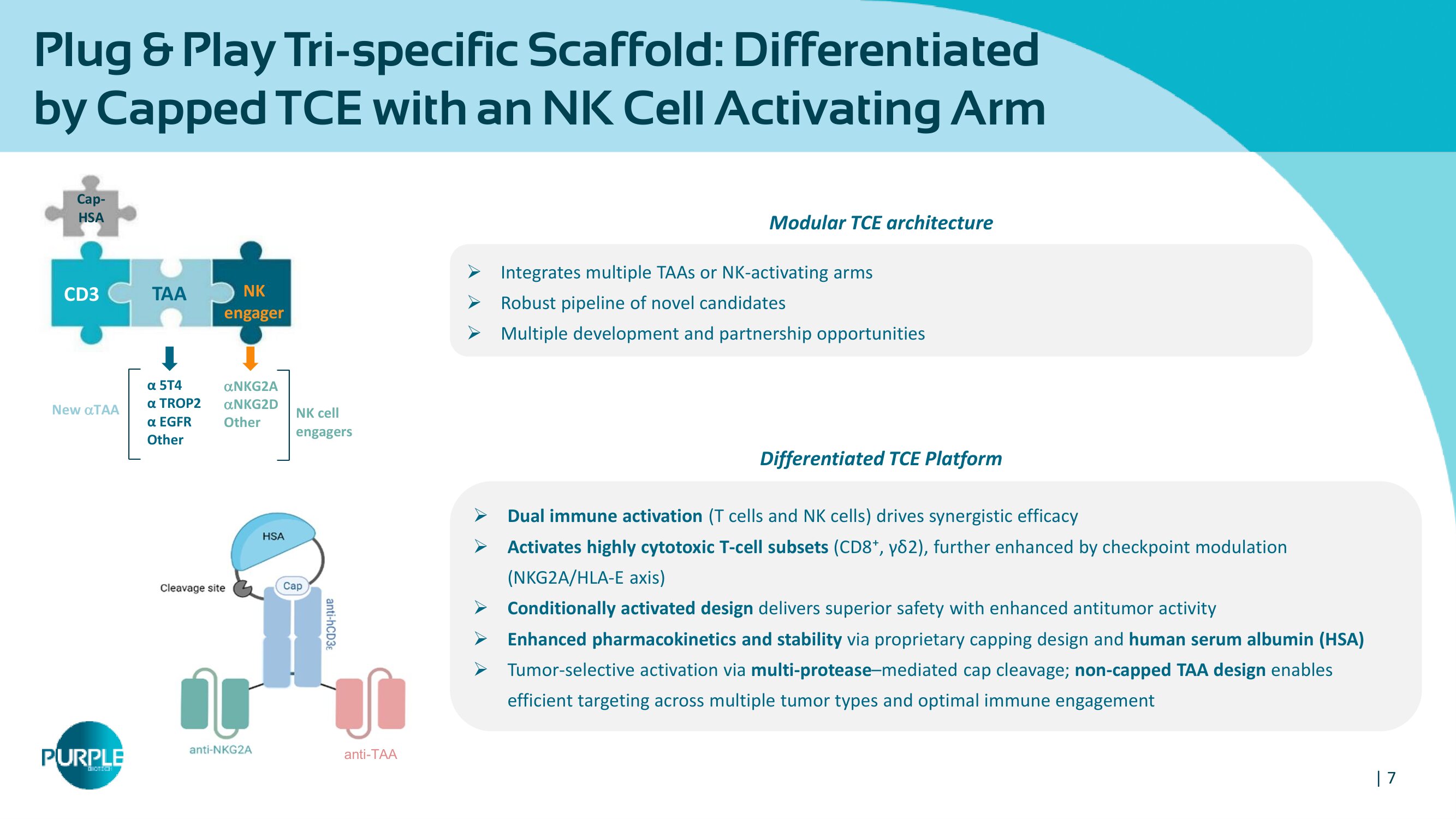
| 7 anti - TAA Plug & Play Tri - specific Scaffold: Differentiated by Capped TCE with an NK Cell Activating Arm 7 » Integrates multiple TAAs or NK - activating arms » Robust pipeline of novel candidates » Multiple development and partnership opportunities NKG 2 A NKG 2 D Other NK cell engagers NK engager Cap - HSA CD 3 TAA α 5 T 4 α TROP 2 α EGFR Other New TAA » Dual immune activation ( T cells and NK cells ) drives synergistic efficacy » Activates highly cytotoxic T - cell subsets (CD 8 ⁺ , γδ 2 ), further enhanced by checkpoint modulation (NKG 2 A/HLA - E axis) » Conditionally activated design delivers superior safety with enhanced antitumor activity » Enhanced pharmacokinetics and stability via proprietary capping design and human serum albumin (HSA) » Tumor - selective activation via multi - protease – mediated cap cleavage ; non - capped TAA design enables efficient targeting across multiple tumor types and optimal immune engagement Differentiated TCE Platform Modular TCE architecture
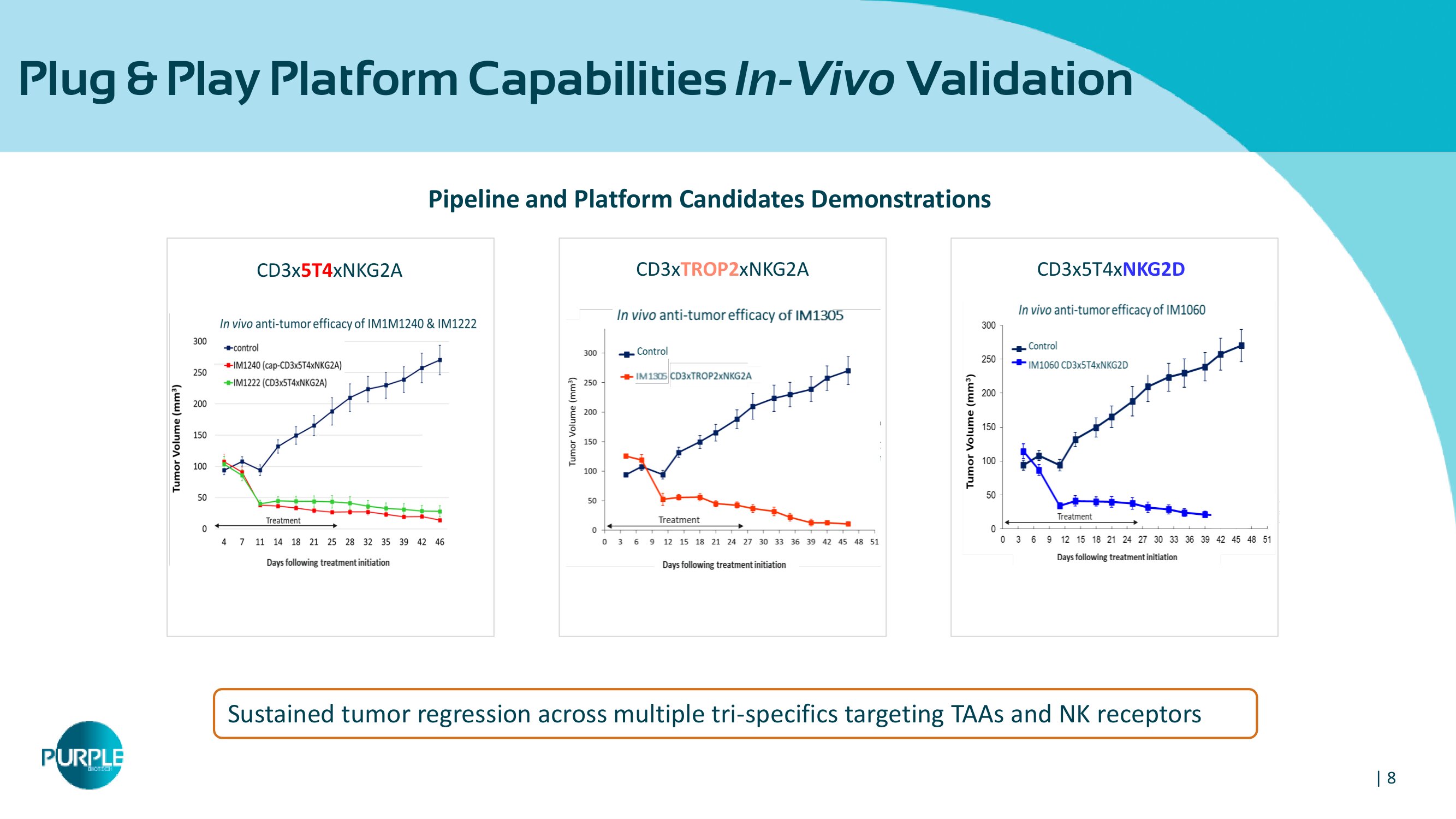
| 8 Plug & Play Platform Capabilities In - Vivo Validation 8 CD 3 x 5 T 4 x NKG 2 D Pipeline and Platform Candidates Demonstrations Sustained tumor regression across multiple tri - specifics targeting TAAs and NK receptors CD 3 x 5 T 4 xNKG 2 A CD 3 x TROP 2 xNKG 2 A
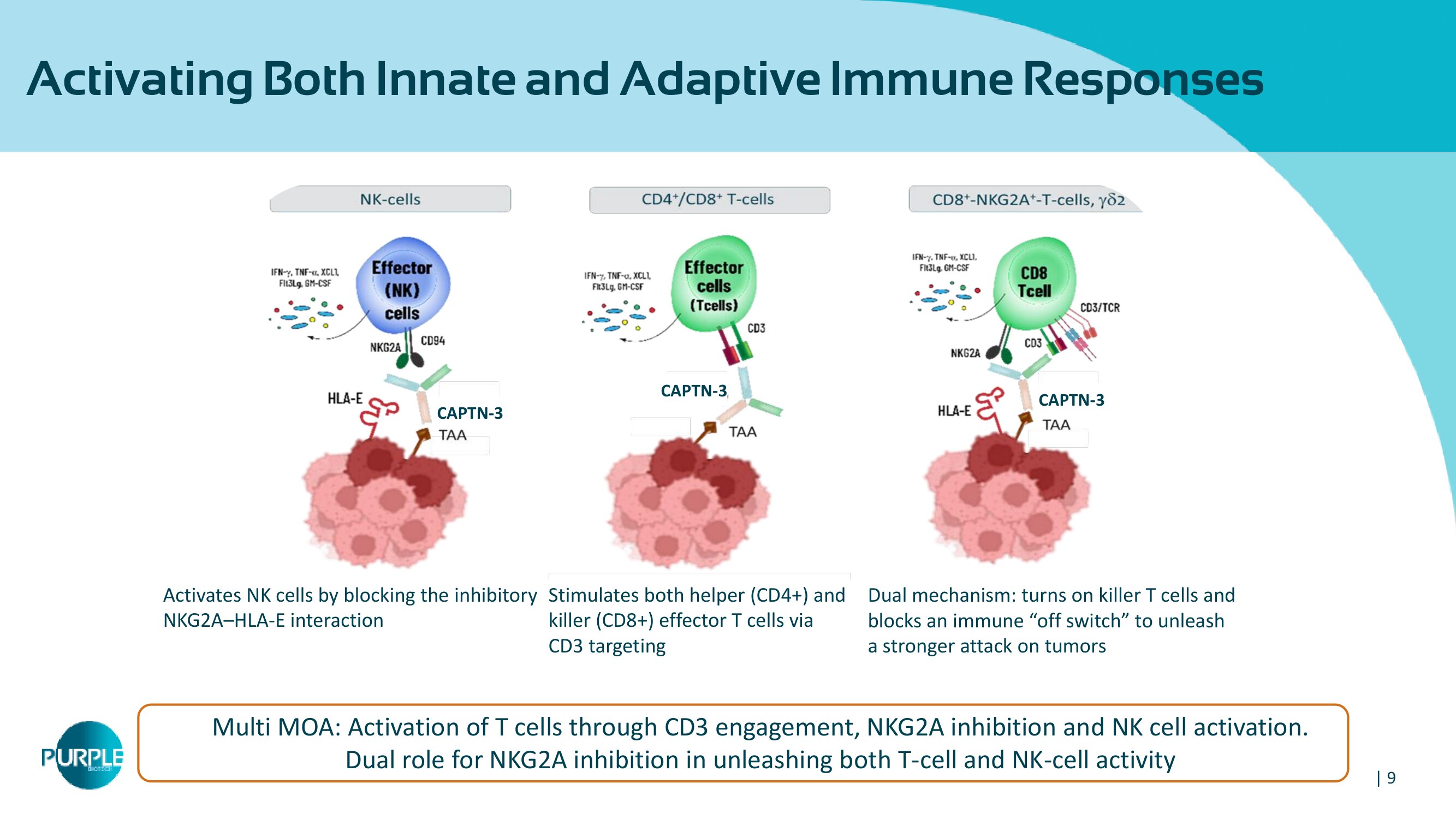
| 9 Activating Both Innate and Adaptive Immune Responses Multi MOA: Activation of T cells through CD3 engagement, NKG2A inhibition and NK cell activation. Dual role for NKG2A inhibition in unleashing both T - cell and NK - cell activity Stimulates both helper (CD 4 +) and killer (CD 8 +) effector T cells via CD 3 targeting Dual mechanism: turns on killer T cells and blocks an immune off switch to unleash a stronger attack on tumors Activates NK cells by blocking the inhibitory NKG 2 A – HLA - E interaction CAPTN - 3 CAPTN - 3 CAPTN - 3
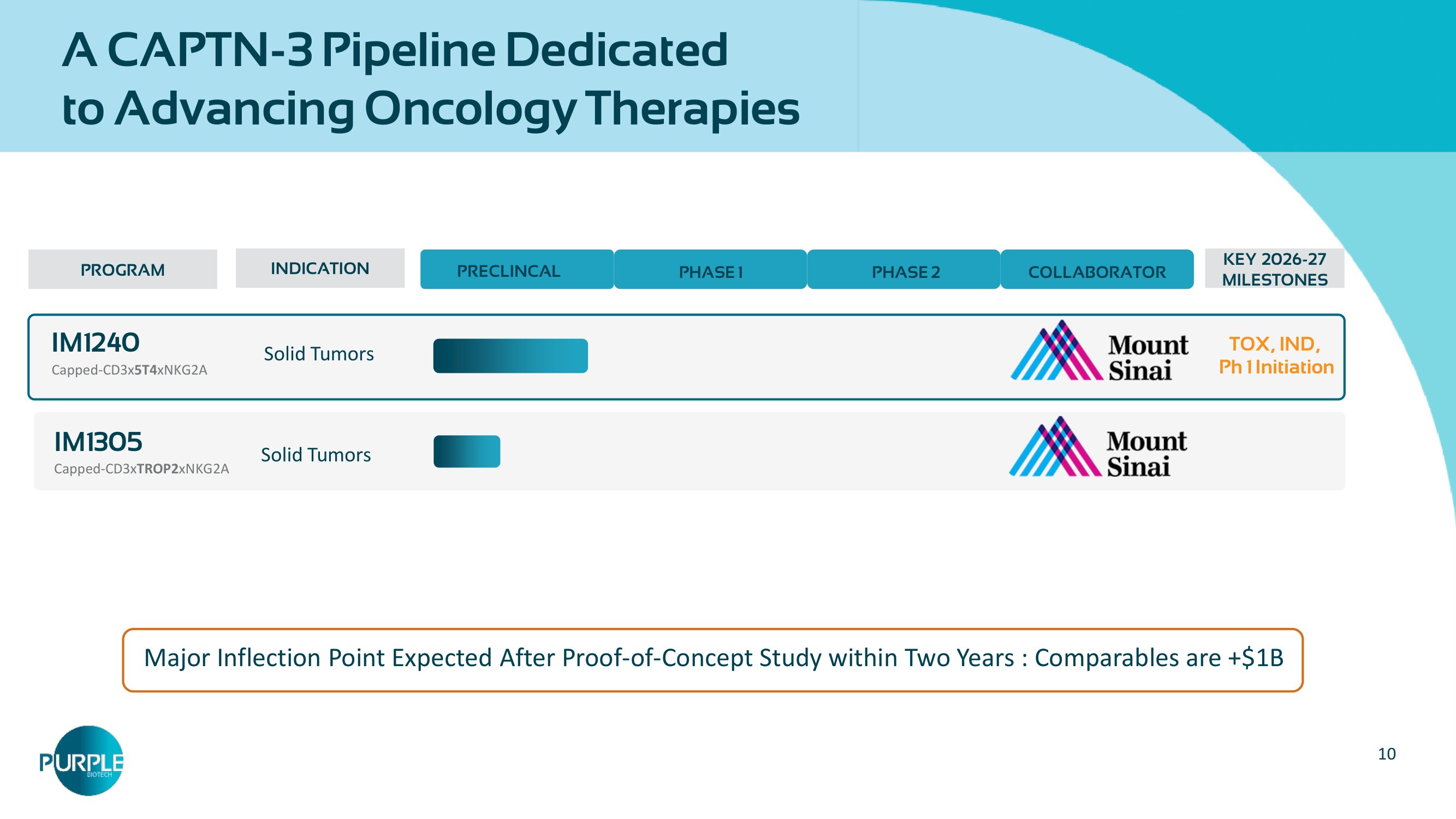
10 PROGRAM INDICATION PRECLINCAL PHASE 1 PHASE 2 COLLABORATOR KEY 2026 - 27 MILESTONES IM 1240 Capped - CD3x 5T4 xNKG2A Solid Tumors TOX, IND, Ph 1 Initiation IM 1305 Capped - CD 3 x TROP 2 xNKG 2 A Solid Tumors Major Inflection Point Expected After Proof - of - Concept Study within Two Years : Comparables are +$ 1 B A CAPTN - 3 Pipeline Dedicated to Advancing Oncology Therapies
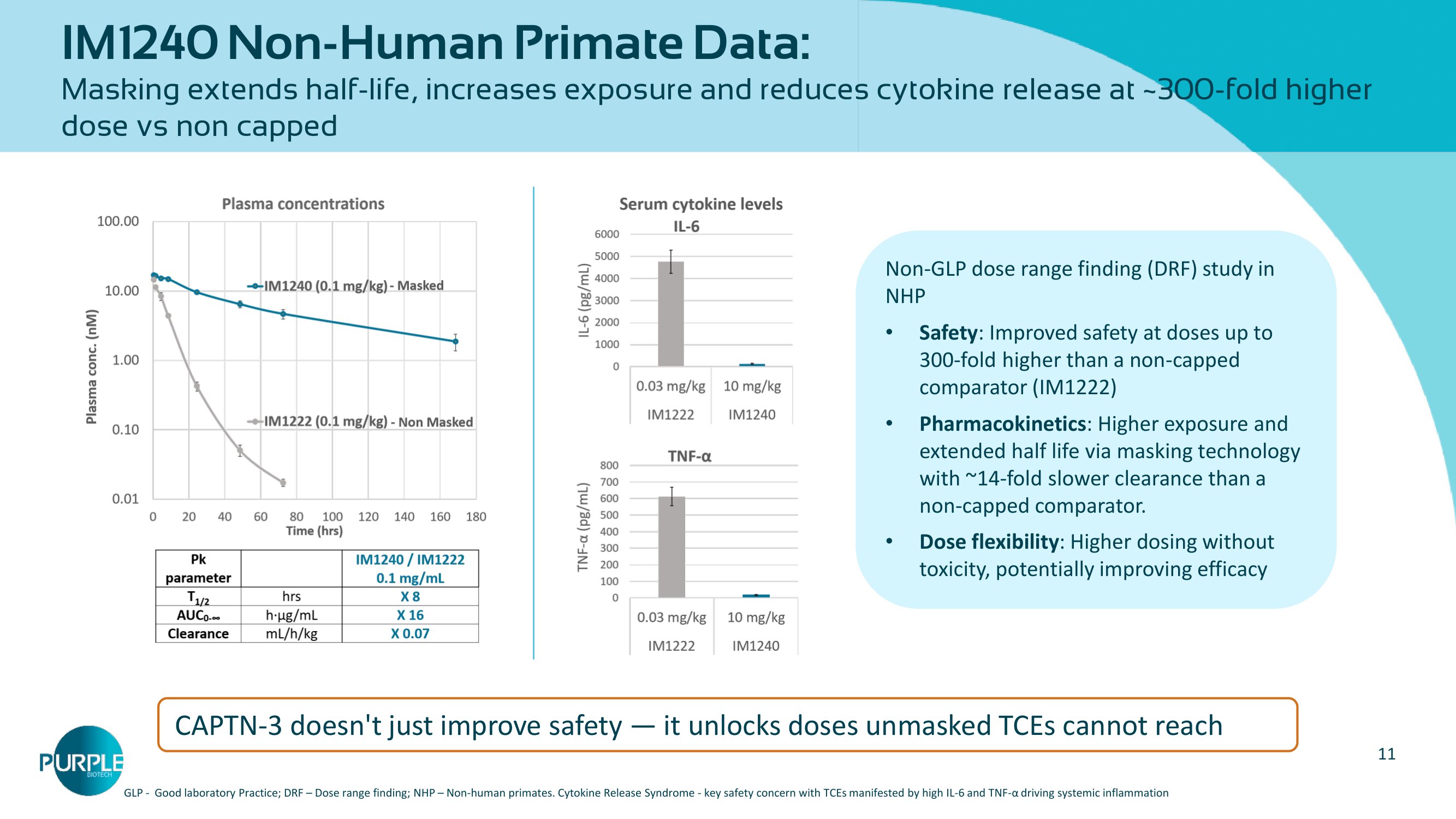
11 IM 1240 Non - Human Primate Data: Masking extends half - life, increases exposure and reduces cytokine release at ~ 300 - fold higher dose vs non capped Non - GLP dose range finding (DRF) study in NHP • Safety : Improved safety at doses up to 300 - fold higher than a non - capped comparator (IM 1222 ) • Pharmacokinetics : Higher exposure and extended half life via masking technology with ~ 14 - fold slower clearance than a non - capped comparator. • Dose flexibility : Higher dosing without toxicity, potentially improving efficacy CAPTN - 3 doesn't just improve safety — it unlocks doses unmasked TCEs cannot reach GLP - Good laboratory Practice; DRF – Dose range finding; NHP – Non - human primates. Cytokine Release Syndrome - key safety conc ern with TCEs manifested by high IL - 6 and TNF - α driving systemic inflammation
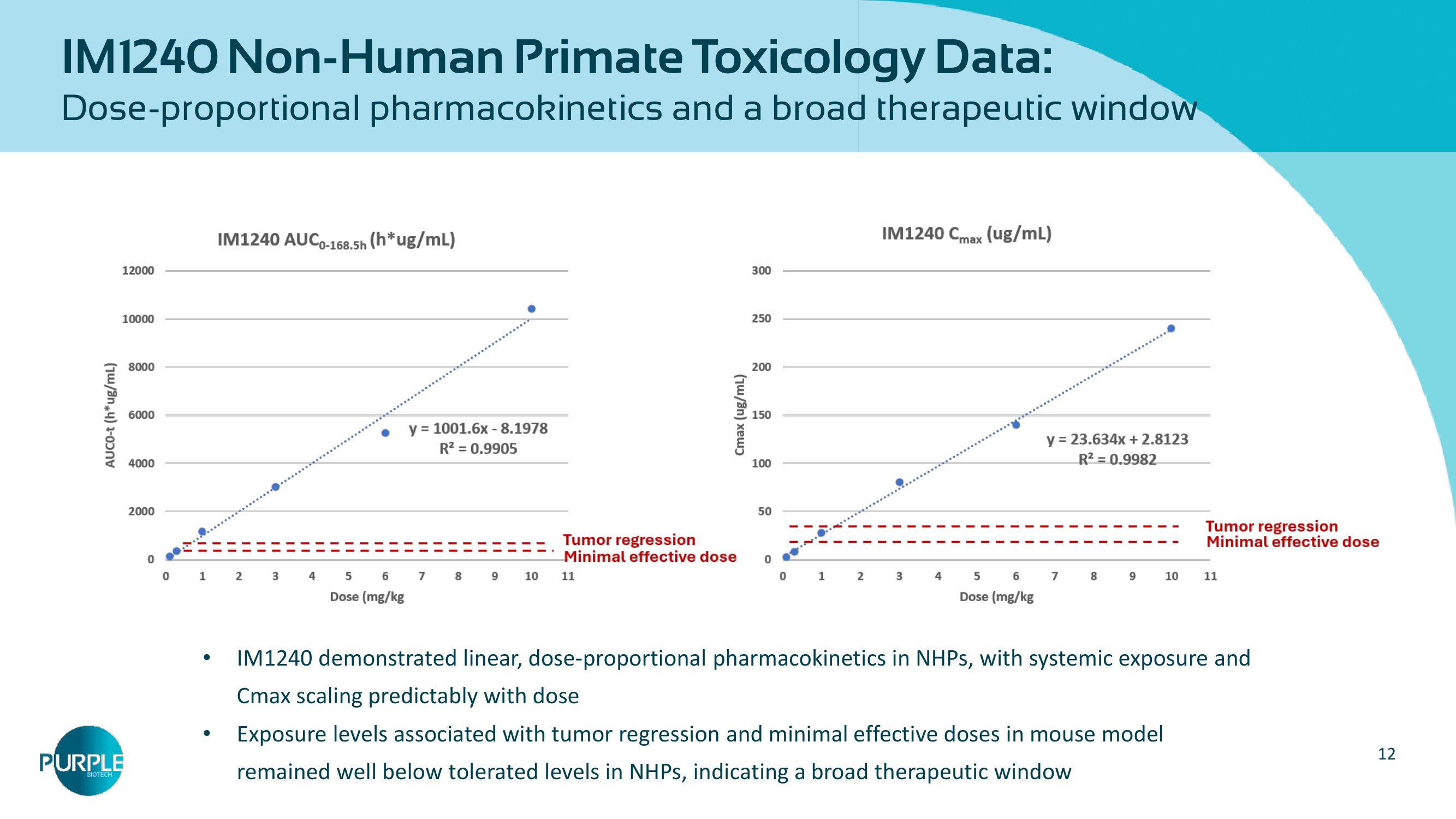
12 IM1240 Non - Human Primate Toxicology Data: Dose - proportional pharmacokinetics and a broad therapeutic window • IM 1240 demonstrated linear, dose - proportional pharmacokinetics in NHPs, with systemic exposure and Cmax scaling predictably with dose • Exposure levels associated with tumor regression and minimal effective doses in mouse model remained well below tolerated levels in NHPs, indicating a broad therapeutic window
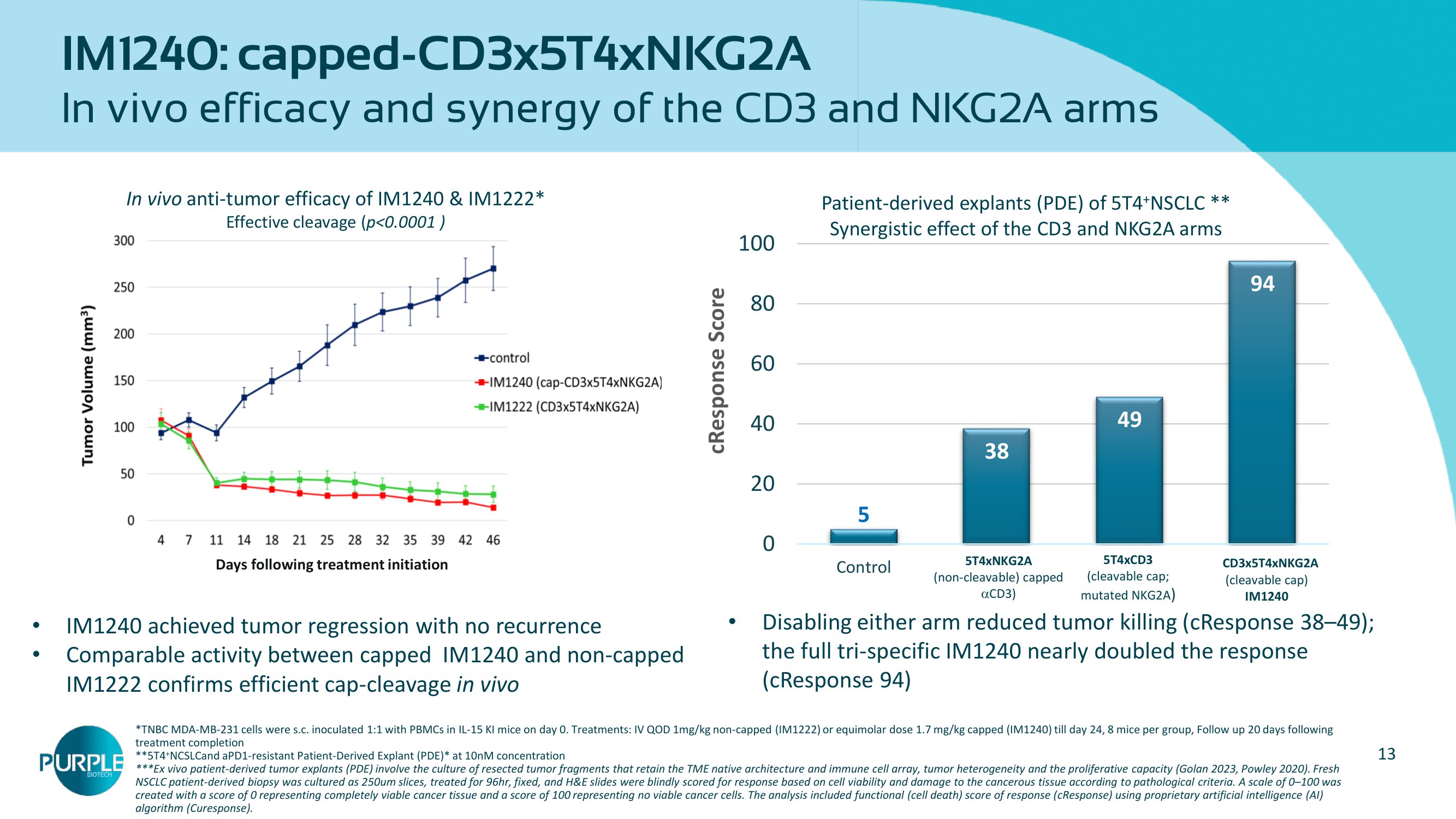
13 5 38 49 94 0 20 40 60 80 100 Control IM1242 IM1340 IM1240 cResponse Score CD3x5T4 x NKG2A (cleavable cap) IM1240 5 T 4 xNKG 2 A (non - cleavable) capped CD 3 ) 5 T 4 xCD 3 (cleavable cap; mutated NKG 2 A ) Patient - derived explants (PDE) of 5 T 4 + NSCLC ** Synergistic effect of the CD 3 and NKG 2 A arms *TNBC MDA - MB - 231 cells were s.c. inoculated 1:1 with PBMCs in IL - 15 KI mice on day 0. Treatments: IV QOD 1mg/kg non - capped (IM1222) or equimolar dose 1.7 mg/kg capped (IM1240) till day 24, 8 mice per gro up, Follow up 20 days following treatment completion **5T4 + NCSLCand aPD1 - resistant Patient - Derived Explant (PDE)* at 10nM concentration *** Ex vivo patient - derived tumor explants (PDE) involve the culture of resected tumor fragments that retain the TME native architec ture and immune cell array, tumor heterogeneity and the proliferative capacity (Golan 2023, Powley 2020). Fresh NSCLC patient - derived biopsy was cultured as 250um slices, treated for 96hr, fixed, and H&E slides were blindly scored for response based on cell viability and damage to the cancerous tissue according t o p athological criteria. A scale of 0 – 100 was created with a score of 0 representing completely viable cancer tissue and a score of 100 representing no viable cancer cells . T he analysis included functional (cell death) score of response ( cResponse ) using proprietary artificial intelligence (AI) algorithm ( Curesponse ). IM 1240 : capped - CD 3 x 5 T 4 xNKG 2 A In vivo efficacy and synergy of the CD 3 and NKG 2 A arms Days following treatment initiation In vivo anti - tumor efficacy of IM1240 & IM1222* Effective cleavage ( p<0.0001 ) • IM 1240 achieved tumor regression with no recurrence • Comparable activity between capped IM 1240 and non - capped IM 1222 confirms efficient cap - cleavage in vivo • Disabling either arm reduced tumor killing ( cResponse 38 – 49 ); the full tri - specific IM 1240 nearly doubled the response ( cResponse 94 )
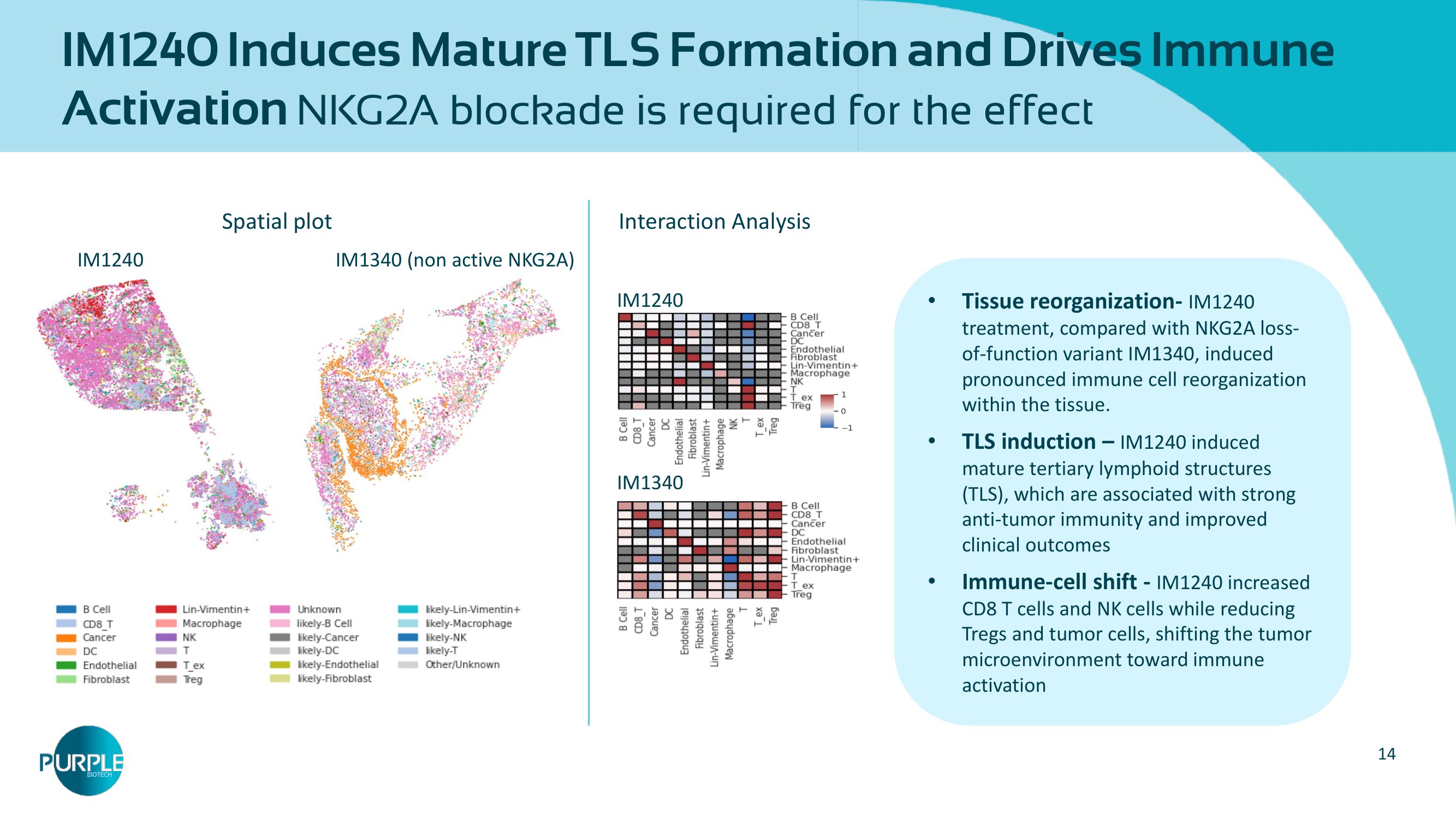
14 IM1240 Induces Mature TLS Formation and Drives Immune Activation NKG2A blockade is required for the effect IM 1240 IM 1340 (non active NKG 2 A) Spatial plot IM1240 IM 1340 Interaction Analysis • Tissue reorganization - IM 1240 treatment, compared with NKG 2 A loss - of - function variant IM 1340 , induced pronounced immune cell reorganization within the tissue. • TLS induction – IM 1240 induced mature tertiary lymphoid structures (TLS), which are associated with strong anti - tumor immunity and improved clinical outcomes • Immune - cell shift - IM 1240 increased CD 8 T cells and NK cells while reducing Tregs and tumor cells, shifting the tumor microenvironment toward immune activation
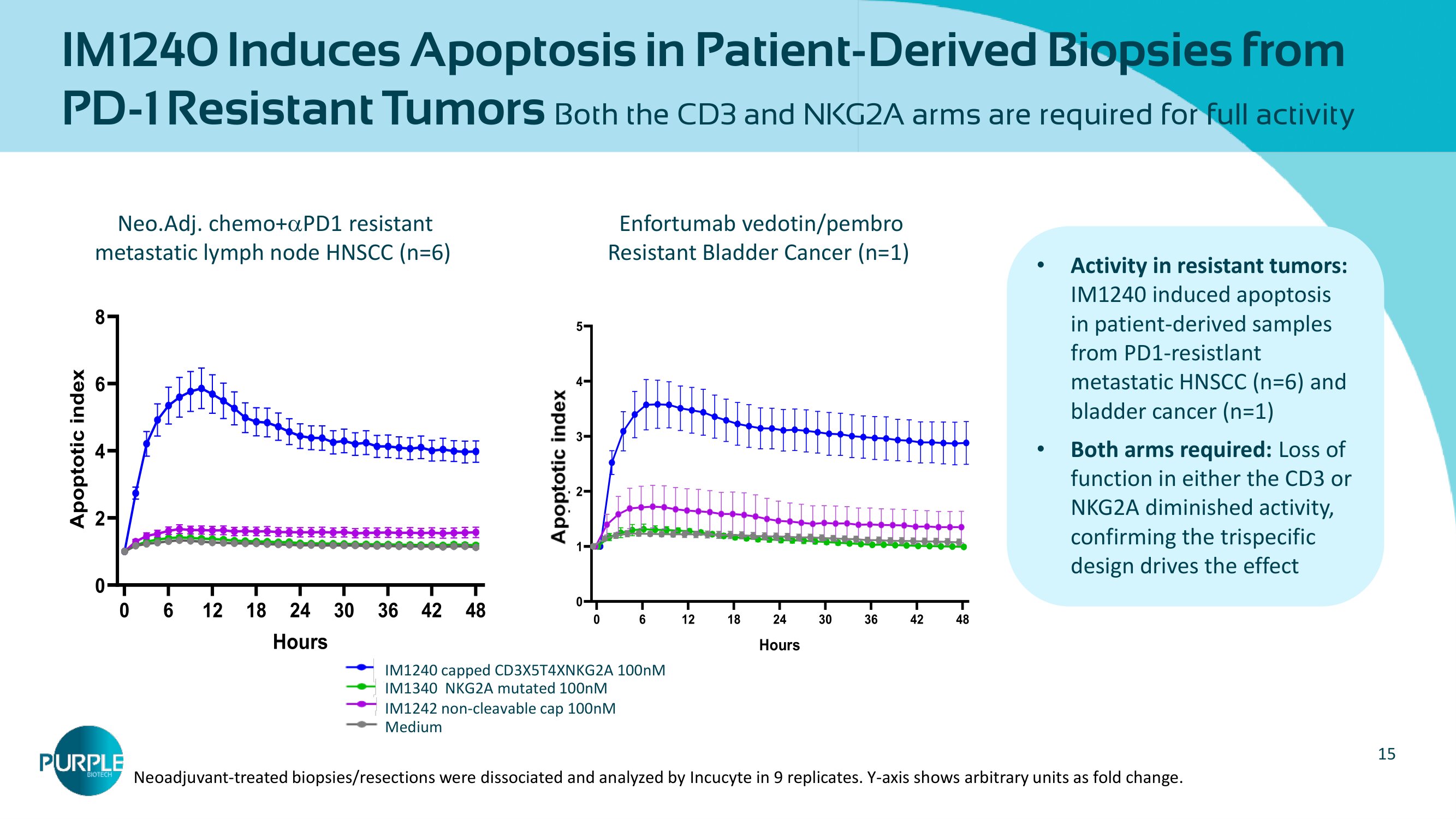
15 IM 1240 Induces Apoptosis in Patient - Derived Biopsies from PD - 1 Resistant Tumors Both the CD 3 and NKG 2 A arms are required for full activity • Activity in resistant tumors: IM 1240 induced apoptosis in patient - derived samples from PD 1 - resistlant metastatic HNSCC (n= 6 ) and bladder cancer (n= 1 ) • Both arms required: Loss of function in either the CD 3 or NKG 2 A diminished activity, confirming the trispecific design drives the effect Enfortumab vedotin/ pembro Resistant Bladder Cancer (n= 1 ) 0 6 12 18 24 30 36 42 48 0 2 4 6 8 Bladder (n=1) Hours A p o p t o t i c i n d e x Medium 1242 100 nM 1340 100 nM 1240 100 nM Neo.Adj . chemo+ PD 1 resistant metastatic lymph node HNSCC (n= 6 ) 0 6 12 18 24 30 36 42 48 0 1 2 3 4 5 Hours A p o p t o s i s i n d e x Media IM1242 [100nM] IM1340 [100nM] IM1240 [100nM] Neo. Adj. Chemo+IO - Resistant HNSCC (n=6) IM1242 non - cleavable cap 100nM IM 1340 NKG 2 A mutated 100 nM IM 1240 capped CD 3 X 5 T 4 XNKG 2 A 100 nM Medium Neoadjuvant - treated biopsies/resections were dissociated and analyzed by Incucyte in 9 replicates. Y - axis shows arbitrary units as fold change.
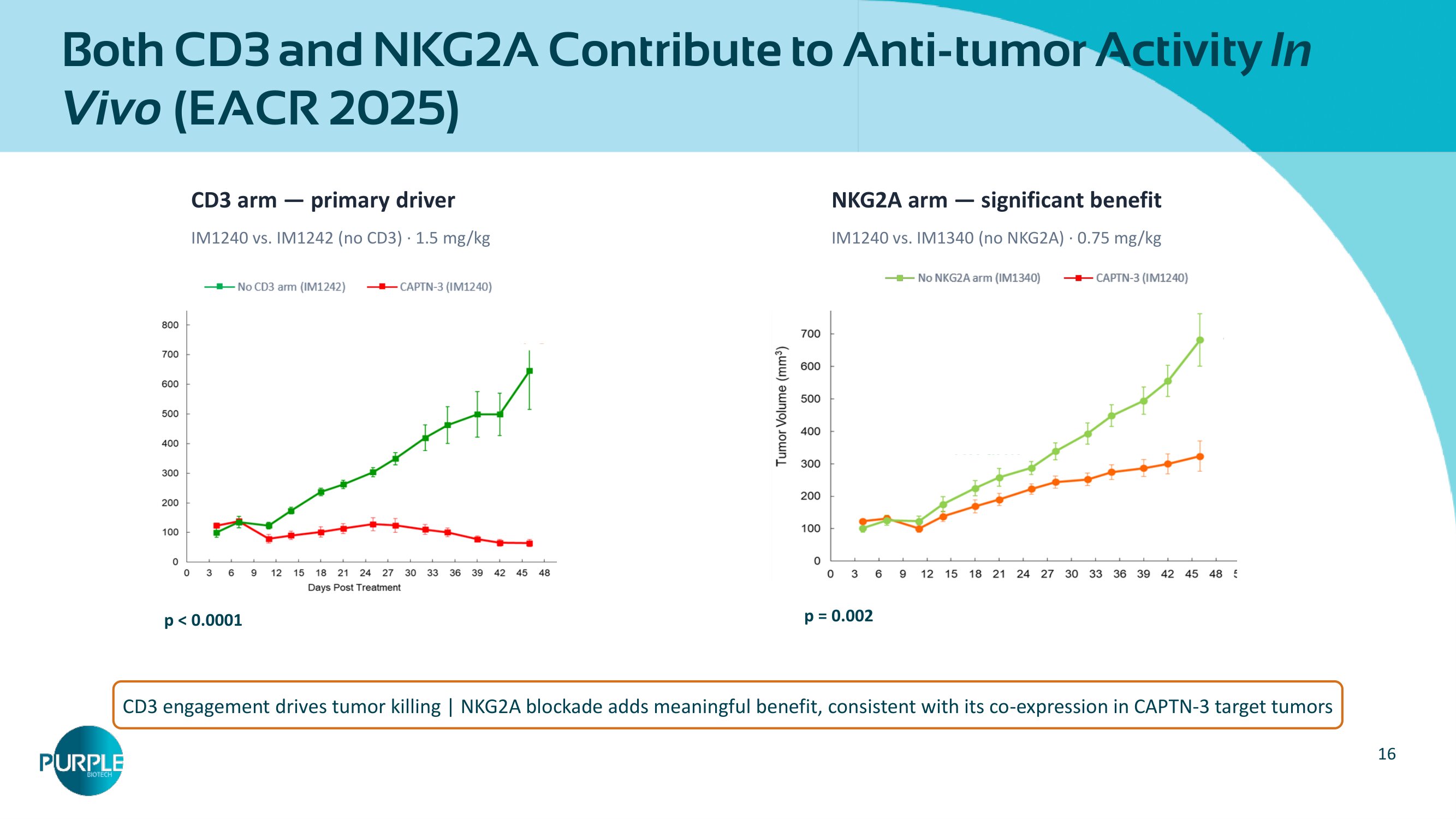
16 Both CD 3 and NKG 2 A Contribute to Anti - tumor Activity In Vivo (EACR 2025 ) CD 3 arm — primary driver IM1240 vs. IM1242 (no CD3) · 1.5 mg/kg NKG 2 A arm — significant benefit IM 1240 vs. IM 1340 (no NKG 2 A) · 0.75 mg/kg CD 3 engagement drives tumor killing | NKG 2 A blockade adds meaningful benefit, consistent with its co - expression in CAPTN - 3 target tumors p = 0.002 p < 0.0001
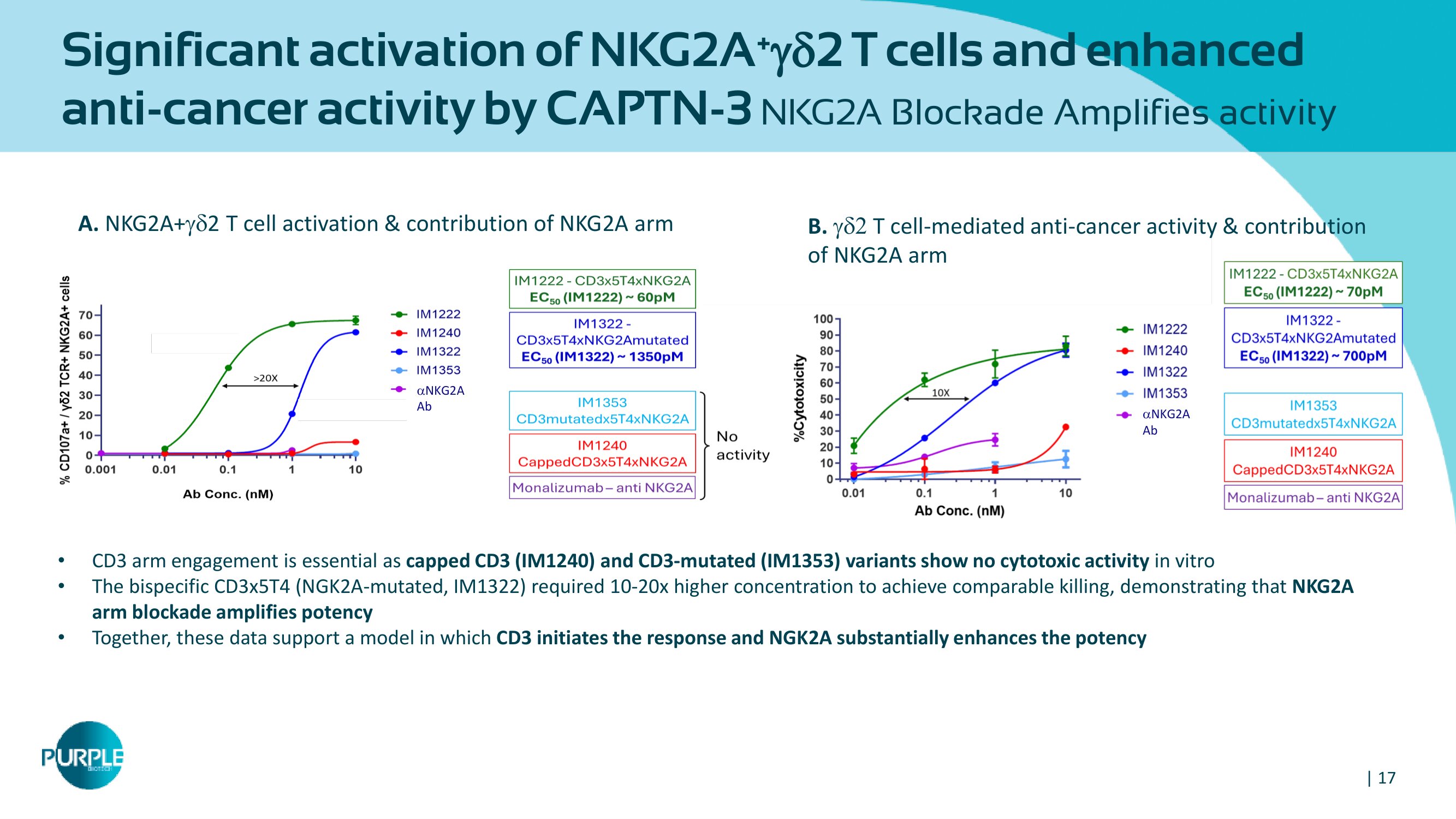
| 17 A. NKG 2 A+ 2 T cell activation & contribution of NKG 2 A arm B. T cell - mediated anti - cancer activity & contribution of NKG2A arm • CD 3 arm engagement is essential as capped CD 3 (IM 1240 ) and CD 3 - mutated (IM 1353 ) variants show no cytotoxic activity in vitro • The bispecific CD 3 x 5 T 4 ( NGK 2 A - mutated, IM 1322 ) required 10 - 20 x higher concentration to achieve comparable killing, demonstrating that NKG 2 A arm blockade amplifies potency • Together, these data support a model in which CD 3 initiates the response and NGK 2 A substantially enhances the potency NKG 2 A Ab NKG 2 A Ab Significant activation of NKG2A + 2 T cells and enhanced anti - cancer activity by CAPTN - 3 NKG2A Blockade Amplifies activity
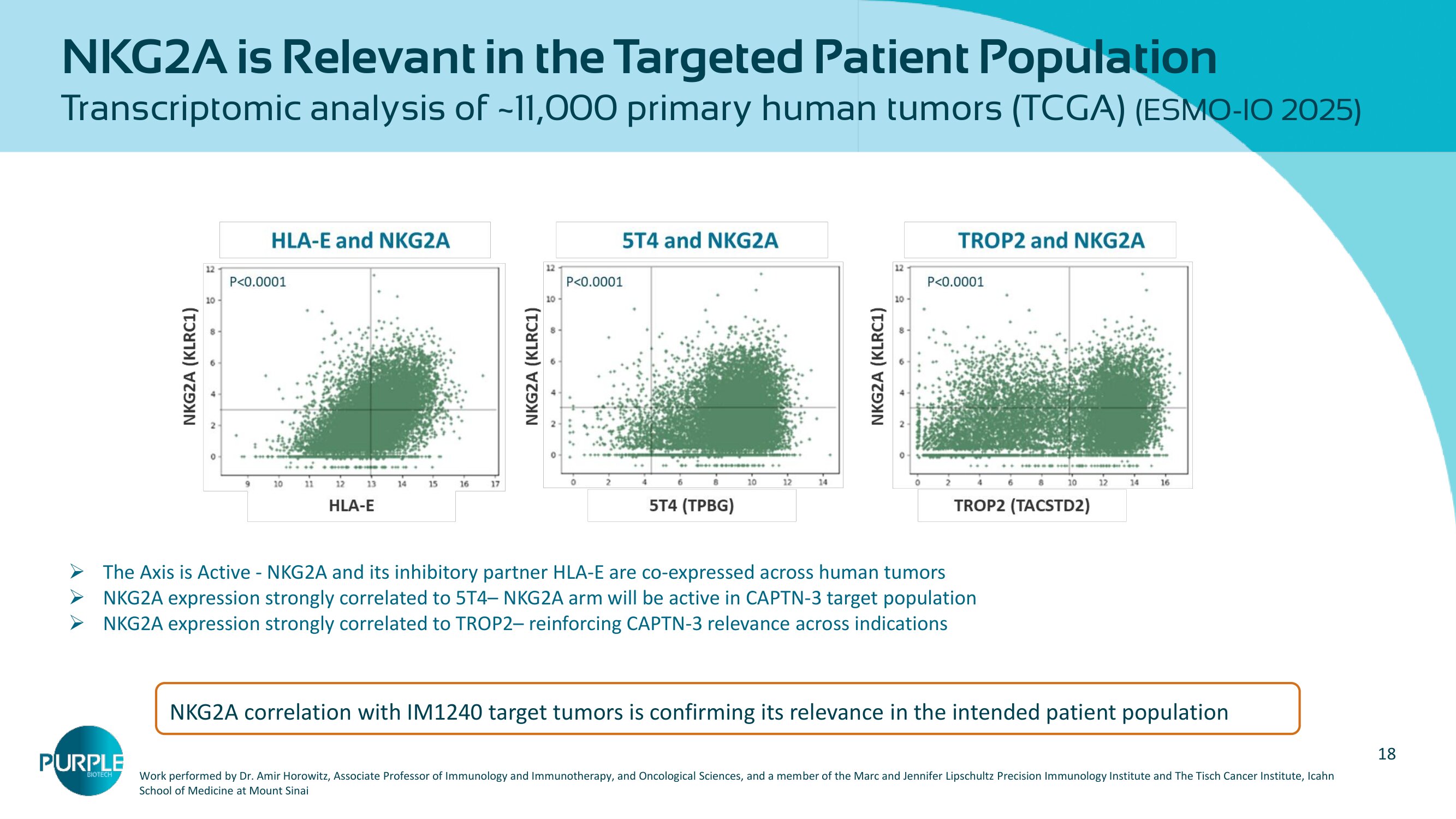
18 NKG 2 A is Relevant in the Targeted Patient Population Transcriptomic analysis of ~ 11,000 primary human tumors (TCGA) (ESMO - IO 2025 ) » The Axis is Active - NKG 2 A and its inhibitory partner HLA - E are co - expressed across human tumors » NKG 2 A expression strongly correlated to 5 T 4 – NKG 2 A arm will be active in CAPTN - 3 target population » NKG 2 A expression strongly correlated to TROP 2 – reinforcing CAPTN - 3 relevance across indications Work performed by Dr. Amir Horowitz, Associate Professor of Immunology and Immunotherapy, and Oncological Sciences, and a mem ber of the Marc and Jennifer Lipschultz Precision Immunology Institute and The Tisch Cancer Institute, Icahn School of Medicine at Mount Sinai NKG 2 A correlation with IM 1240 target tumors is confirming its relevance in the intended patient population
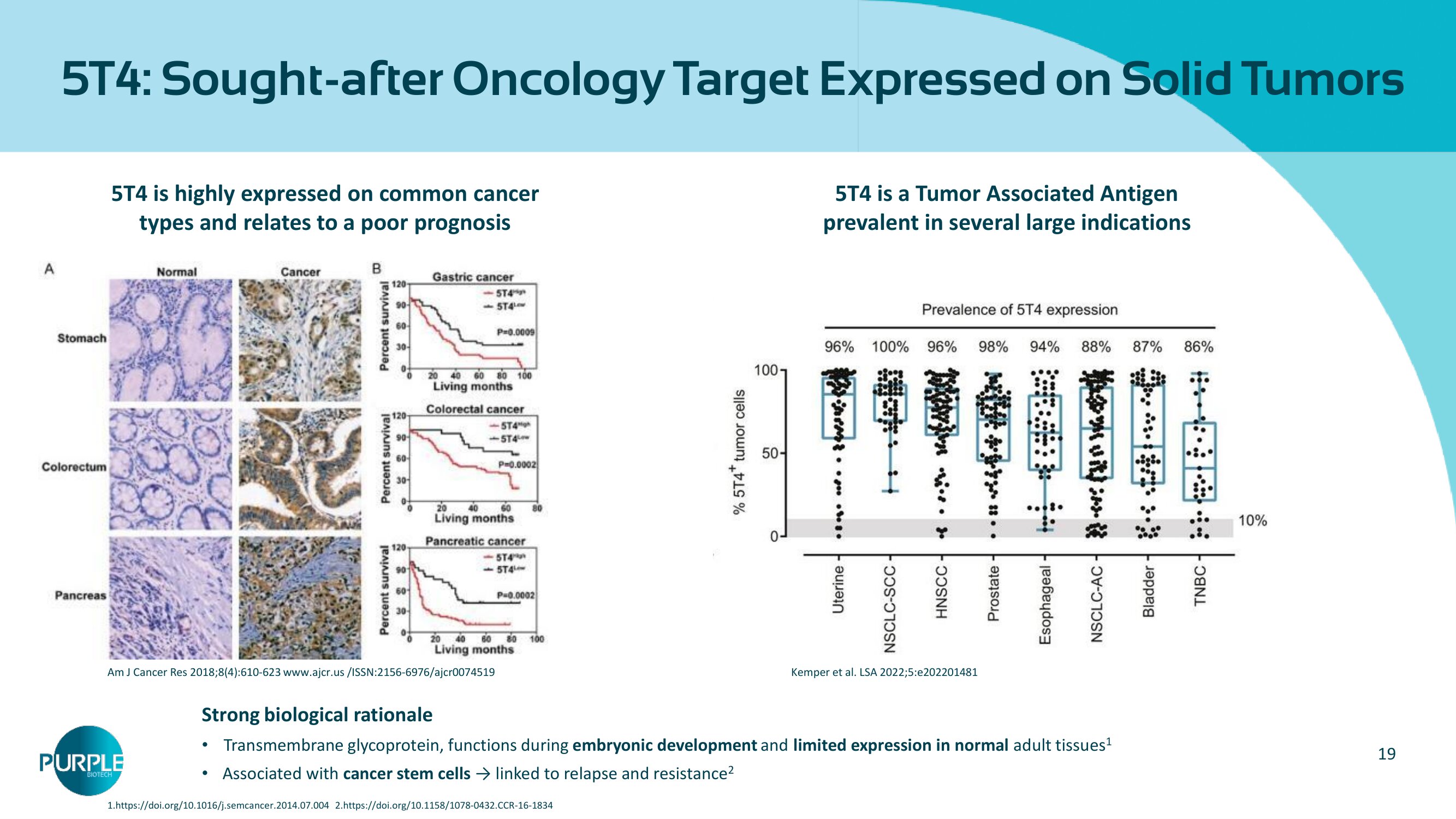
19 5 T 4 : Sought - after Oncology Target Expressed on Solid Tumors 5 T 4 is highly expressed on common cancer types and relates to a poor prognosis Am J Cancer Res 2018;8(4):610 - 623 www.ajcr.us /ISSN:2156 - 6976/ajcr0074519 5 T 4 is a Tumor Associated Antigen prevalent in several large indications Kemper et al. LSA 2022;5:e202201481 Strong biological rationale • Transmembrane glycoprotein, functions during embryonic development and limited expression in normal adult tissues 1 • Associated with cancer stem cells → linked to relapse and resistance 2 1 .https://doi.org/ 10.1016 /j.semcancer. 2014.07.004 2 . https://doi.org/ 10.1158 / 1078 - 0432 .CCR - 16 - 1834
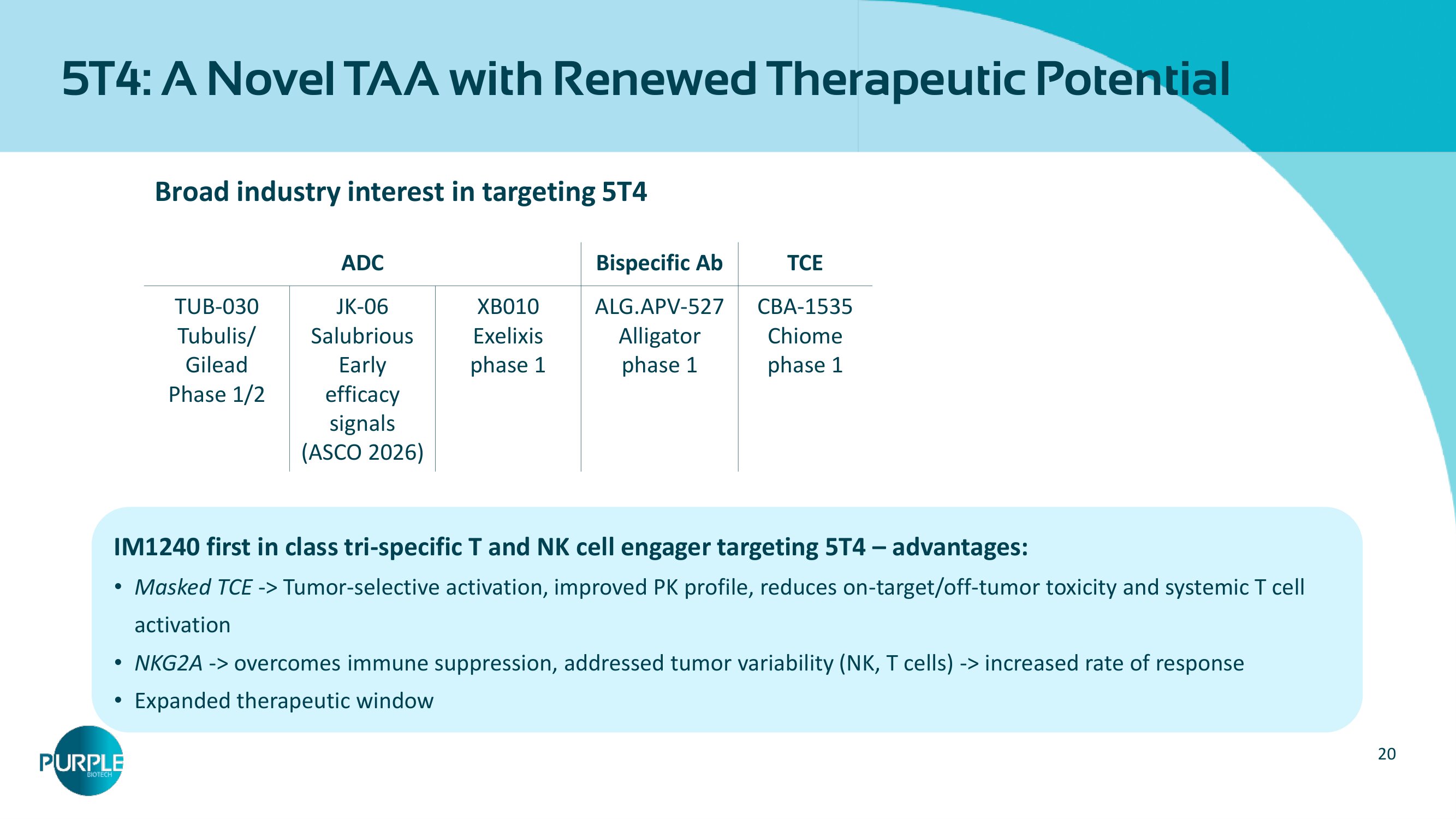
20 5 T 4 : A Novel TAA with Renewed Therapeutic Potential IM1240 fi rst in class tri - specific T and NK cell engager targeting 5T4 – advantages: • Masked TCE - > Tumor - selective activation, improved PK profile, reduces on - target/off - tumor toxicity and systemic T cell activation • NKG2A - > overcomes immune suppression, addressed tumor variability (NK, T cells) - > increased rate of response • Expanded therapeutic window Broad industry interest in targeting 5 T 4 TCE Bispecific Ab ADC CBA - 1535 Chiome phase 1 ALG.APV - 527 Alligator phase 1 XB010 Exelixis phase 1 JK - 06 Salubrious Early efficacy signals (ASCO 2026) TUB - 030 Tubulis / Gilead Phase 1/2
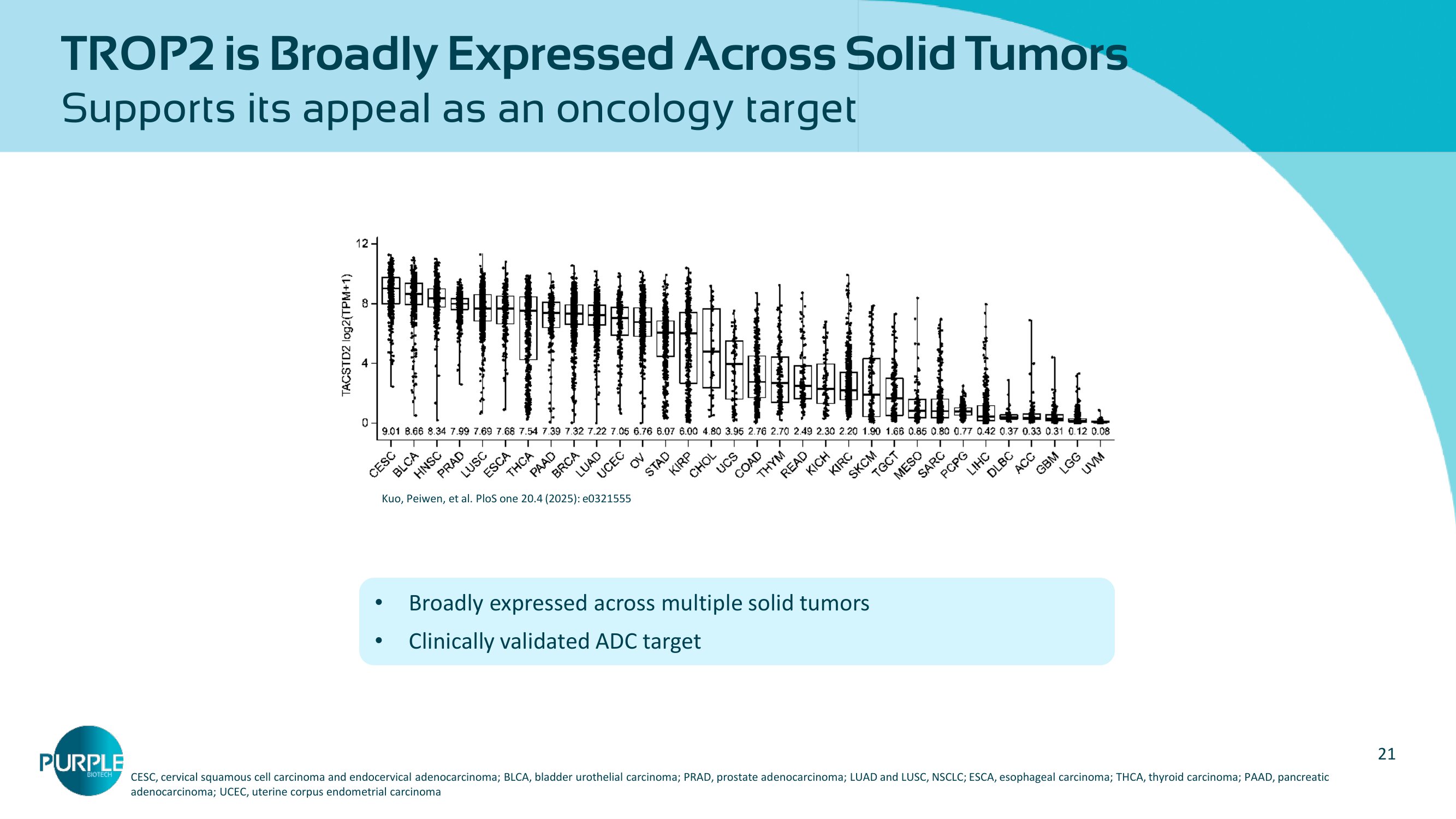
21 TROP2 is B roadly E xpressed A cross S olid T umors Supports its appeal as an oncology target Kuo, Peiwen, et al. PloS one 20.4 (2025): e0321555 CESC, cervical squamous cell carcinoma and endocervical adenocarcinoma; BLCA, bladder urothelial carcinoma; PRAD, prostate ad eno carcinoma; LUAD and LUSC, NSCLC; ESCA, esophageal carcinoma; THCA, thyroid carcinoma; PAAD, pancreatic adenocarcinoma; UCEC, uterine corpus endometrial carcinoma • Broadly expressed across multiple solid tumors • Clinically validated ADC target
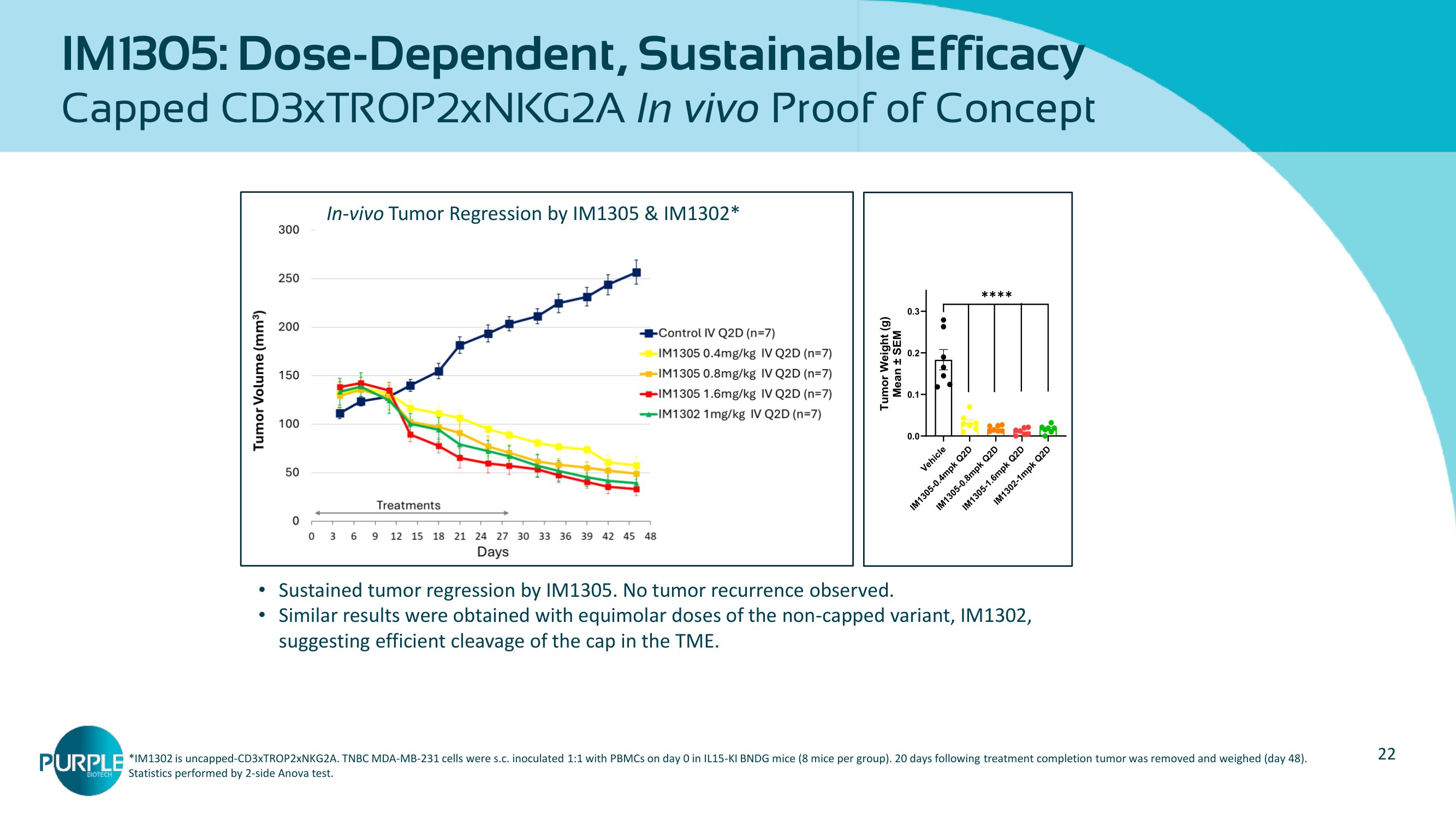
22 IM 1305 : Dose - Dependent, Sustainable Efficacy Capped CD 3 xTROP 2 xNKG 2 A In vivo Proof of Concept In - vivo Tumor Regression by IM1305 & IM1302* • Sustained tumor regression by IM 1305 . No tumor recurrence observed. • Similar results were obtained with equimolar doses of the non - capped variant, IM 1302 , suggesting efficient cleavage of the cap in the TME. *IM 1302 is uncapped - CD ϯ xTROP 2 xNKG 2 A. TNBC MDA - MB - 231 cells were s.c. inoculated 1:1 with PBMCs on day 0 in IL 15 - KI BNDG mice ( 8 mice per group). 20 days following treatment completion tumor was removed and weighed (day 48 ). Statistics performed by 2 - side Anova test.
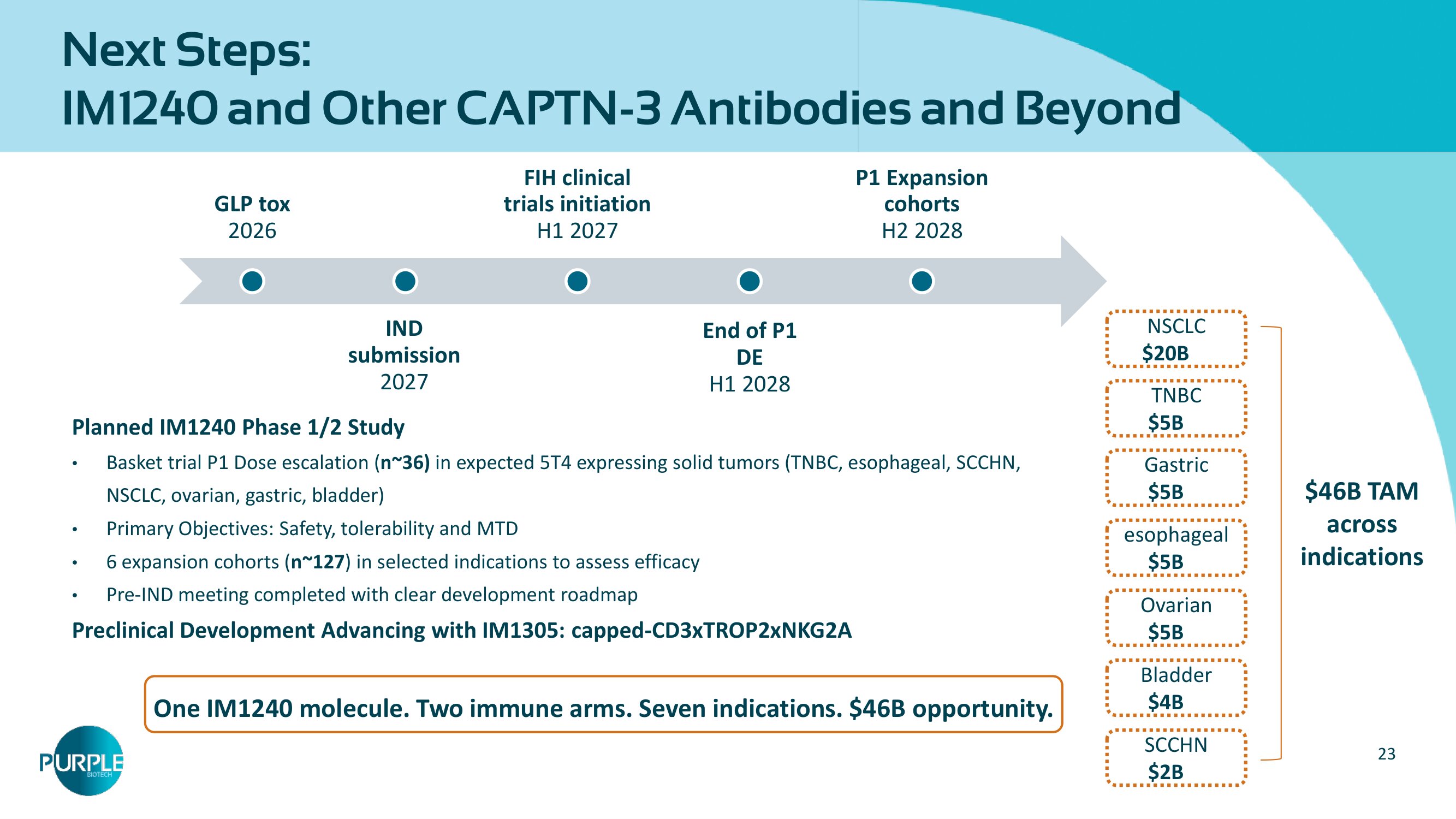
23 Next Steps: IM1240 and Other CAPTN - 3 Antibodies and Beyond GLP tox 2026 IND submission 2027 FIH clinical trials initiation H 1 2027 End of P1 DE H1 2028 P 1 Expansion cohorts H 2 2028 Planned IM 1240 Phase 1 / 2 Study • Basket trial P 1 Dose escalation ( n~ 36 ) in expected 5 T 4 expressing solid tumors (TNBC, esophageal, SCCHN, NSCLC, ovarian, gastric, bladder) • Primary Objectives: Safety, tolerability and MTD • 6 expansion cohorts ( n~ 127 ) in selected indications to assess efficacy • Pre - IND meeting completed with clear development roadmap Preclinical Development Advancing with IM 1305 : capped - CD 3 xTROP 2 xNKG 2 A NSCLC $20B LC Ovarian $5B LC esophageal $ 5 B LC Gastric $ 5 B LC $ 46 B TAM across indications Bladder $4B LC TNBC $ 5 B LC SCCHN $ 2 B LC One IM1240 molecule. Two immune arms. Seven indications. $46B opportunity.
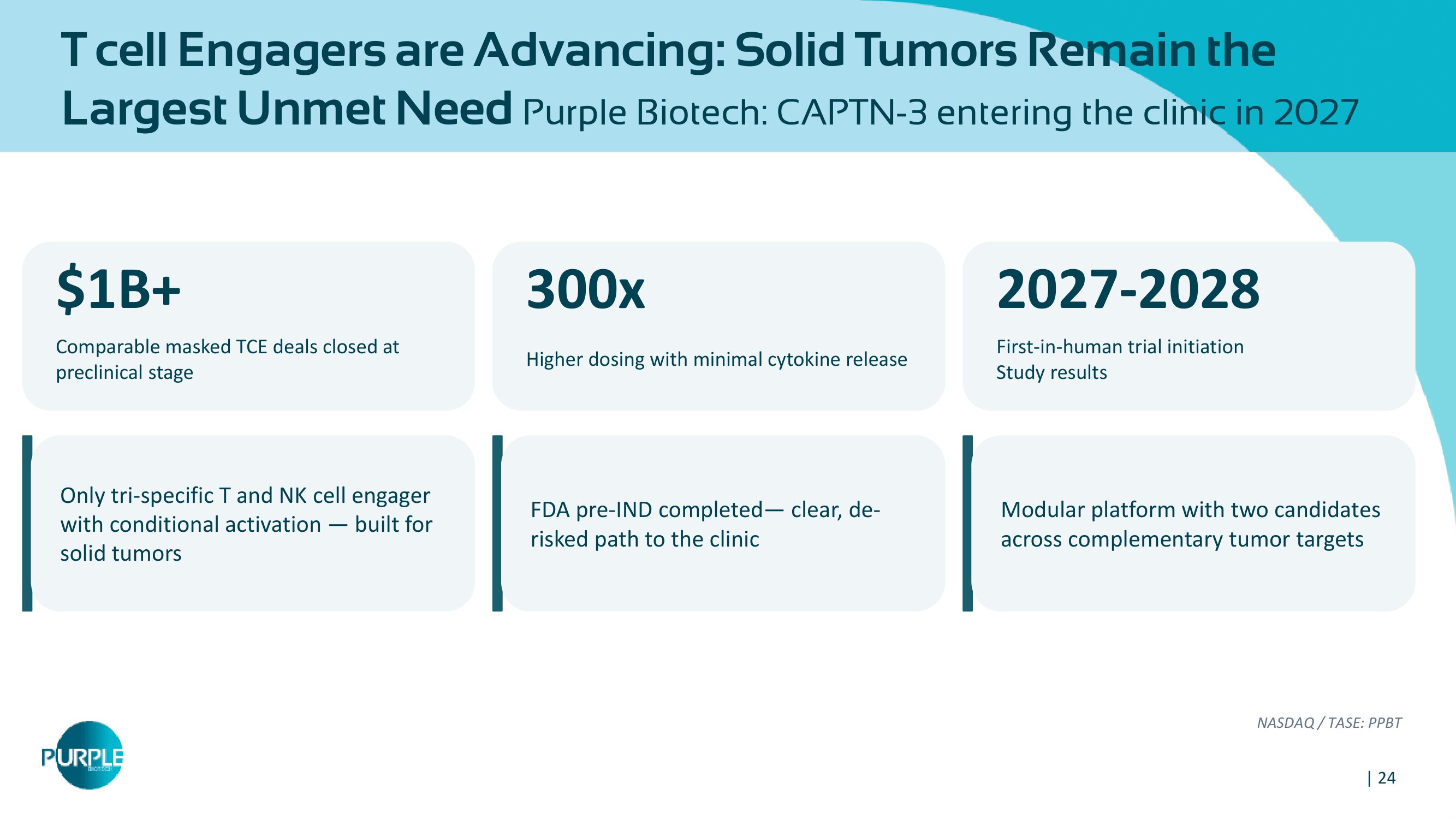
| 24 T cell Engagers are Advancing: Solid Tumors Remain the Largest Unmet Need Purple Biotech: CAPTN - 3 entering the clinic in 2027 $ 1 B+ Comparable masked TCE deals closed at preclinical stage 300x Higher dosing with minimal cytokine release Only tri - specific T and NK cell engager with conditional activation — built for solid tumors FDA pre - IND completed — clear, de - risked path to the clinic NASDAQ / TASE: PPBT 2027 - 2028 First - in - human trial initiation Study results Modular platform with two candidates across complementary tumor targets

| 25 2 Lead program expected to enter the clinic in 2027 IM1240 (cappedCD3x 5T4 xNKG2A), a first - in - class CAPTN - 3 tri - specific antibody Second program, IM1305 (cappedCD3x TROP2 xNKG2A) 1 CAPTN - 3 : differentiated tri - specific platform activating both innate and adaptive immune systems The only platform engaging both T cells AND NK cells while incorporating a masking technology 5 Solid tumors remain largely untreated by T cell engagers A large unmet need with no approved tri - specific option 4 Focused on key inflection point and significant market potential to create value Comparable masked TCE programs secured >$1B deals at preclinical stage. Key catalyst - results from P1 study starting from 1H 2028 FINANCIALS Cash $ 6.4 M Runway INTO H1 2027 Exchange NASDAQ + TASE PPBT As of March 31, 2026 Snapshot: Company Highlights 3 Safety and efficacy demonstrated in IND enabling Studies Strong anti - tumor activity and 300 п improved safety profile versus the non - masked comparator

| 26 Leadership Team Michael Schickler, PhD Head of Clinical and Regulatory Affairs Formerly at Hoffmann - La Roche, CEO at CureTech Hadas Reuveni, PhD VP Research & Development Formerly at Keryx (NASDAQ:KERX) Gil Efron Chief Executive Officer Former Deputy CEO & CFO at Kamada (NASDAQ:KMDA) Eric K. Rowinsky, MD Chairman of the Board Former CMO at ImClone, Stemline , Board member at Biogen Inc. Shai Lankry Chief Financial Officer Former CFO at Gamida Cell Ltd. (NASDAQ:GMDA)

27 Contact Us: ir@purple - biotech.com THANK YOU
Appendix: CAPTN - 3
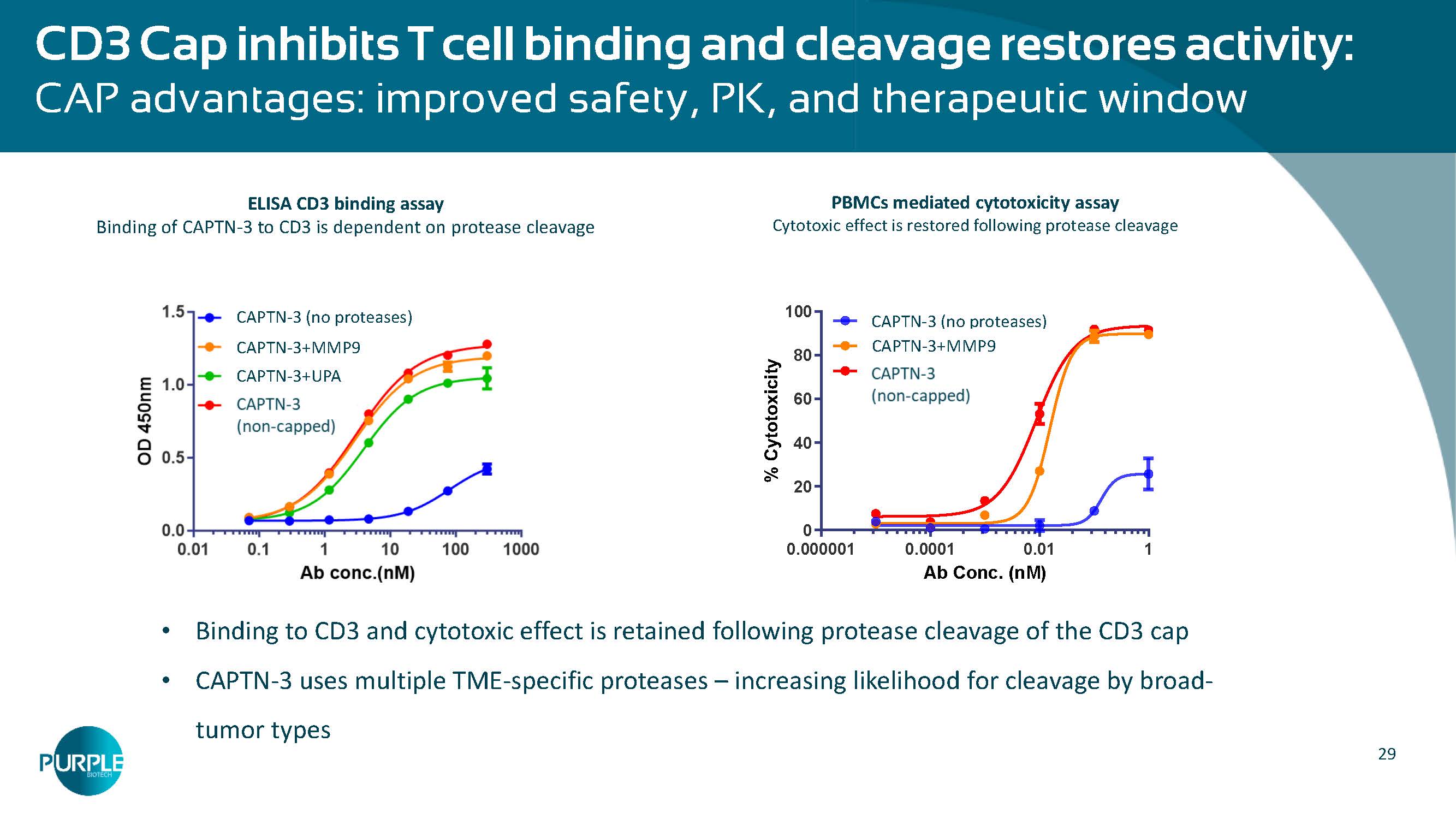
29 • Binding to CD 3 and cytotoxic effect is retained following protease cleavage of the CD 3 cap • CAPTN - 3 uses multiple TME - specific proteases – increasing likelihood for cleavage by broad - tumor types CD 3 Cap inhibits T cell binding and cleavage restores activity: CAP advantages: improved safety, PK, and therapeutic window PBMCs mediated cytotoxicity assay Cytotoxic effect is restored following protease cleavage ELISA CD 3 binding assay Binding of CAPTN - 3 to CD 3 is dependent on protease cleavage (no proteases) CAPTN - 3 (no proteases) CAPTN - 3 +MMP 9 CAPTN - 3 +UPA Ab Conc. (nM) % C y t o t o x i c i t y 0.000001 0.0001 0.01 1 0 20 40 60 80 100 ProTribody ProTribody + MMP9 TriBody (no proteases) CAPTN - 3 (no proteases) CAPTN - 3 +MMP 9
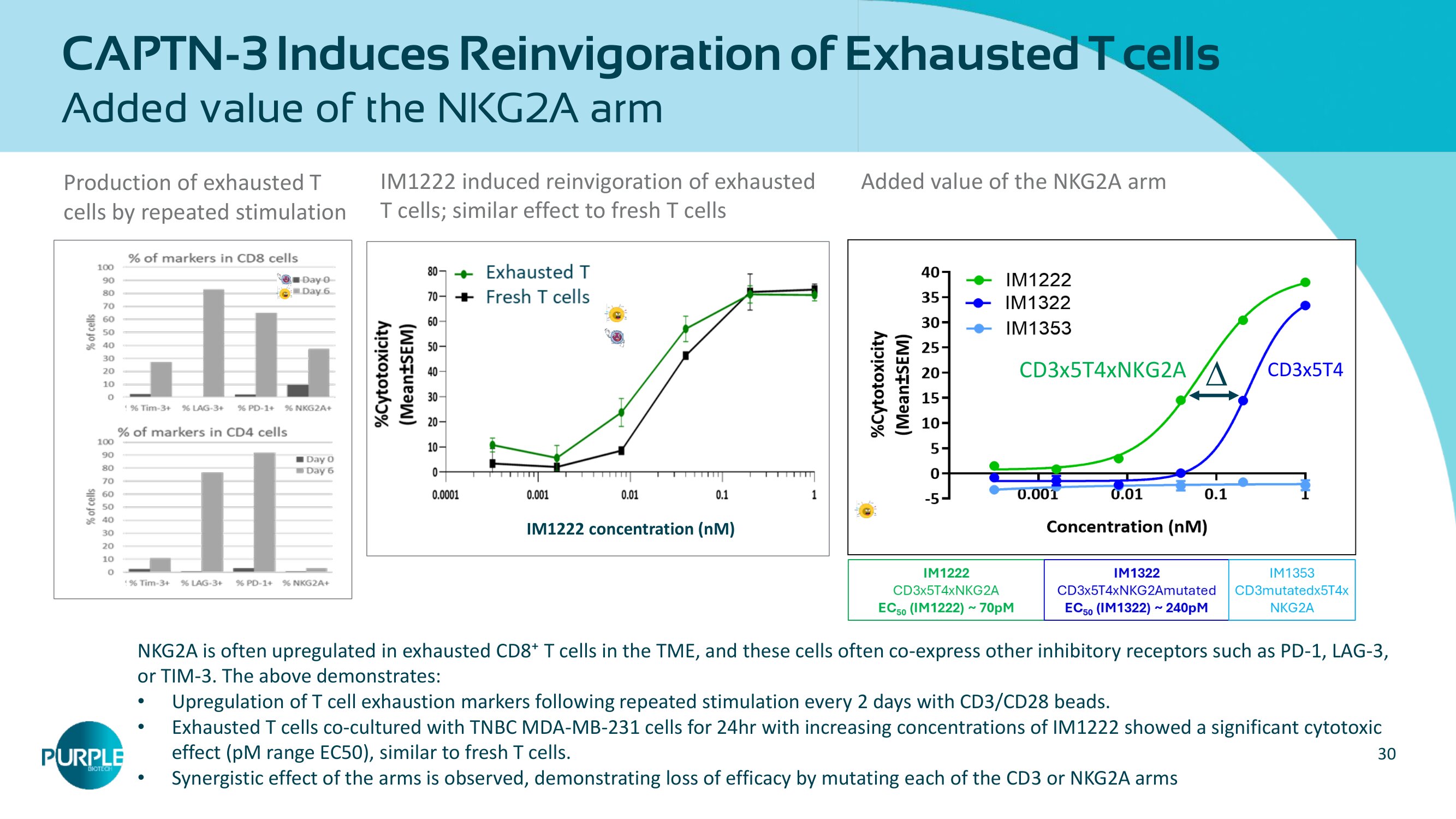
30 CAPTN - 3 Induces Reinvigoration of Exhausted T cells Added value of the NKG2A arm IM 1222 induced reinvigoration of exhausted T cells; similar effect to fresh T cells Production of exhausted T cells by repeated stimulation Added value of the NKG 2 A arm IM1222 concentration ( nM ) CD 3 x 5 T 4 CD 3 x 5 T 4 xNKG 2 A NKG2A is often upregulated in exhausted CD8⁺ T cells in the TME, and these cells often co - express other inhibitory receptors suc h as PD - 1, LAG - 3, or TIM - 3. The above demonstrates: • Upregulation of T cell exhaustion markers following repeated stimulation every 2 days with CD3/CD28 beads. • Exhausted T cells co - cultured with TNBC MDA - MB - 231 cells for 24hr with increasing concentrations of IM1222 showed a significant cytotoxic effect ( pM range EC50), similar to fresh T cells. • Synergistic effect of the arms is observed, demonstrating loss of efficacy by mutating each of the CD3 or NKG2A arms
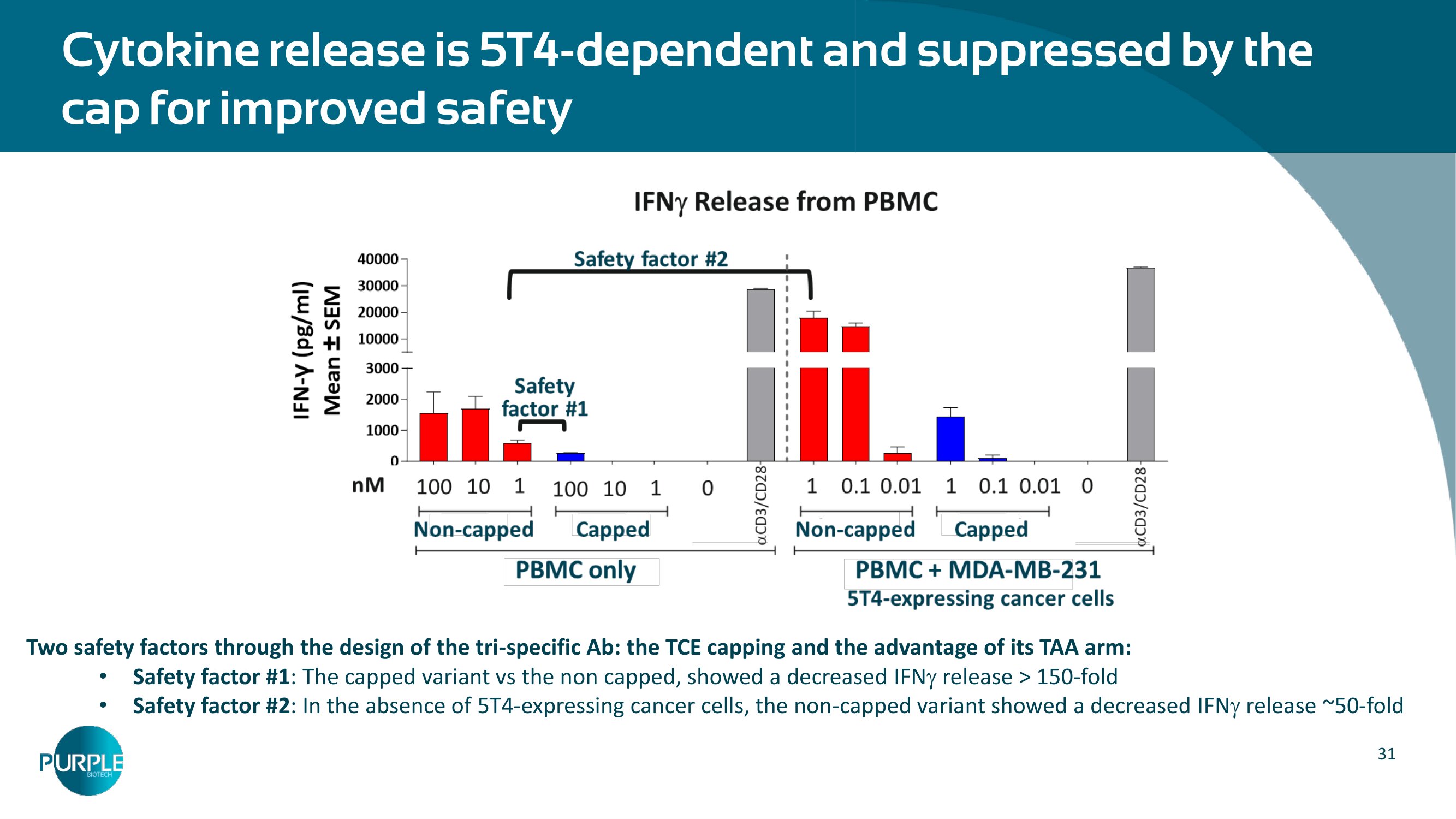
31 Cytokine release is 5 T 4 - dependent and suppressed by the cap for improved safety Two safety factors through the design of the tri - specific Ab: the TCE capping and the advantage of its TAA arm: • Safety factor # 1 : The capped variant vs the non capped, showed a decreased IFN release > 150 - fold • Safety factor # 2 : In the absence of 5 T 4 - expressing cancer cells, the non - capped variant showed a decreased IFN release ~ 50 - fold
CM 24 : an α - CEACAM 1 * mAb Significant opportunity in multiple large indications with unmet medical need Clinical POC achieved in PDAC *Carcinoembryonic Antigen Cell Adhesion Molecule
33 CM 24 : Targeting CEACAM 1 expressing tumors • CEACAM1 is overexpressed in >90% of colon, pancreatic and bladder cancers and in >70% in lung, gastric and biliary tract cancers • CEACAM1 is a part of the Neutrophil Extracellular Traps (NETs) structure Attractive new target • CM 24 increases T cell and NK cell - mediated cytotoxicity against tumors • CM 24 binds to CEACAM 1 on NETs and inhibits NET - related activities • CM 24 shows benefits in combination with immuno - oncology treatments Demonstrated mechanism of action • 19 % reduction in risk of death (HR=0. 81 ) and 2 5 % reduction in the risk of progression or death (HR=0.7 5 ) and 25% ORR, in metastatic PDAC as second - line treatment • Potential biomarkers: Serum CEACAM1 and MPO, C EA CAM1 + tumor cells and CPS PoC Clinical efficacy • Large opportunities to leverage the MoA in multiple indications (lung, colon, GI etc.) • Significant unmet medical need in pancreatic ductal adenocarcinoma (PDAC), the most common form of pancreatic cancer Sizable market potential
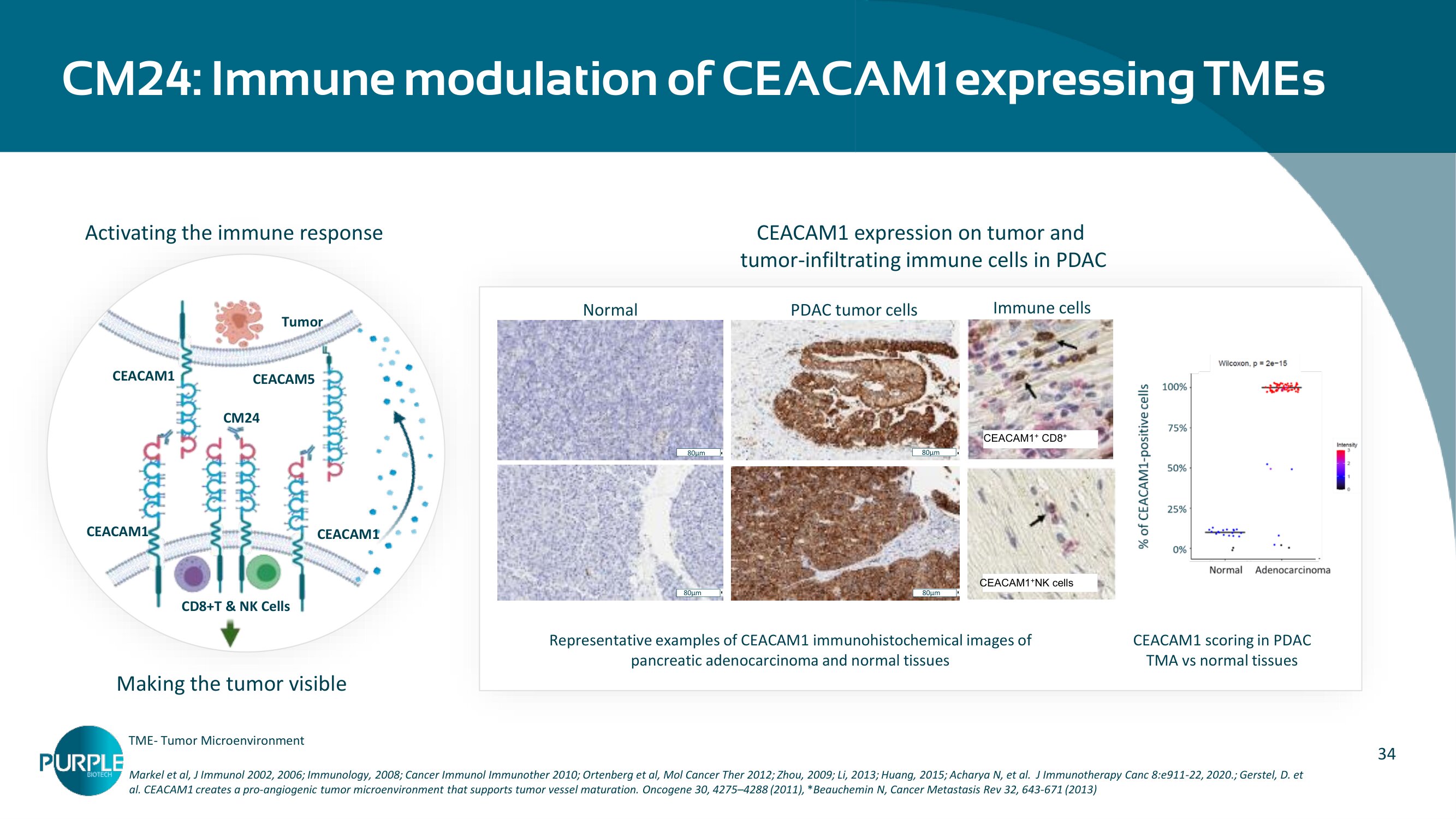
34 CM 24 : Immune modulation of CEACAM 1 expressing TMEs Markel et al, J Immunol 2002 , 2006 ; Immunology, 2008 ; Cancer Immunol Immunother 2010 ; Ortenberg et al, Mol Cancer Ther 2012 ; Zhou, 2009 ; Li, 2013 ; Huang, 2015 ; Acharya N, et al. J Immunotherapy Canc 8 :e 911 - 22 , 2020 . ; Gerstel, D. et al. CEACAM 1 creates a pro - angiogenic tumor microenvironment that supports tumor vessel maturation. Oncogene 30 , 4275 – 4288 ( 2011 ), * Beauchemin N, Cancer Metastasis Rev 32 , 643 - 671 ( 2013 ) CEACAM 1 expression on tumor and tumor - infiltrating immune cells in PDAC CEACAM1 scoring in PDAC TMA vs normal tissues Representative examples of CEACAM 1 immunohistochemical images of pancreatic adenocarcinoma and normal tissues CD PDAC tumor cells Normal 80 µm 80 µm 80 µm 80µm CEACAM 1 + CD 8 + CD CEACAM 1 + NK cells Immune cells Tumor CD 8 +T & NK Cells CEACAM 1 CEACAM1 CEACAM 1 CEACAM 5 CM 24 Activating the immune response Making the tumor visible TME - Tumor Microenvironment
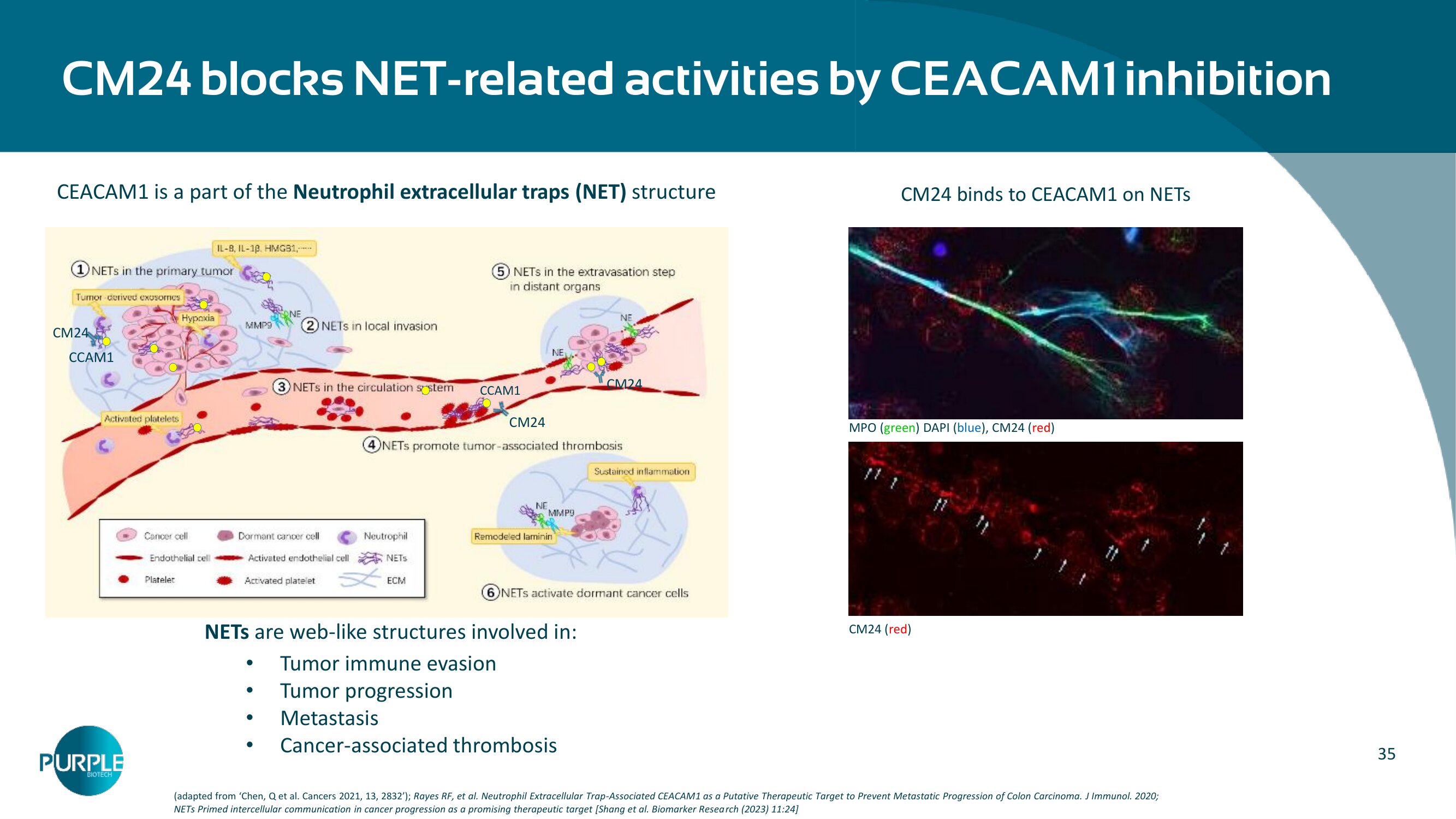
35 CCAM1 CM 24 CM 24 CCAM 1 CM24 CM 24 b locks NET - related activities by CEACAM 1 inhibition (adapted from ‘ Chen, Q et al. Cancers 2021 , 13 , 2832 ’ ); Rayes RF, et al. Neutrophil Extracellular Trap - Associated CEACAM 1 as a Putative Therapeutic Target to Prevent Metastatic Progression of Colon Carcinoma. J Immunol. 2020 ; NETs Primed intercellular communication in cancer progression as a promising therapeutic target [Shang et al. Biomarker Resea rch ( 2023 ) 11:24 ] CEACAM 1 is a part of the Neutrophil extracellular traps ( NET) structure MPO ( green ) DAPI ( blue ), CM24 ( red ) CM 24 ( red ) CM 24 binds to CEACAM 1 on NETs NETs are web - like structures involved in: • Tumor immune evasion • Tumor progression • Metastasis • Cancer - associated thrombosis
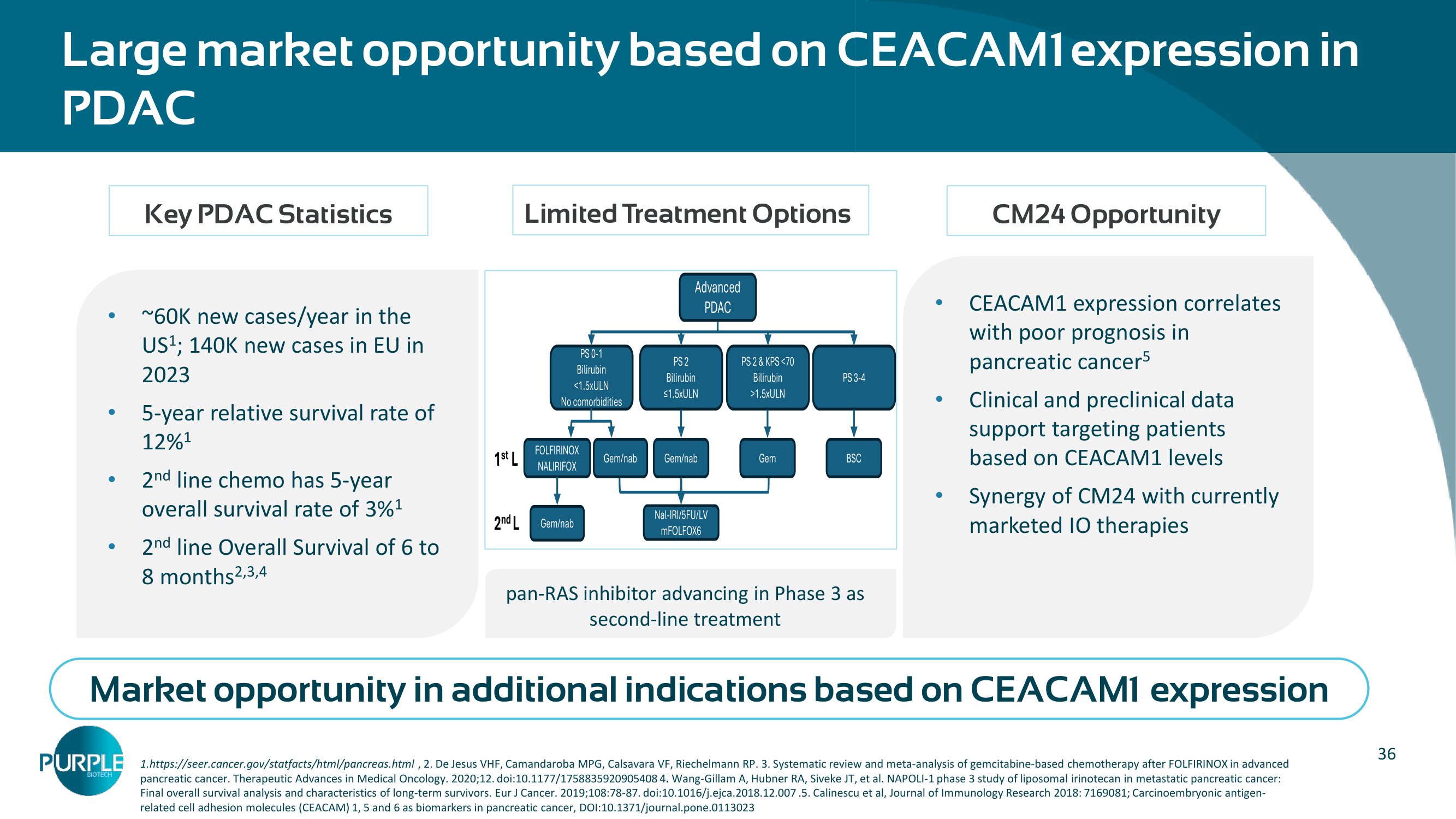
36 Large market opportunity based on CEACAM 1 expression in PDAC 1 .https://seer.cancer.gov/ statfacts /html/pancreas.html , 2 . De Jesus VHF, Camandaroba MPG, Calsavara VF, Riechelmann RP. 3 . Systematic review and meta - analysis of gemcitabine - based chemotherapy after FOLFIRINOX in advanced pancreatic cancer. Therapeutic Advances in Medical Oncology. 2020 ; 12 . doi: 10.1177 / 1758835920905408 4 . Wang - Gillam A, Hubner RA, Siveke JT, et al. NAPOLI - 1 phase 3 study of liposomal irinotecan in metastatic pancreatic cancer: Final overall survival analysis and characteristics of long - term survivors. Eur J Cancer. 2019 ; 108:78 - 87 . doi: 10.1016 /j.ejca. 2018.12.007 . 5 . Calinescu et al, Journal of Immunology Research 2018 : 7169081 ; Carcinoembryonic antigen - related cell adhesion molecules (CEACAM) 1 , 5 and 6 as biomarkers in pancreatic cancer, DOI: 10.1371 /journal.pone. 0113023 • ~ 60 K new cases/year in the US 1 ; 140 K new cases in EU in 2023 • 5 - year relative survival rate of 12 % 1 • 2 nd line chemo has 5 - year overall survival rate of 3 % 1 • 2 nd line Overall Survival of 6 to 8 months 2,3,4 • CEACAM1 expression correlates with poor prognosis in pancreatic cancer 5 • Clinical and preclinical data support targeting patients based on CEACAM1 levels • Synergy of CM24 with currently marketed IO therapies Key PDAC Statistics Limited Treatment Options CM 24 Opportunity Market opportunity in additional indications based on CEACAM1 expression pan - RAS inhibitor advancing in Phase 3 as second - line treatment Advanced PDAC PS 0 - 1 Bilirubin <1.5xULN No comorbidities PS 2 Bilirubin ≤1.5xULN PS 2 & KPS <70 Bilirubin >1.5xULN PS 3 - 4 FOLFIRINOX NALIRIFO X Gem/nab Nal - IRI/5FU/LV mFOLFOX6 Gem/nab Gem BSC Gem/nab 1 st L 2 nd L
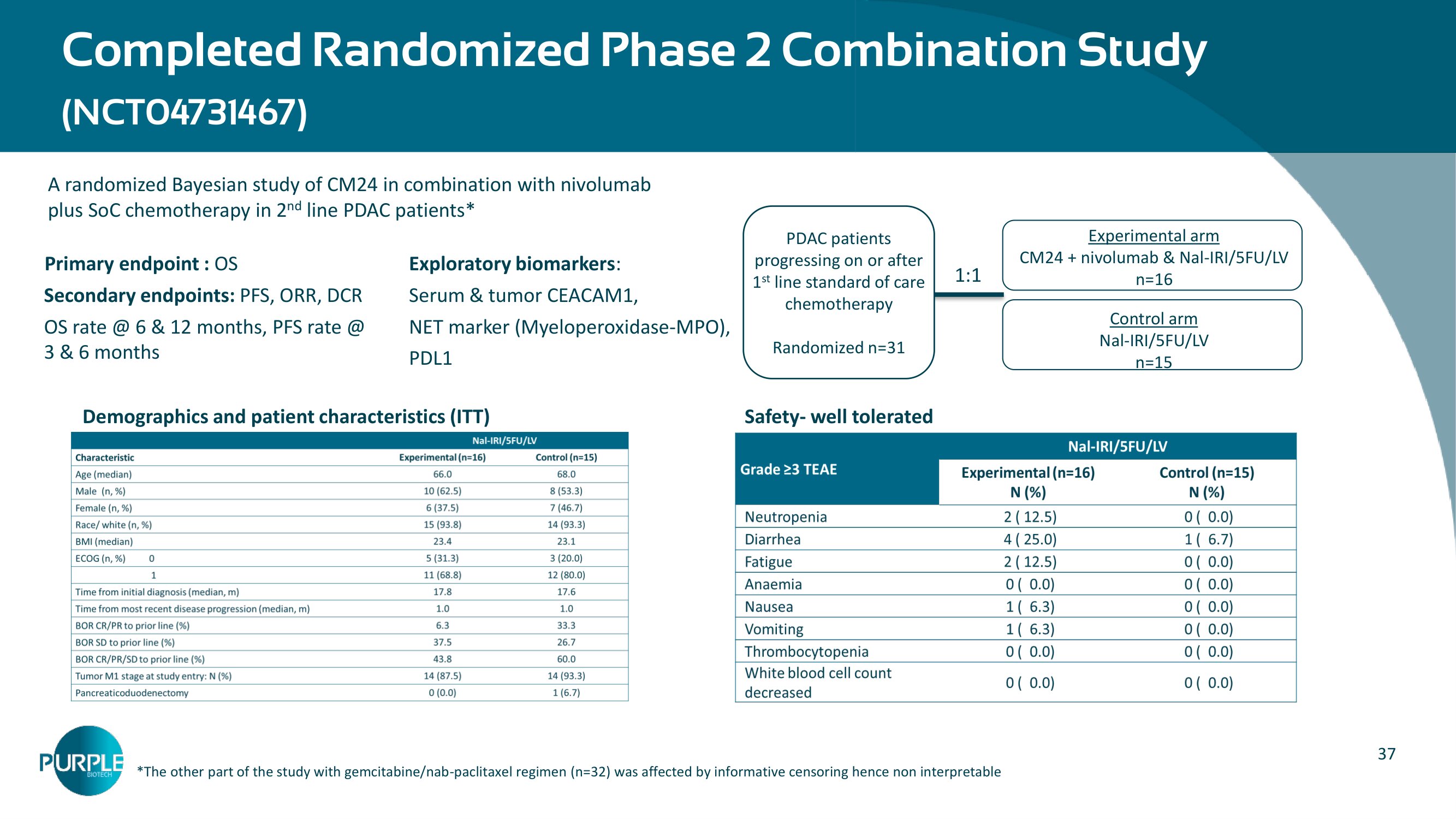
37 A randomized Bayesian study of CM24 in combination with nivolumab plus SoC chemotherapy in 2 nd line PDAC patients* Primary endpoint : OS Secondary endpoints: PFS, ORR, DCR OS rate @ 6 & 12 months, PFS rate @ 3 & 6 months Completed Randomized Phase 2 Combination Study (NCT 04731467 ) – Experimental arm CM 24 + nivolumab & Nal - IRI/ 5 FU/LV n= 16 Control arm Nal - IRI/5FU/LV n=15 PDAC patients progressing on or after 1 st line standard of care chemotherapy Randomized n= 31 1:1 * The other part of the study with gemcitabine/nab - paclitaxel regimen (n= 32 ) was affected by informative censoring hence non interpretable Safety - well tolerated Exploratory biomarkers : Serum & tumor CEACAM 1 , NET marker (Myeloperoxidase - MPO), PDL 1 Demographics and patient characteristics (ITT)
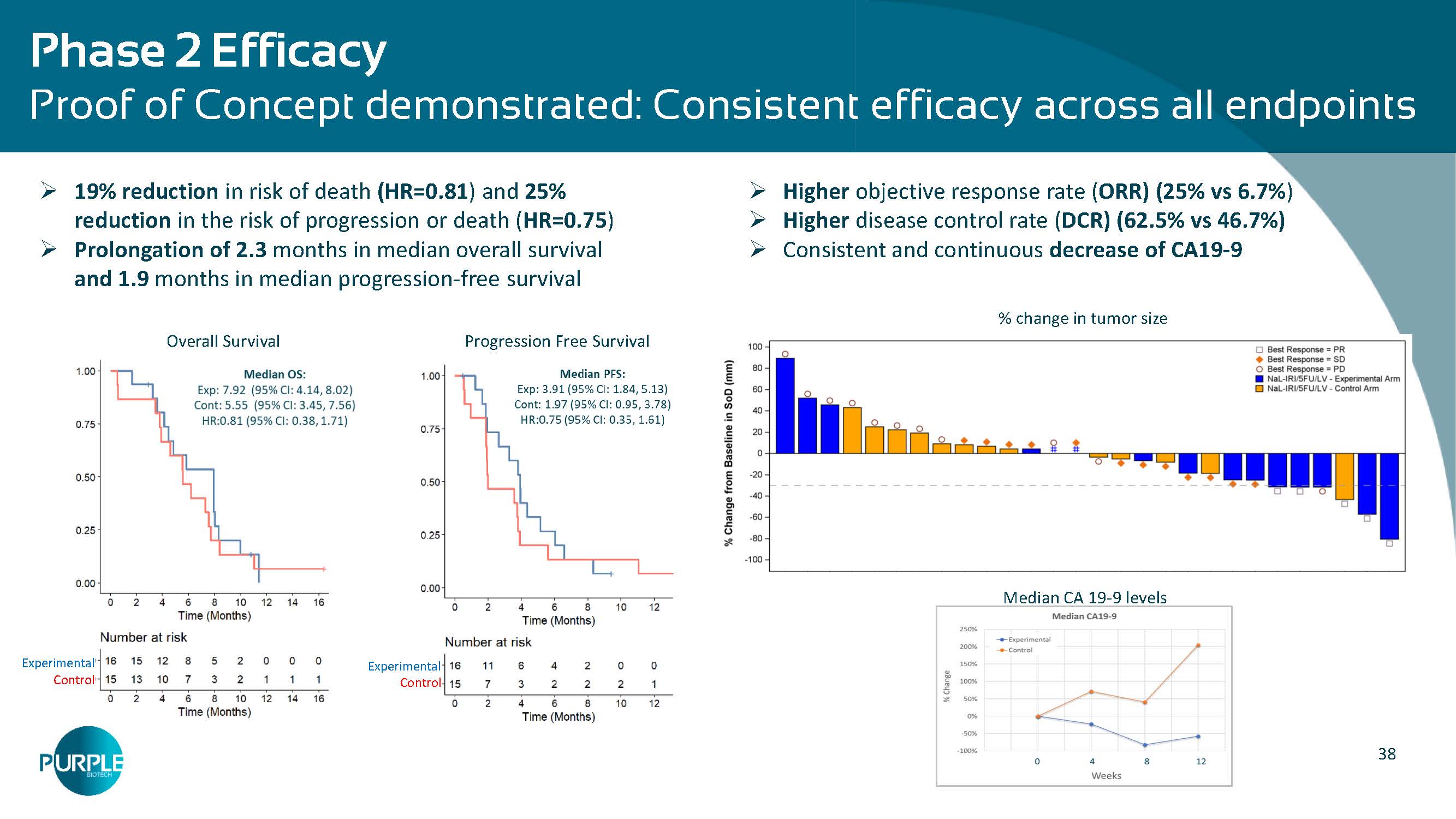
38 Phase 2 Efficacy Proof of Concept demonstrated: Consistent efficacy across all endpoints » Higher objective response rate ( ORR) ( 25 % vs 6.7 % ) » Higher disease control rate ( DCR) ( 62.5 % vs 46.7 %) » Consistent and continuous decrease of CA 19 - 9 Median CA 19 - 9 levels % change in tumor size » 19 % reduction in risk of death (HR=0. 81 ) and 2 5 % reduction in the risk of progression or death ( HR=0.7 5 ) » Prolongation of 2. 3 months in median overall survival and 1.9 months in median progression - free survival Overall Survival Progression Free Survival Experimental Control Experimental Control
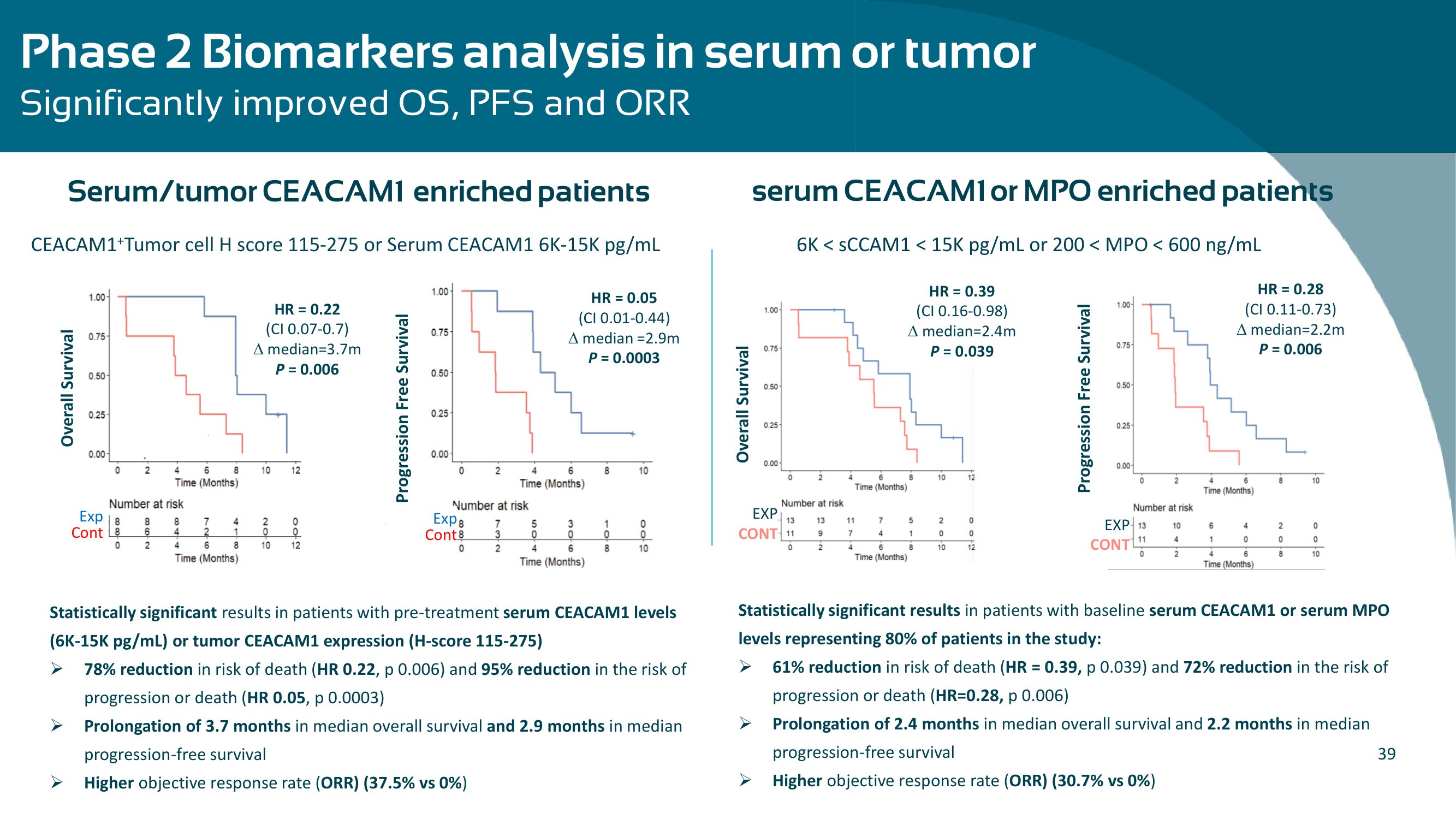
39 Phase 2 Biomarkers analysis in serum or tumor Significantly improved OS, PFS and ORR Statistically significant results in patients with pre - treatment serum CEACAM 1 levels ( 6 K - 15 K pg /mL) or tumor CEACAM 1 expression (H - score 115 - 275 ) » 78 % reduction in risk of death ( HR 0. 22 , p 0.006 ) and 95 % reduction in the risk of progression or death ( HR 0.05 , p 0.0003 ) » Prolongation of 3.7 months in median overall survival and 2 .9 months in median progression - free survival » Higher objective response rate ( ORR) ( 37.5 % vs 0 % ) serum CEACAM1 or MPO enriched patients CEACAM 1 + Tumor cell H score 115 - 275 or Serum CEACAM 1 6 K - 15 K pg /mL Overall Survival HR = 0.22 (CI 0.07 - 0.7 ) median= 3.7 m P = 0.006 Exp Cont Progression Free Survival HR = 0.05 (CI 0.01 - 0.44 ) median = 2.9 m P = 0.0003 Exp Cont Serum/tumor CEACAM1 enriched patients – EXP CONT 6 K < sCCAM 1 < 15 K pg /mL or 200 < MPO < 600 ng/mL Overall Survival EXP CONT HR = 0.39 (CI 0.16 - 0.98 ) median= 2.4 m P = 0.039 Progression Free Survival HR = 0.28 (CI 0.11 - 0.73 ) median= 2.2 m P = 0.006 Statistically significant results in patients with baseline serum CEACAM1 or serum MPO levels representing 80% of patients in the study : » 61 % reduction in risk of death ( HR = 0. 39, p 0.039 ) and 72 % reduction in the risk of progression or death ( HR =0.28, p 0.006 ) » Prolongation of 2 . 4 months in median overall survival and 2.2 months in median progression - free survival » Higher objective response rate ( ORR) (30.7% vs 0% )
NT 219 : Small Molecule Degrader of IRS 1 / 2 and Blocker of STAT 3 Recurrent/Metastatic Head & Neck Cancer (R/M SCCHN)
41 NT 219 : Novel IRS 1 / 2 and STAT 3 dual inhibitor for multiple indications • Covalently binds to Insulin Receptor Substrate IRS 1 / 2 and leads to their degradation • Dual inhibitor of STAT 3 & IRS 1 / 2 , both required to overcome drug resistance • Affects both the tumor and the TME • Suppresses cancer stem cells Innovative MOA • Outstanding efficacy in various PDX models in monotherapy and in combination • Potential in EGFRi , MAPKi and ICI resistant cancers Robust preclinical package • No DLTs in monotherapy or in combination • Early clinical proof - of - mechanism • Activated IGF 1 R and STAT 3 identified as potential predictive biomarkers • RP 2 D determined at 100 mg/kg , Phase 1 concluded. Phase 2 initiated Clinical Stage • Opportunity to establish a Standard of Care in 2 L r/m SCCHN patients • Multiple market upsides in combination with approved cancer treatments • NT 219 is the only IRS degrader available for clinical investigation Broad Market Potential
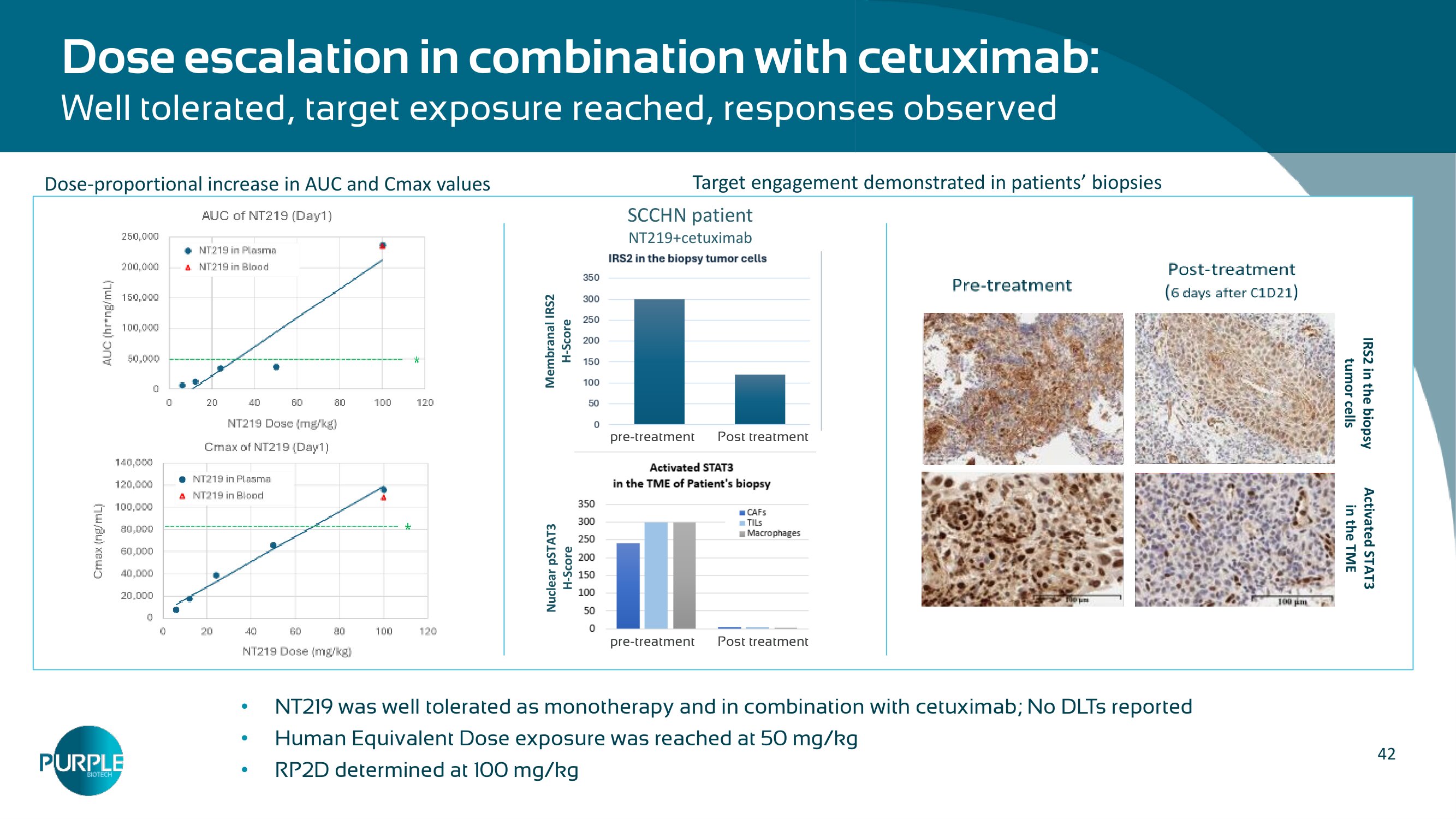
42 Dose escalation in combination with cetuximab: Well tolerated, target exposure reached, responses observed • NT 219 was well tolerated as monotherapy and in combination with cetuximab ; No DLTs reported • Human Equivalent Dose exposure was reached at 50 mg/kg • RP 2 D determined at 100 mg/kg IRS2 in the biopsy tumor cells Activated STAT 3 in the TME SCCHN patient NT 219 +cetuximab Nuclear pSTAT 3 H - Score Membranal IRS 2 H - Score pre - treatment Post treatment pre - treatment Post treatment Target engagement demonstrated in patients ’ biopsies Dose - proportional increase in AUC and Cmax values
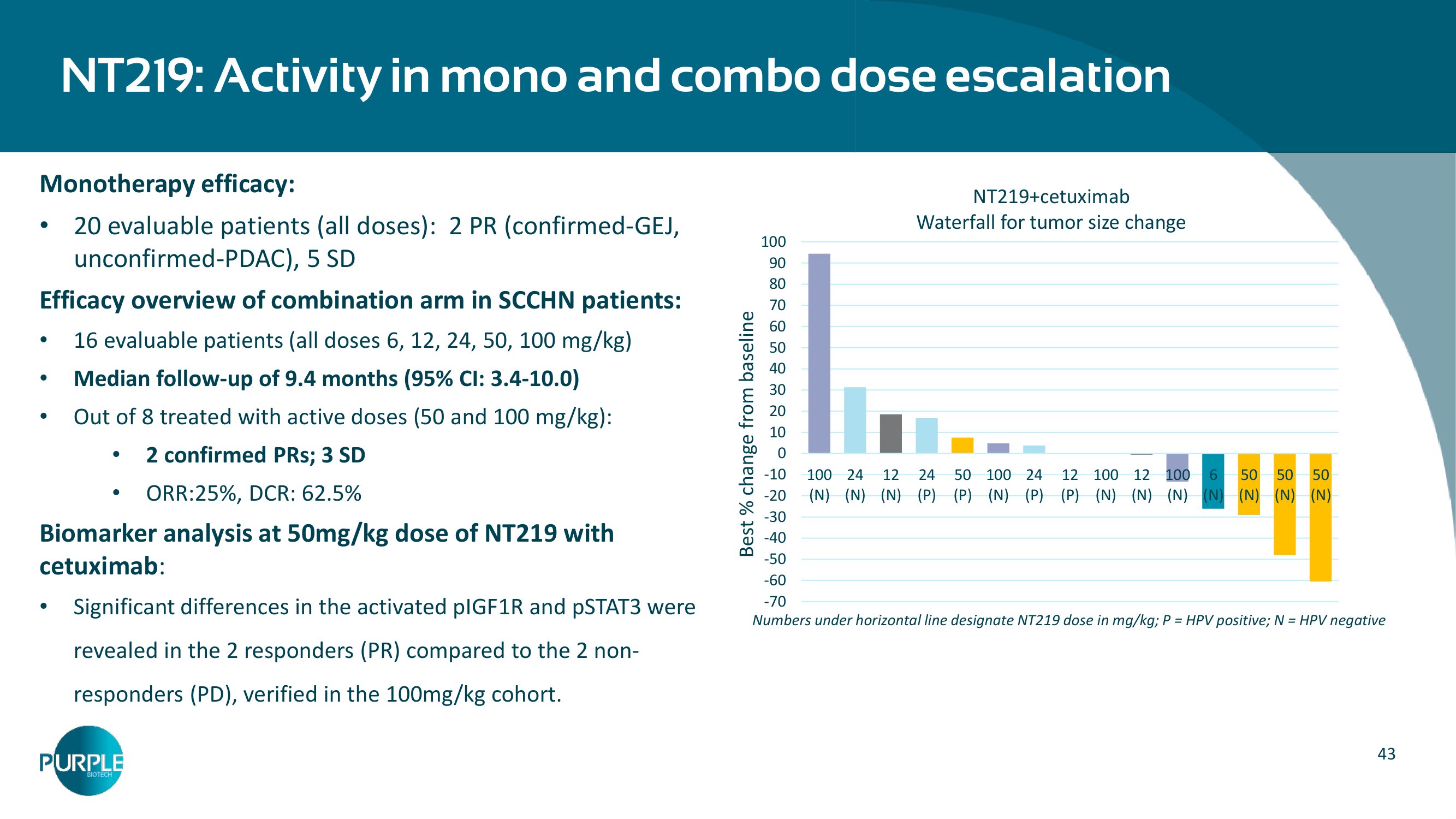
43 Monotherapy efficacy: • 20 evaluable patients (all doses): 2 PR (confirmed - GEJ, unconfirmed - PDAC), 5 SD Efficacy overview of combination arm in SCCHN patients: • 16 evaluable patients (all doses 6 , 12 , 24 , 50 , 100 mg/kg ) • Median follow - up of 9.4 months ( 95 % CI: 3.4 - 10.0 ) • Out of 8 treated with active doses ( 50 and 100 mg/kg): • 2 confirmed PRs; 3 SD • ORR: 25 %, DCR: 62.5 % Biomarker analysis at 50 mg/kg dose of NT 219 with cetuximab : • Significant differences in the activated pIGF 1 R and pSTAT 3 were revealed in the 2 responders (PR) compared to the 2 non - responders (PD), verified in the 100 mg/kg cohort. NT 219 : Activity in mono and combo dose escalation Numbers under horizontal line designate NT 219 dose in mg/kg; P = HPV positive; N = HPV negative -70 -60 -50 -40 -30 -20 -10 0 10 20 30 40 50 60 70 80 90 100 100 (N) 24 (N) 12 (N) 24 (P) 50 (P) 100 (N) 24 (P) 12 (P) 100 (N) 12 (N) 100 (N) 6 (N) 50 (N) 50 (N) 50 (N) Best % change from baseline NT 219 +cetuximab Waterfall for tumor size change
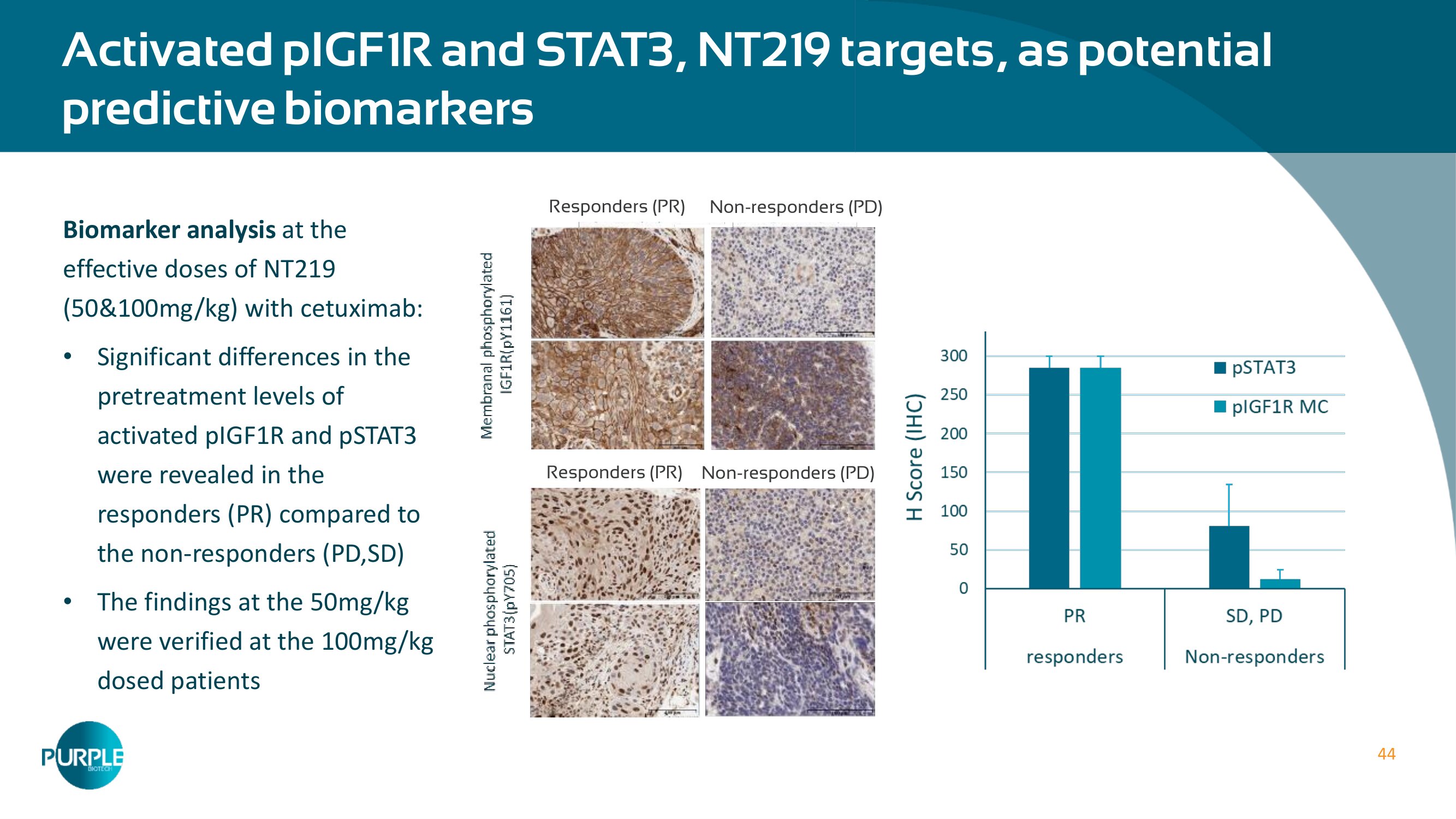
44 Activated pIGF 1 R and STAT 3 , NT 219 targets, as potential predictive biomarkers Biomarker analysis at the effective doses of NT 219 ( 50 & 100 mg/kg) with cetuximab: • Significant differences in the pretreatment levels of activated pIGF 1 R and pSTAT 3 were revealed in the responders (PR) compared to the non - responders (PD,SD) • The findings at the 50 mg/kg were verified at the 100 mg/kg dosed patients Responders (PR) Non - responders (PD) Responders (PR) Non - responders (PD)
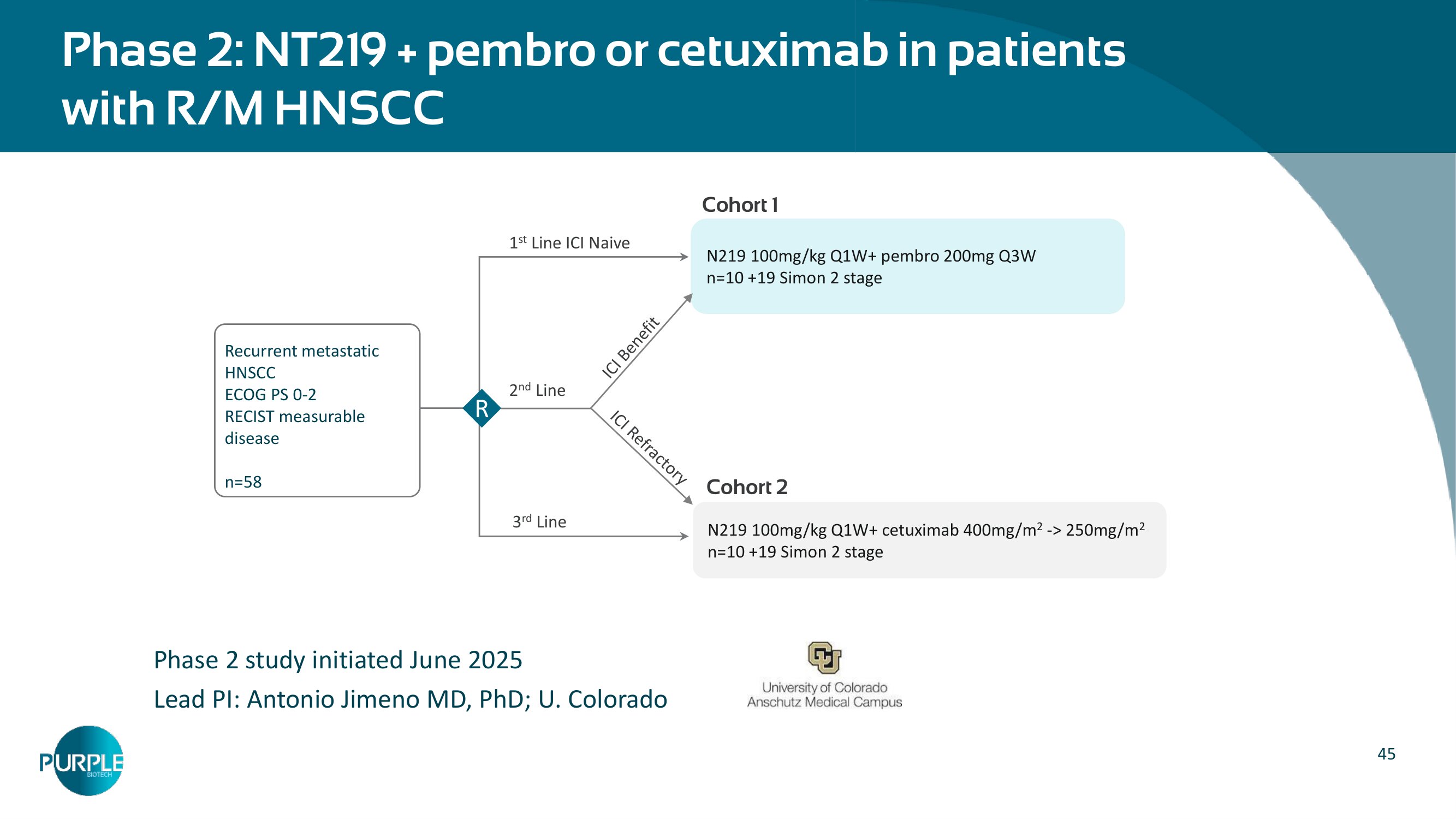
45 Phase 2 : NT 219 + pembro or cetuximab in patients with R/M HNSCC – Phase 2 study initiated June 2025 Lead PI: Antonio Jimeno MD, PhD; U. Colorado Recurrent metastatic HNSCC ECOG PS 0 - 2 RECIST measurable disease n= 58 N 219 100 mg/kg Q 1 W+ pembro 200 mg Q 3 W n= 10 + 19 Simon 2 stage N 219 100 mg/kg Q 1 W+ cetuximab 400 mg/m 2 - > 250 mg/m 2 n= 10 + 19 Simon 2 stage R 1 st Line ICI Naive 2 nd Line 3 rd Line Cohort 1 Cohort 2