Exhibit 99.1
VS - 7375 : Potential Best - in - Class KRAS G12D (ON/OFF) Inhibitor R&D Update Call June 23, 2026
2 FORWARD - LOOKING STATEMENTS This presentation includes forward - looking statements about, among other things, Verastem Oncology’s (the “Company”) programs an d product candidates, strategy, future plans and prospects, including statements related to the approval and commercialization of AVMAPKI® FAKZYNJA® CO - PACK ( avutometinib capsules; defactinib tablets) as a treatment for adult patients with Kirsten rat sarcoma viral oncogene homolog (KRAS) mutant - type (mt) recurrent Lo w - Grade Serous Ovarian Cancer (LGSOC), the expected outcome and benefits of collaborations, including with GenFleet Therapeutics (Shanghai), Inc. ( GenFleet ), including the conduct of a Phase 1/2a study and subsequent studies with respect to VS - 7375, the potential of the results of the RAMP 301 Phase 3 trial to confirm the results of the RAMP 201 study specific to KRAS mutant patients and to expand the in dic ation for AVMAPKI FAKZYNJA CO - PACK regardless of KRAS mutation status, the structure and potential clinical value of our completed, planned and pending clinical trials, the potential clinical value of various of the Company's clinical trials, inc lud ing the RAMP 201, RAMP 201J, RAMP 205, RAMP 301 and VS - 7375 trials, the timing of commencing and completing trials, including topline data reports, our interactions with regulators, the timeline and indications for clinical development, regu lat ory submissions and the potential for and timing of commercialization of our product candidates and potential for additional development programs involving the Company’s lead compound and the potential market opportunities thereof; and the estimated add ressable markets for, and anticipated market opportunities of our drug candidates. The words "anticipate," "believe," "estimate," "expect," "may," "plan," "target," "potential," "would," "could," "should," "continue," "potential," “can” and si mil ar expressions are intended to identify forward - looking statements, although not all forward - looking statements contain these identifying words. Each forward - looking statement is subject to risks and uncertainties that could cause actual results to diffe r materially from those expressed or implied in such statement. Forward - looking statements are subject to a number of risks and uncertainties including, but not limited to: the assumptions und erlying the forward - looking statements; risks related to the development and successful commercialization of our product candidates; obtaining and maintaining regulatory approvals, including, but not limited to, potential regulatory delays or rej ect ions; the challenges with the commercialization of a new product; our history of operating losses and the possibility that we may never achieve or maintain profitability; risks associated with meeting the objectives of Verastem's clinical trials, incl udi ng, but not limited to Verastem's ability to achieve enrollment objectives concerning patient numbers (including an adequate saf ety database), outcomes objectives and/or timing objectives for Verastem's trials; any delays or failures enrollment and the occu rre nce of adverse safety events; our ability to successfully commercialize AVMAPKI FAKZYNJA CO - PACK in the U.S. including our ability to generate market demand for and acceptance of AVMAPKI FAKZYNJA CO - PACK; the potential inability to raise sufficient ca pital to fund ongoing operations as currently planned or to obtain financing on acceptable terms or to fund operations from revenues generated by the sales of AVMAPKI FAKZYNJA CO - PACK; actions or advice of regulatory agencies to maintain regulator y approval of AVMAPKI FAKZYNJA CO - PACK; the impact of current and future healthcare reforms, including those affecting the delivery of or payment for healthcare products and services; uncertainties related to the activities and initia tiv es of the current U.S. presidential administration, including regulatory and policy changes that may adversely affect our bus ine ss; risks related to our ability to obtain, maintain and enforce patent and other intellectual property protection for our product candidates; dec isi ons by regulatory authorities regarding trial design, labeling and other matters that could affect the timing, availability or commercial potential of our product candidates; whether preclinical testing of our product candidates and pre lim inary or interim data from clinical trials will be predictive of the results or success of ongoing or later clinical trials; tha t the timing, scope and rate of reimbursement for our product candidates is uncertain; that the market opportunities of our drug ca ndi dates are based on internal and third - party estimates which may prove to be incorrect; that third - party payors (including government agencies) may not reimburse; that there may be competitive developments affecting our product candidates; that dat a m ay not be available when expected; that enrollment of clinical trials may take longer than expected; the risks that we will not satisfy our post - marketing requirements and commitments established and agreed to as part of the FDA's approval of AVMAPKI F AKZYNJA CO - PACK; that our marketed product candidates may cause adverse safety events and/or unexpected concerns may arise from additional data or analysis, or result in unmanageable safety profiles as compared to their levels of ef ficacy; that we may not be able to confirm the results from the RAMP 201 study or expand the approved indication for AVMAPKI FAKZYNJA CO - PACK; that our product candidates may experience manufacturing or supply interruptions or failures; that any of our third - party contract research organizations, contract manufacturing organizations, clinical sites, or contractors, among others, which we rely on may fail to fully perform; that we face substantial competition, which may result in others developi ng or commercializing products before or more successfully than we do which could result in reduced market share or market potential for our product candidates; that we may be unable to successfully initiate or complete the clinical development and ev entual commercialization of our product candidates; that the development and commercialization of our product candidates may take longer or cost more than planned, including as a result of conducting additional studies or our decisions regarding exe cution of such commercialization; that we may not attract and retain high quality personnel; that we or Pfizer, Inc. may fail to fully perform under the license agreement covering certain Pfizer FAK inhibitors, including defactinib ; that we or Chugai Pharmaceutical Co., Ltd. may fail to fully perform under the avutometinib license agreement; that we or GenFleet may fail to fully perform under the collaboration and option agreement covering VS - 7375 and other assets we may decide to option in; that our tota l addressable and target markets for our product candidates might be smaller than we are presently estimating; that we or Secura Bio, Inc. may fail to fully perform under the asset purchase agreement with Secura Bio, Inc., including in relation to milestone payments; that we may not be able to establish new or expand on existing collaborations or partnerships, including with respect to in - licensing of our product candidates, on favorable terms, or at all; that we may be unable to obtain adequate financing in the future through product licensing, co - promotional arrangements, public or private equity, debt financing or otherwise; that we may not pursue or submit regulatory filings for our product candidates; that, due to the current president ial administration's significant reduction in the FDA's workforce and potential reductions to the FDA's budget, we may experience a material impact to the FDA's ability to engage in a variety of activities that may affect our business, includin g r outine regulatory and oversight activities; and that our product candidates may not receive regulatory approval, become commercially successful products, or result in new treatment options being offered to patients. Other risks and uncertainties include those identified under the heading “Risk Factors” in the Company’s Annual Report on For m 1 0 - K for the year ended December 31, 2025, as filed with the Securities and Exchange Commission (SEC) on March 04, 2026, and in any subsequent filings with the SEC, which are available at www.sec.govand www.verastem.com.The forward - looking sta tements in this presentation speak only as of the original date of this presentation, and we undertake no obligation to update or revise any of these statements whether as a result of new information, future events or otherwise, except as requir ed by law. Our business is subject to substantial risks and uncertainties, including those referenced above. Investors, potentia l investors, and others should give careful consideration to these risks and uncertainties. USE OF NON - GAAP FINANCIAL MEASURES This presentation contains references to our non - GAAP operating expense, a financial measure that is not calculated in accordanc e with generally accepted accounting principles in the US (GAAP). This non - GAAP financial measure excludes certain amounts or expenses from the corresponding financial measures determined in accordance with GAAP. Management believes this non - GAAP information is useful for investors, taken in conjunction with the Company’s GAAP financial statements, because it provides greater transparency and period - over - period comparability with respect to the Company’s operating performanc e and can enhance investors’ ability to identify operating trends in the Company’s business. Management uses this measure, among other factors, to assess and analyze operational results and trends and to make financial and operational deci sio ns. Non - GAAP information is not prepared under a comprehensive set of accounting rules and should only be used to supplement an understanding of the Company’s operating results as reported under GAAP, not in isolation or as a substitute fo r, or superior to, financial information prepared and presented in accordance with GAAP. In addition, this non - GAAP financial measure is unlikely to be comparable with non - GAAP information provided by other companies. The determination of the amounts tha t are excluded from non - GAAP financial measures is a matter of management judgment and depends upon, among other factors, the nature of the underlying expense or income amounts. Reconciliations between this non - GAAP financial measure a nd the most comparable GAAP financial measure are included in the footnotes to the slides in this presentation on which such non - GAAP number appears. THIRD - PARTY SOURCES Certain information contained in this presentation, including industry and market data and other statistical information, rel ate s to or is based on studies, publications, surveys and other data obtained from third - party sources and the Company’s own internal estimates and research. While the Company believes these third - party sources to be reliable as of the date of this pres entation, it has not independently verified, and makes no representation as to the adequacy, fairness, accuracy or completeness of, any information obtained from third - party sources. In addition, all of the market data included in this present ation involves a number of assumptions and limitations, and there can be no guarantee as to the accuracy or reliability of such assumptions. Disclaimers

3 3 Agenda and Conference Call Participants JULISSA VIANA SVP, Corporate Communications, Investor Relations and Patient Advocacy Introduction DAN PATERSON President and Chief Executive Officer Opening Remarks MICHAEL KAUFFMAN, MD, PHD President, Development VS - 7375 Clinical Update JON PACHTER, PHD Chief Scientific Officer Rationale for New Clinical Collaborations with VS - 7375 DAN PATERSON & EXECUTIVE TEAM Closing Remarks & Q&A

Dan Paterson President & CEO Opening Remarks
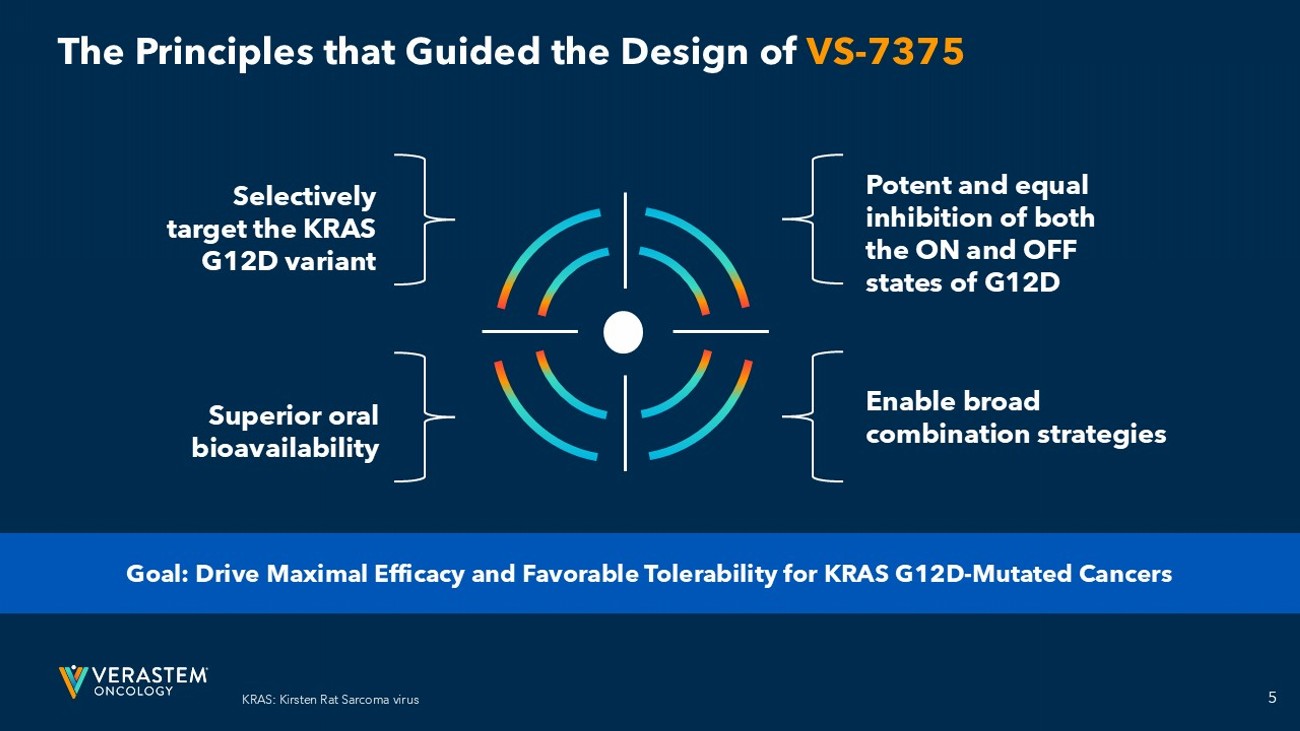
5 The Principles that Guided the Design of VS - 7375 Potent and equal inhibition of both the ON and OFF states of G12D Enable broad combination strategies Selectively target the KRAS G12D variant Superior oral bioavailability Goal: Drive Maximal Efficacy and Favorable Tolerability for KRAS G12D - Mutated Cancers KRAS: Kirsten Rat Sarcoma virus
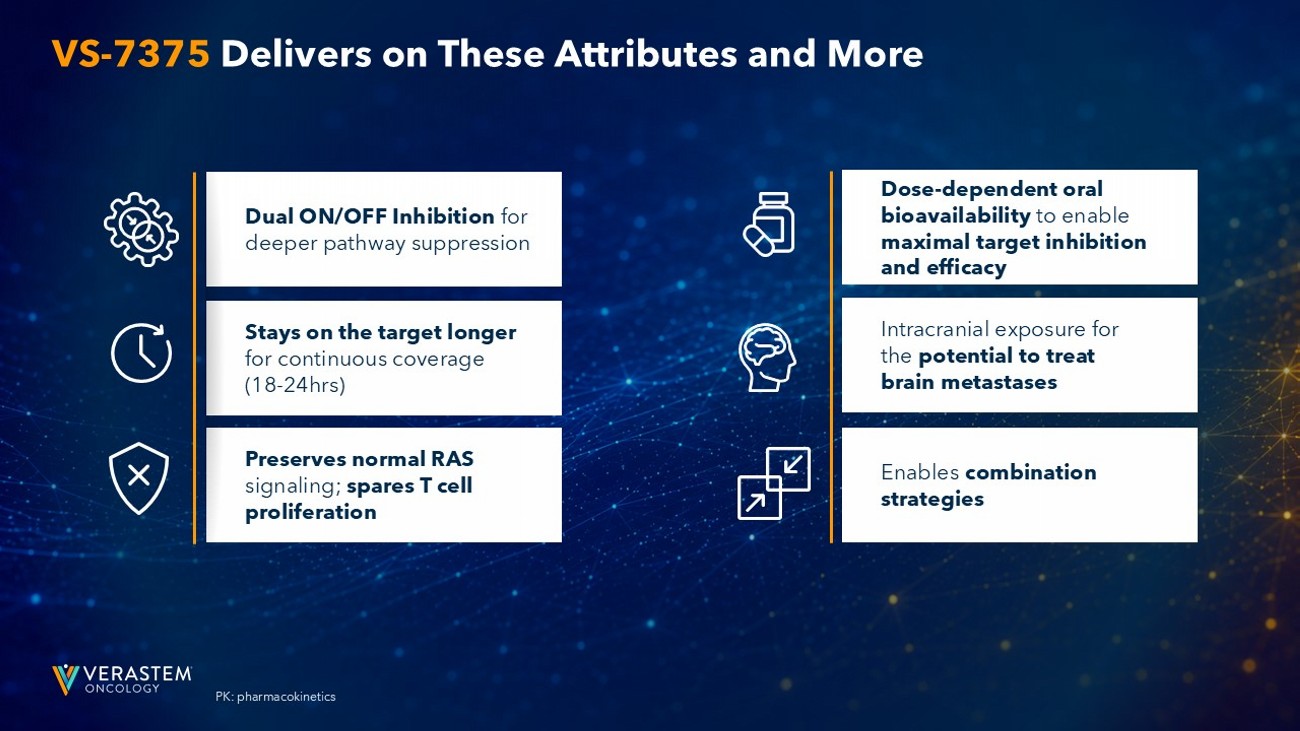
6 PK: pharmacokinetics VS - 7375 Delivers on These Attributes and More Dose - dependent oral bioavailability to enable maximal target inhibition and efficacy Enables combination strategies Intracranial exposure for the potential to treat brain metastases Stays on the target longer for continuous coverage (18 - 24hrs) Dual ON/OFF Inhibition for deeper pathway suppression Preserves normal RAS signaling; spares T cell proliferation
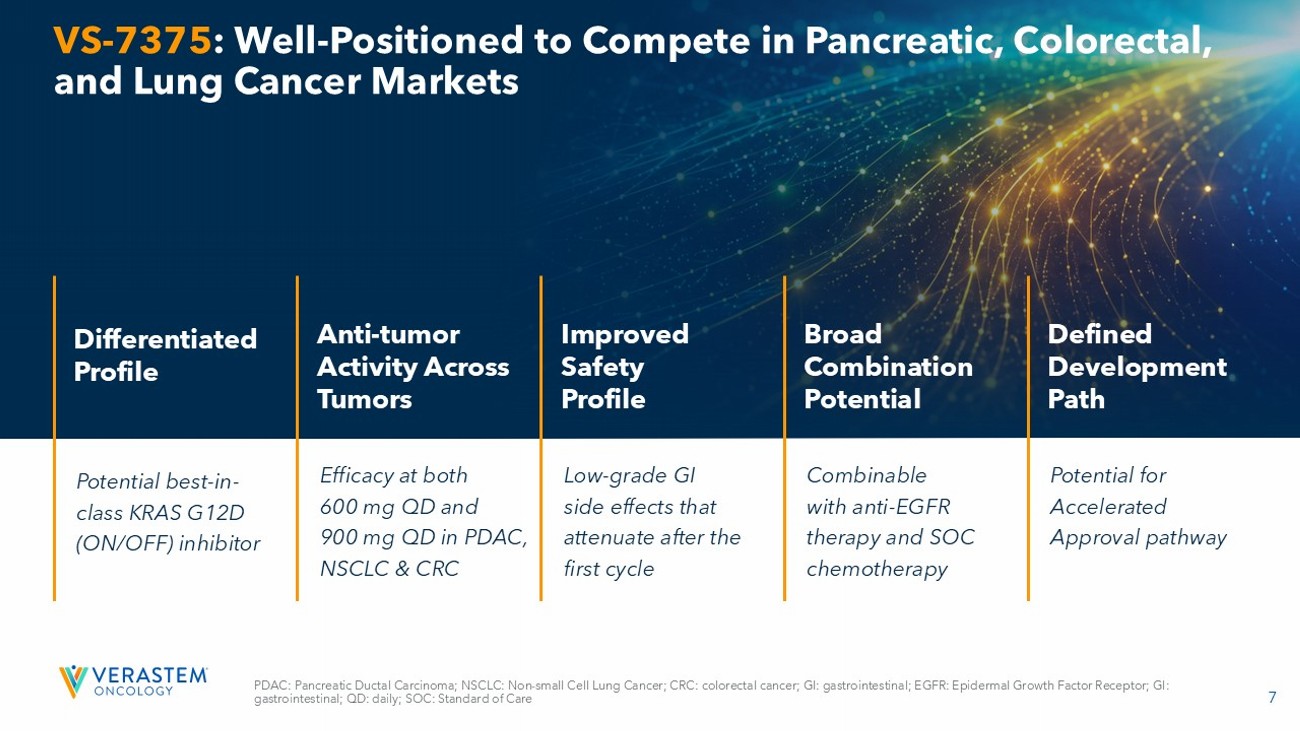
7 VS - 7375 : Well - Positioned to Compete in Pancreatic, Colorectal, and Lung Cancer Markets Potential b est - in - class KRAS G12D (ON/OFF) inhibitor Differentiated Profile Efficacy at both 600 mg QD and 900 mg QD in PDAC, NSCLC & CRC Anti - tumor Activity Across Tumors Low - grade GI side effects that attenuate after the first cycle Improved Safety Profile Combinable with anti - EGFR therapy and SOC chemotherapy Broad Combination Potential Potential for Accelerated Approval pathway Defined Development Path PDAC: Pancreatic Ductal Carcinoma; NSCLC: Non - small Cell Lung Cancer; CRC: colorectal cancer; GI: gastrointestinal; EGFR: Epider mal Growth Factor Receptor; GI: gastrointestinal; QD: daily; SOC: Standard of Care
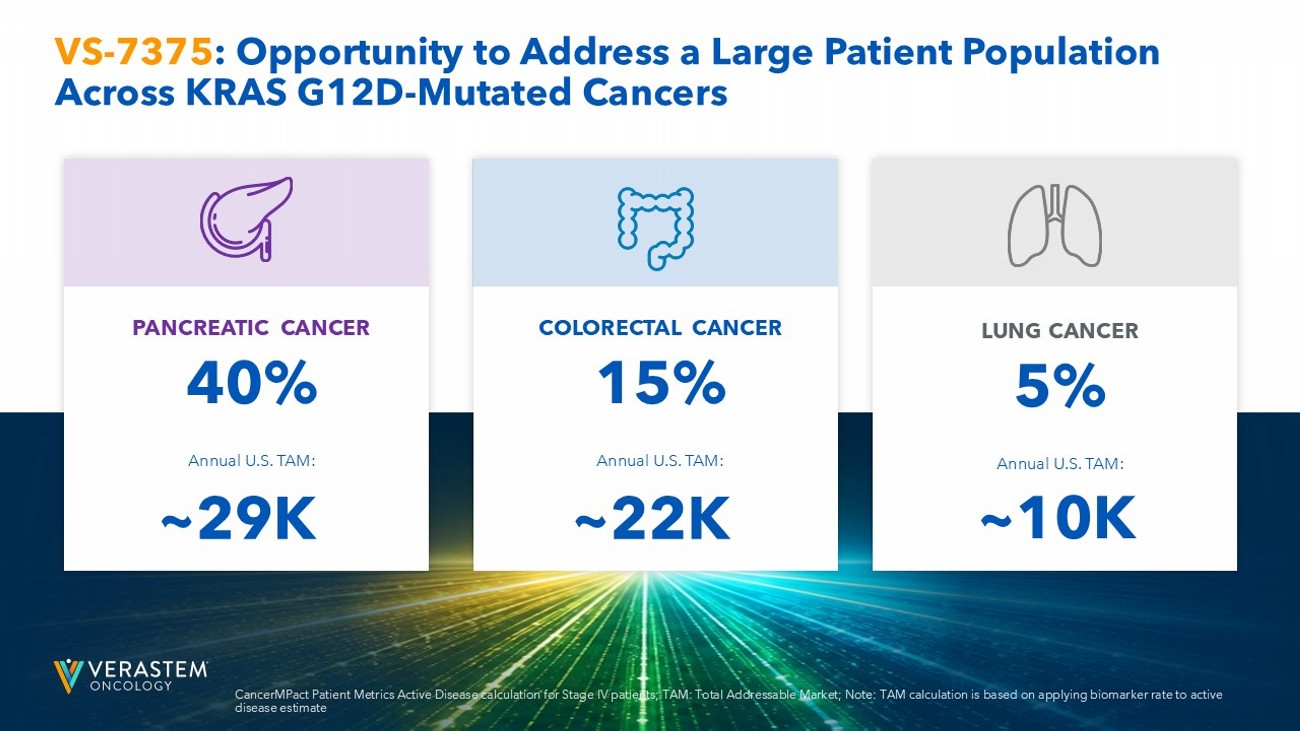
8 PANCREATIC CANCER 40% Annual U.S. TAM: COLORECTAL CANCER 15% Annual U.S. TAM: LUNG CANCER 5% Annual U.S. TAM: VS - 7375 : Opportunity to Address a Large Patient Population Across KRAS G12D - Mutated Cancers ~29K ~22K ~10K CancerMPact Patient Metrics Active Disease calculation for Stage IV patients; TAM: Total Addressable Market; Note: TAM calculation is bas ed on applying biomarker rate to active disease estimate

VS - 7375 Clinical Update Michael Kauffman, MD, PhD President, Development
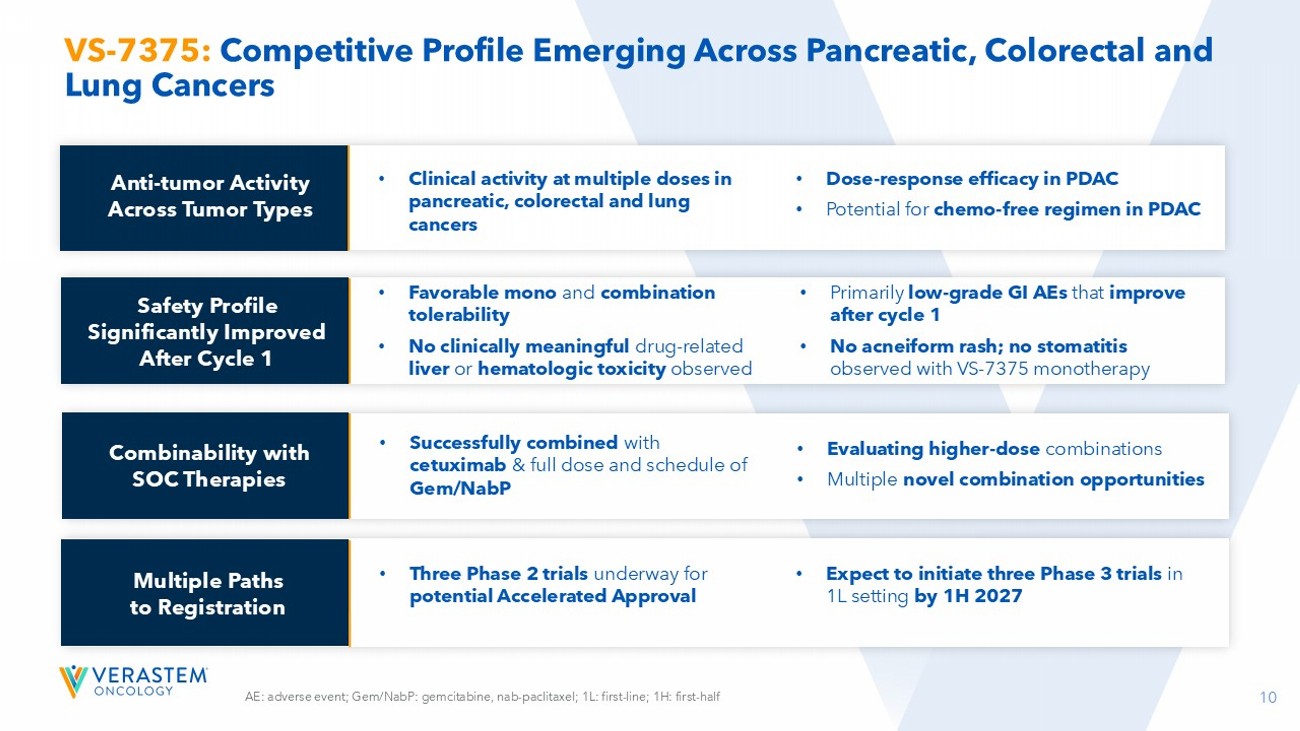
10 VS - 7375: Competitive Profile Emerging Across Pancreatic, Colorectal and Lung Cancers AE: adverse event; Gem/NabP: gemcitabine, nab - paclitaxel; 1L: first - line; 1H: first - half Safety Profile Significantly Improved After Cycle 1 Combinability with SOC Therapies Multiple Paths to Registration • Clinical activity at multiple doses in pancreatic, colorectal and lung cancers • Dose - response efficacy in PDAC • Potential for chemo - free regimen in PDAC • Favorable mono and combination tolerability • No clinically meaningful drug - related liver or hematologic toxicity observed • Primarily low - grade GI AEs that improve after cycle 1 • No acneiform rash; no stomatitis observed with VS - 7375 monotherapy • Successfully combined with cetuximab & full dose and schedule of Gem/NabP • Evaluating higher - dose combinations • Multiple novel combination opportunities • Three Phase 2 trials underway for potential Accelerated Approval • Expect to initiate three Phase 3 trials in 1L setting by 1H 2027 Anti - tumor Activity Across Tumor Types
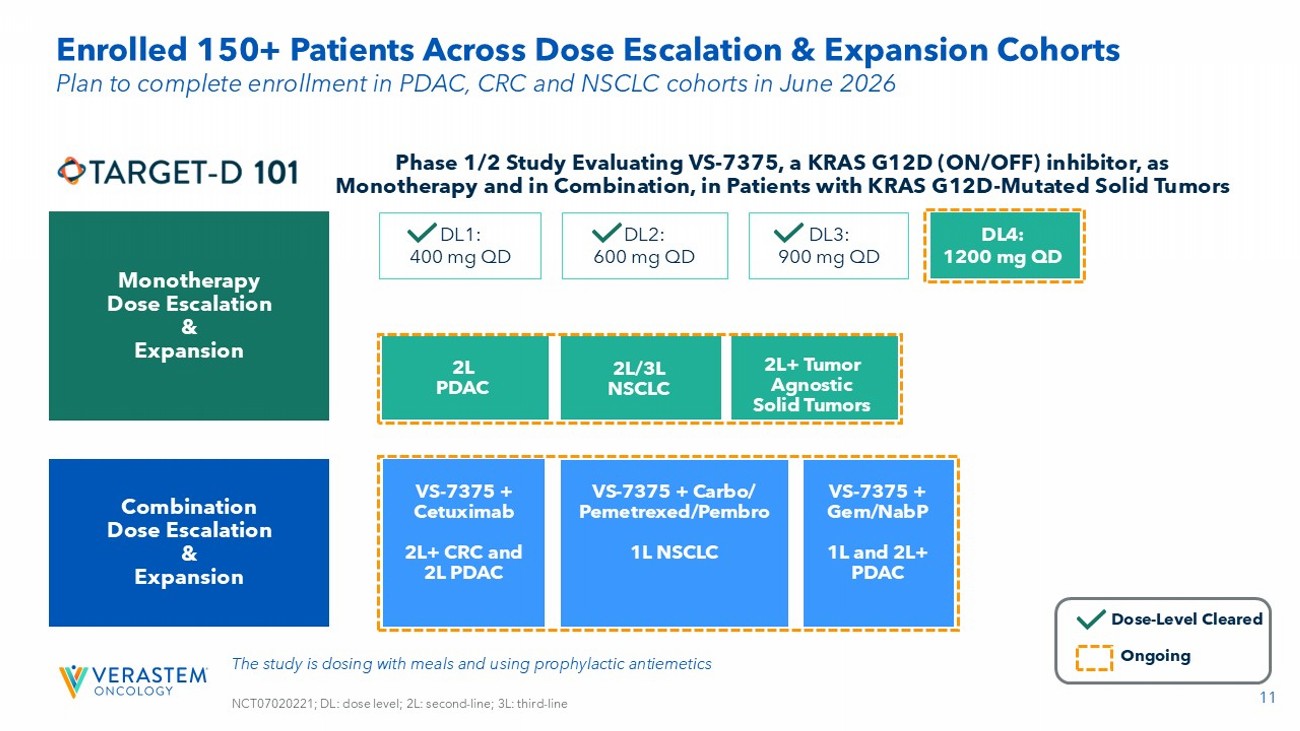
11 Enrolled 150+ Patients Across Dose Escalation & Expansion Cohorts Phase 1/2 Study Evaluating VS - 7375, a KRAS G12D (ON/OFF) inhibitor, as Monotherapy and in Combination, in Patients with KRAS G12D - Mutated Solid Tumors The study is dosing with meals and using prophylactic antiemetics NCT07020221; DL: dose level; 2L: second - line; 3L: third - line Monotherapy Dose Escalation & Expansion DL2: 600 mg QD DL3: 900 mg QD DL1: 400 mg QD 2L+ Tumor Agnostic Solid Tumors 2L/3L NSCLC 2L PDAC DL4: 1200 mg QD Combination Dose Escalation & Expansion VS - 7375 + Cetuximab 2L+ CRC and 2L PDAC VS - 7375 + Carbo/ Pemetrexed/ Pembro 1L NSCLC VS - 7375 + Gem/ NabP 1L and 2L+ PDAC Dose - Level Cleared Ongoing Plan to complete enrollment in PDAC, CRC and NSCLC cohorts in June 2026
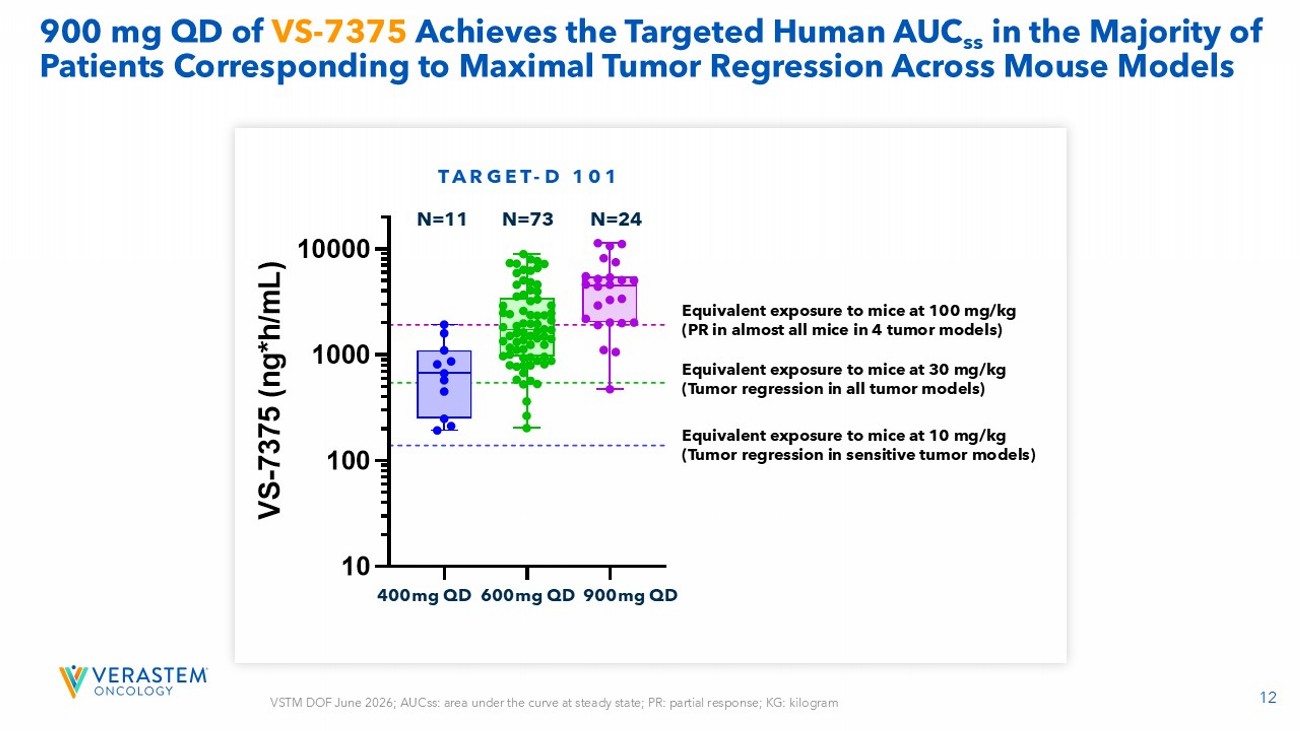
12 900 mg QD of VS - 7375 Achieves the Targeted Human AUC ss in the Majority of Patients Corresponding to Maximal Tumor Regression Across Mouse Models 400mg QD 600mg QD 900mg QD Equivalent exposure to mice at 100 mg/kg (PR in almost all mice in 4 tumor models) Equivalent exposure to mice at 10 mg/kg (Tumor regression in sensitive tumor models) Equivalent exposure to mice at 30 mg/kg (Tumor regression in all tumor models) VSTM DOF June 2026; AUCss : area under the curve at steady state; PR: partial response; KG: kilogram TARGET - D 101 N=11 N=73 N=24 4 0 0 m g Q D 6 0 0 m g Q D 9 0 0 m g Q D 10 100 1000 10000 TARGET-D 101 V S - 7 3 7 5 ( n g * h / m L ) N=11 N=73 N=24
13 mPDAC: VS - 7375 900 mg Demonstrates Promising Preliminary Efficacy; Deeper and More Rapid Responses Seen with Cetuximab Combination KEY OBSERVATIONS: METASTATIC PANCREATIC DUCTAL CARCINOMA 2 - 4L mPDAC Towards 1L mPDAC As of June 2026: 7 of 20+ patients at the 600 mg dose with ≥6 months of follow up 1 of 20+ patients at the 900 mg dose with ≥6 months of follow up Enrolling additional patients in the 600 mg QD plus full dose of Gem/NabP cohort Expect to complete enrollment of 20+ patients at both dose levels in June 2026 ENROLLMENT STATUS: • Evidence of dose - dependent anti - tumor activity observed between 600 and 900 mg QD • Promising preliminary efficacy observed at 900 mg monotherapy • 900 mg QD looks extremely compelling with marked CA19 - 9 reduction in almost all patients • Preliminary anti - EGFR combination demonstrates deeper and more rapid responses even at subtherapeutic doses • Good combinability with SOC Gem/NabP in 2L+ • DLT - cleared VS - 7375 600 mg QD plus full dose of Gem/NabP in 2L+ • Dose - escalation continues with 900 mg QD plus full dose of Gem/NabP in 2L+ • 1L combo data with Gem/NabP expected in 2H 2026 As of June 2026. mPDAC: metastatic pancreatic ductal carcinoma; CA19 - 9: Cancer antigen 19 - 9; DLT: dose - limiting toxicity; 2H: se cond half
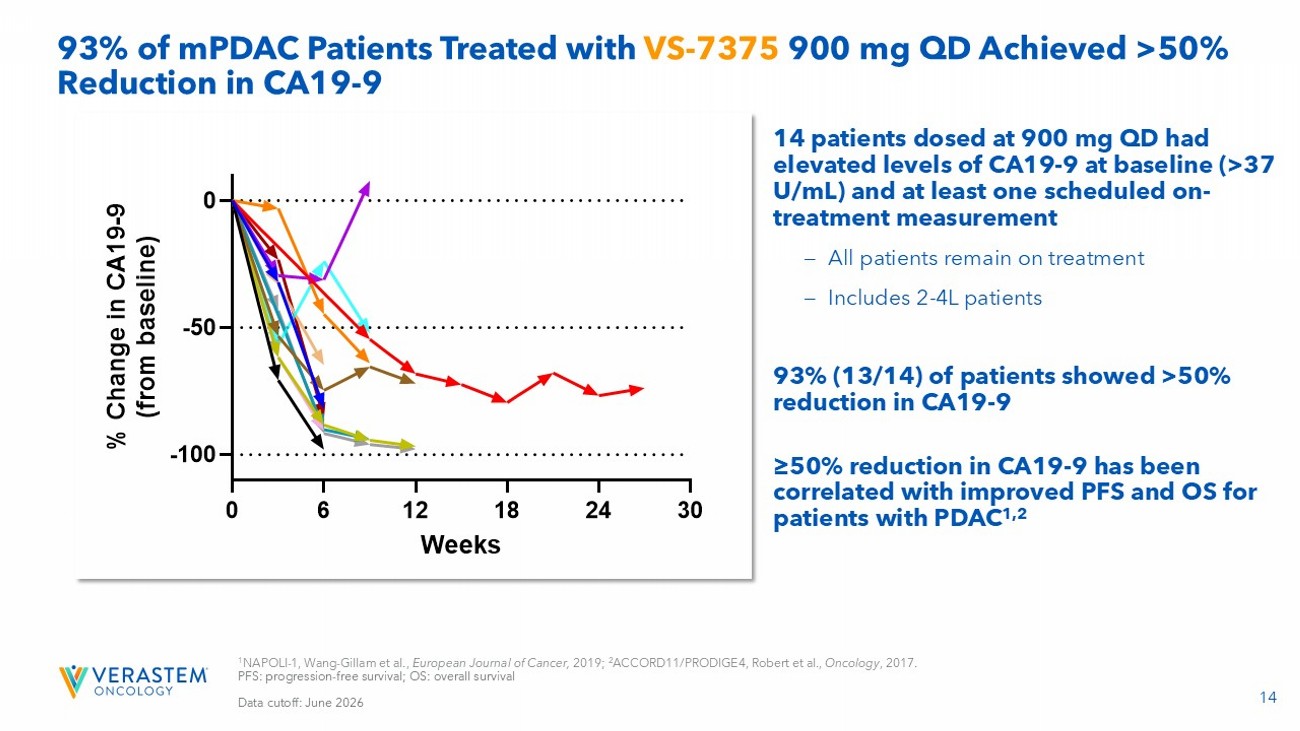
14 14 patients dosed at 900 mg QD had elevated levels of CA19 - 9 at baseline (>37 U/mL) and at least one scheduled on - treatment measurement – All patients remain on treatment – Includes 2 - 4L patients 93% (13/14) of patients showed >50% reduction in CA19 - 9 ≥50% reduction in CA19 - 9 has been correlated with improved PFS and OS for patients with PDAC 1,2 93% of mPDAC Patients Treated with VS - 7375 900 mg QD Achieved >50% Reduction in CA19 - 9 1 NAPOLI - 1, Wang - Gillam et al., European Journal of Cancer, 2019; 2 ACCORD11/PRODIGE4, Robert et al., Oncology , 2017. PFS: progression - free survival; OS: overall survival Data cutoff: June 2026 0 6 12 18 24 30 -100 -50 0 Weeks % C h a n g e i n C A 1 9 - 9 ( f r o m b a s e l i n e ) 0101-020 0102-004 0103-007 0104-012 0104-016 0105-021 0105-023 0105-026 0106-016 0110-007 0112-016 0116-003 0116-005 0116-008 On Treatment
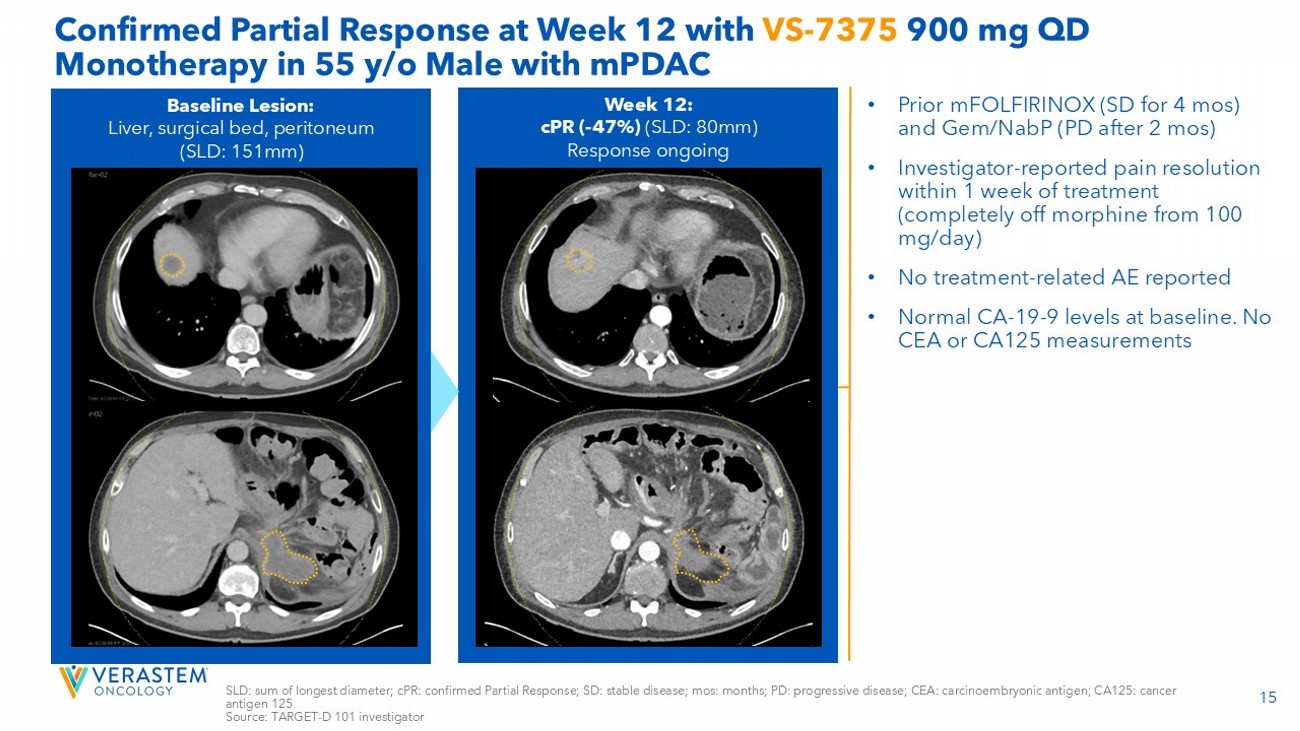
15 Confirmed Partial Response at Week 12 with VS - 7375 900 mg QD Monotherapy in 55 y/o Male with mPDAC • Prior mFOLFIRINOX (SD for 4 mos ) and Gem/NabP (PD after 2 mos ) • Investigator - reported pain resolution within 1 week of treatment (completely off morphine from 100 mg/day) • No treatment - related AE reported • Normal CA - 19 - 9 levels at baseline. No CEA or CA125 measurements Week 12: cPR ( - 47%) (SLD: 80mm) Response ongoing Baseline Lesion: Liver, surgical bed, peritoneum (SLD: 151mm) SLD: sum of longest diameter; cPR : confirmed Partial Response; SD: stable disease; mos : months; PD: progressive disease; CEA: carcinoembryonic antigen; CA125: cancer antigen 125 Source: TARGET - D 101 investigator
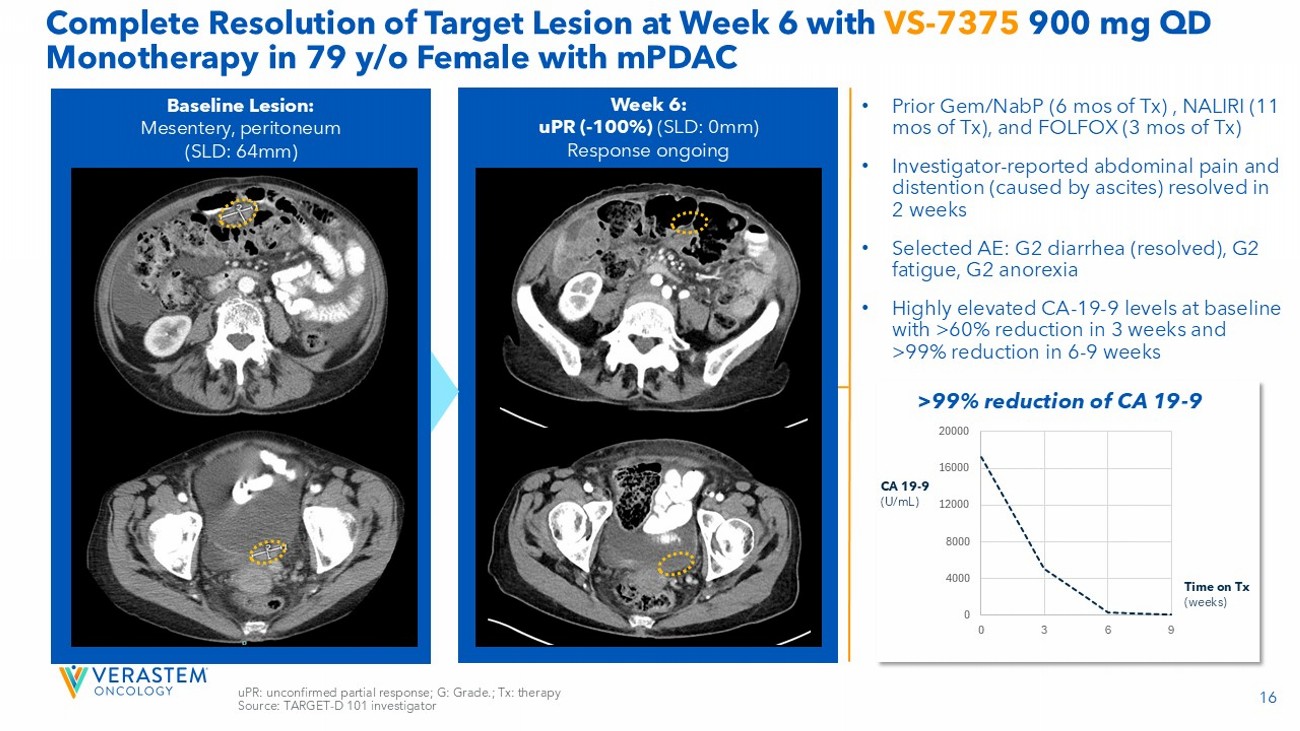
16 Complete Resolution of Target Lesion at Week 6 with VS - 7375 900 mg QD Monotherapy in 79 y/o Female with mPDAC uPR : unconfirmed partial response; G: Grade.; Tx: therapy Source: TARGET - D 101 investigator • Prior Gem/NabP (6 mos of Tx) , NALIRI (11 mos of Tx), and FOLFOX (3 mos of Tx) • Investigator - reported abdominal pain and distention (caused by ascites) resolved in 2 weeks • Selected AE: G2 diarrhea (resolved), G2 fatigue, G2 anorexia • Highly elevated CA - 19 - 9 levels at baseline with >60% reduction in 3 weeks and >99% reduction in 6 - 9 weeks Week 6: uPR ( - 100%) (SLD: 0mm) Response ongoing Baseline Lesion: Mesentery, peritoneum (SLD: 64mm) 0 4000 8000 12000 16000 20000 0 3 6 9 CA 19 - 9 (U/mL) Time on Tx (weeks) >99% reduction of CA 19 - 9
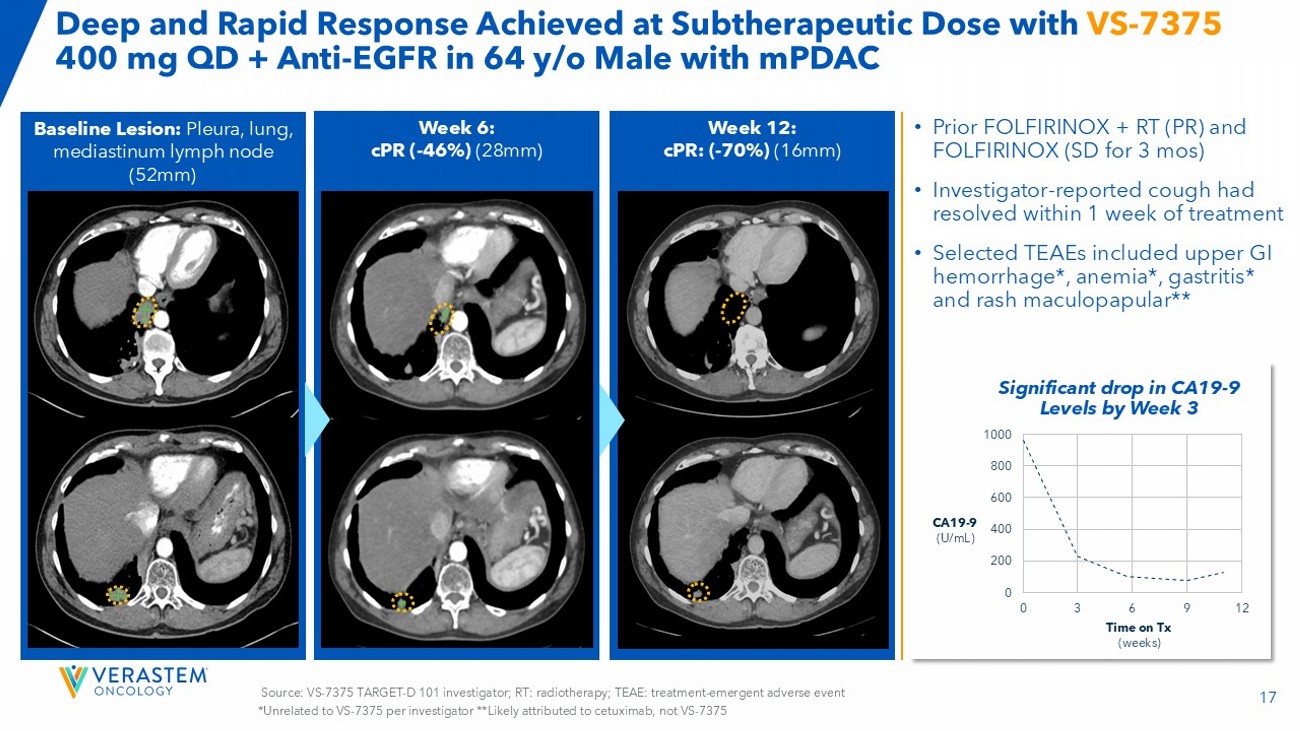
17 Source: VS - 7375 TARGET - D 101 investigator; RT: radiotherapy; TEAE: treatment - emergent adverse event Baseline Lesion: Pleura, lung, mediastinum lymph node (52mm) 7x5mm 9x7mm Week 6: cPR ( - 46%) (28mm) Week 12: cPR : ( - 70%) (16mm) Deep and Rapid Response Achieved at Subtherapeutic Dose with VS - 7375 400 mg QD + Anti - EGFR in 64 y/o Male with mPDAC • Prior FOLFIRINOX + RT (PR) and FOLFIRINOX (SD for 3 mos ) • Investigator - reported cough had resolved within 1 week of treatment • Selected TEAEs included upper GI hemorrhage*, anemia*, gastritis* and rash maculopapular** 0 200 400 600 800 1000 0 3 6 9 12 CA19 - 9 (U/mL) Time on Tx (weeks) Significant drop in CA19 - 9 Levels by Week 3 *Unrelated to VS - 7375 per investigator **Likely attributed to cetuximab, not VS - 7375
18 As of June 2026 mCRC: Preliminary Efficacy Observed with Cetuximab Combination at Both VS - 7375 600 mg QD & 900 mg QD KEY OBSERVATIONS: METASTATIC COLORECTAL CANCER As of June 2026: All patients (20+) at the 600 mg dose in combination with cetuximab have ≤6 months of follow - up 900 mg + full dose cetuximab DLT - cleared in May 2026 ; additional patients to be dosed in TARGET - D 203 Expect to complete enrollment of 20+ patients at the 600 mg dose level + cetuximab in June 2026 ENROLLMENT STATUS: 2L+ CRC • Promising preliminary efficacy observed at 600mg and 900mg QD in combination with anti - EGFR • No overlapping toxicity with cetuximab
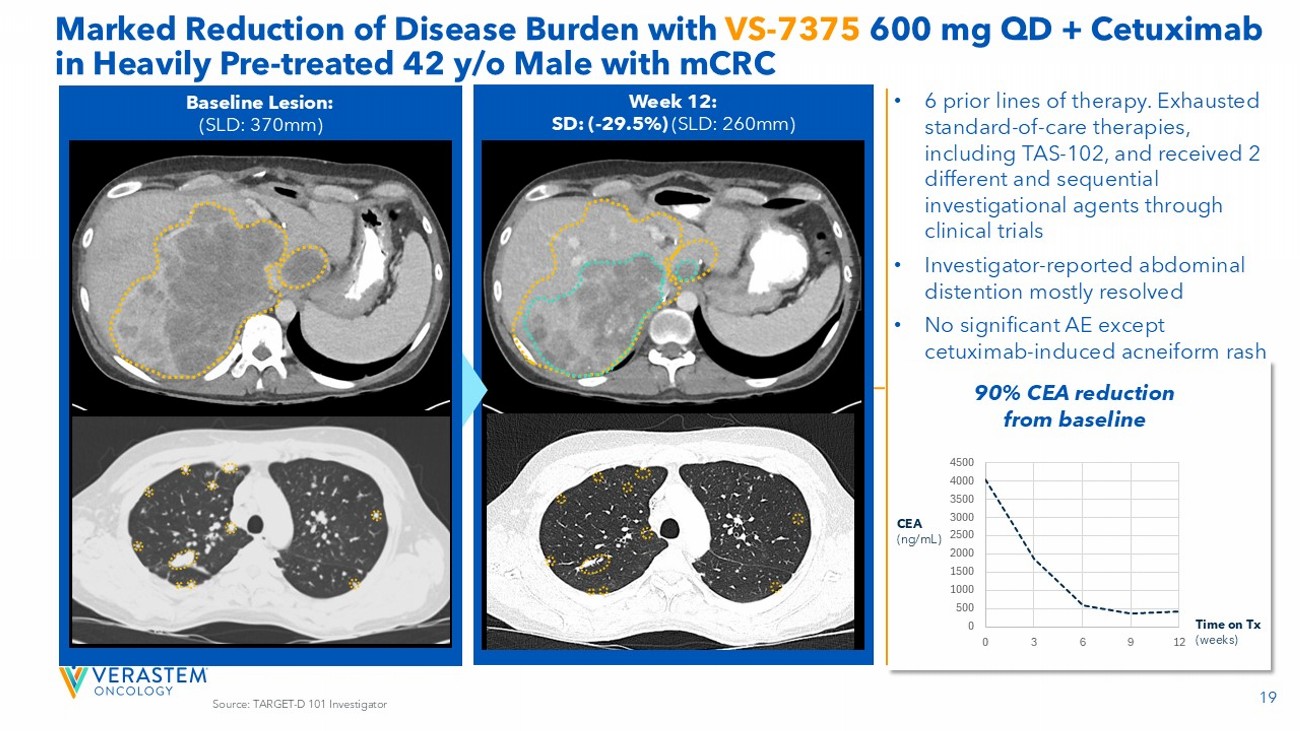
19 Marked Reduction of Disease Burden with VS - 7375 600 mg QD + Cetuximab in Heavily Pre - treated 42 y/o Male with mCRC Source: TARGET - D 101 Investigator Week 12: SD: ( - 29.5%) (SLD: 260mm) Baseline Lesion: (SLD: 370mm) 0 500 1000 1500 2000 2500 3000 3500 4000 4500 0 3 6 9 12 CEA (ng/mL) Time on Tx (weeks) 90% CEA reduction from baseline • 6 prior lines of therapy. Exhausted standard - of - care therapies, including TAS - 102, and received 2 different and sequential investigational agents through clinical trials • Investigator - reported abdominal distention mostly resolved • No significant AE except cetuximab - induced acneiform rash
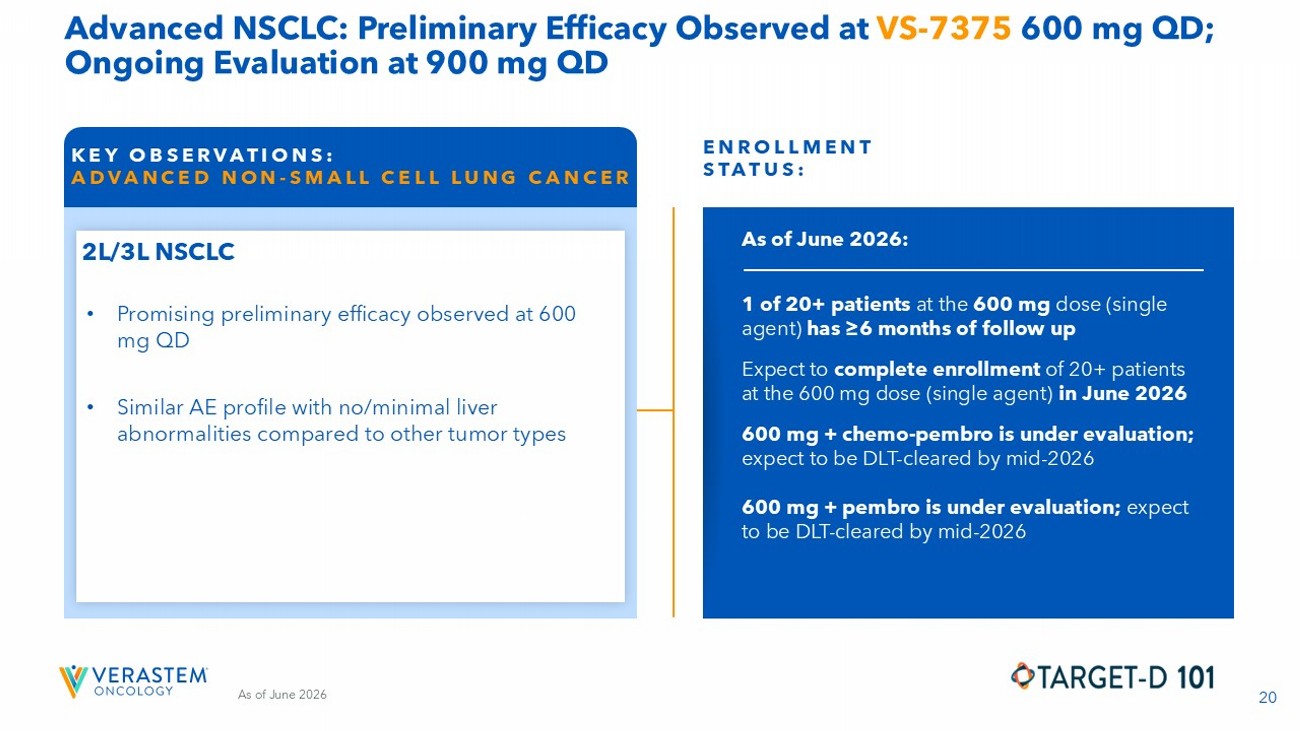
20 As of June 2026 Advanced NSCLC: Preliminary Efficacy Observed at VS - 7375 600 mg QD; Ongoing Evaluation at 900 mg QD KEY OBSERVATIONS: ADVANCED NON - SMALL CELL LUNG CANCER As of June 2026: 1 of 20+ patients at the 600 mg dose (single agent) has ≥6 months of follow up Expect to complete enrollment of 20+ patients at the 600 mg dose (single agent) in June 2026 600 mg + chemo - pembro is under evaluation; expect to be DLT - cleared by mid - 2026 600 mg + pembro is under evaluation; expect to be DLT - cleared by mid - 2026 ENROLLMENT STATUS: 2L/3L NSCLC • Similar AE profile with no/minimal liver abnormalities compared to other tumor types • Promising preliminary efficacy observed at 600 mg QD
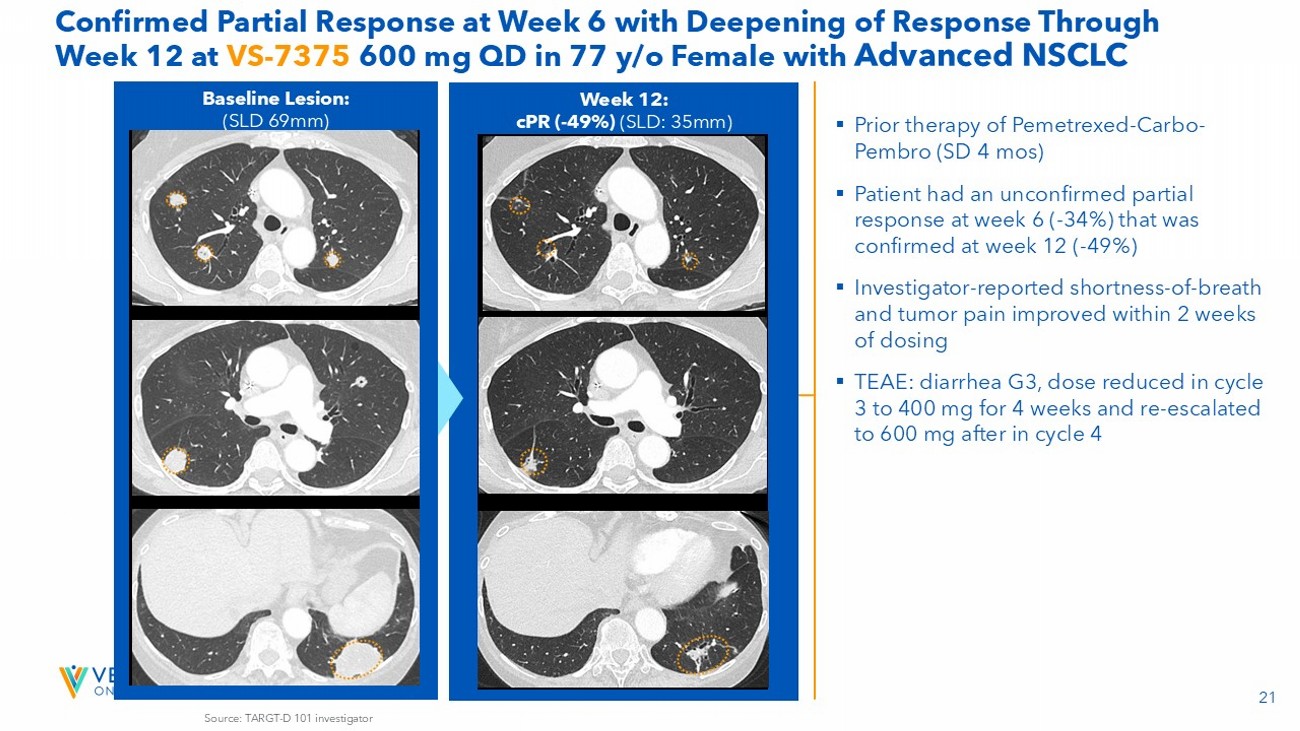
21 Week 12: cPR ( - 49%) (SLD: 35mm) Baseline Lesion: (SLD 69mm) Source: TARGT - D 101 investigator Confirmed Partial Response at Week 6 with Deepening of Response Through Week 12 at VS - 7375 600 mg QD in 77 y/o Female with Advanced NSCLC ▪ Prior therapy of Pemetrexed - Carbo - Pembro (SD 4 mos ) ▪ Patient had an unconfirmed partial response at week 6 ( - 34%) that was confirmed at week 12 ( - 49%) ▪ Investigator - reported shortness - of - breath and tumor pain improved within 2 weeks of dosing ▪ TEAE: diarrhea G3, dose reduced in cycle 3 to 400 mg for 4 weeks and re - escalated to 600 mg after in cycle 4

VS - 7375 Safety Update Michael Kauffman, MD, PhD President, Development
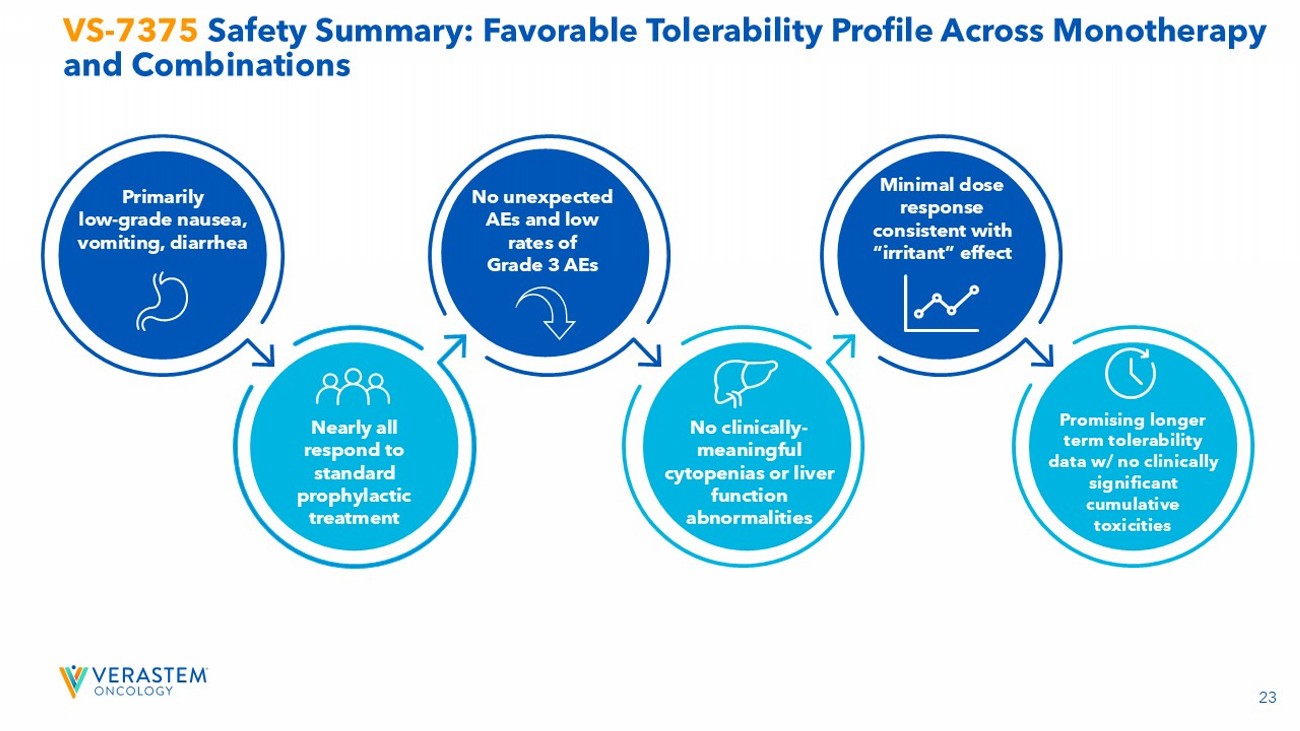
23 VS - 7375 Safety Summary: Favorable Tolerability Profile Across Monotherapy and Combinations Primarily low - grade nausea, vomiting, diarrhea Nearly all respond to standard prophylactic treatment No unexpected AEs and low rates of Grade 3 AEs No clinically - meaningful cytopenias or liver function abnormalities Minimal dose response consistent with “irritant” effect Promising longer term tolerability data w/ no clinically significant cumulative toxicities
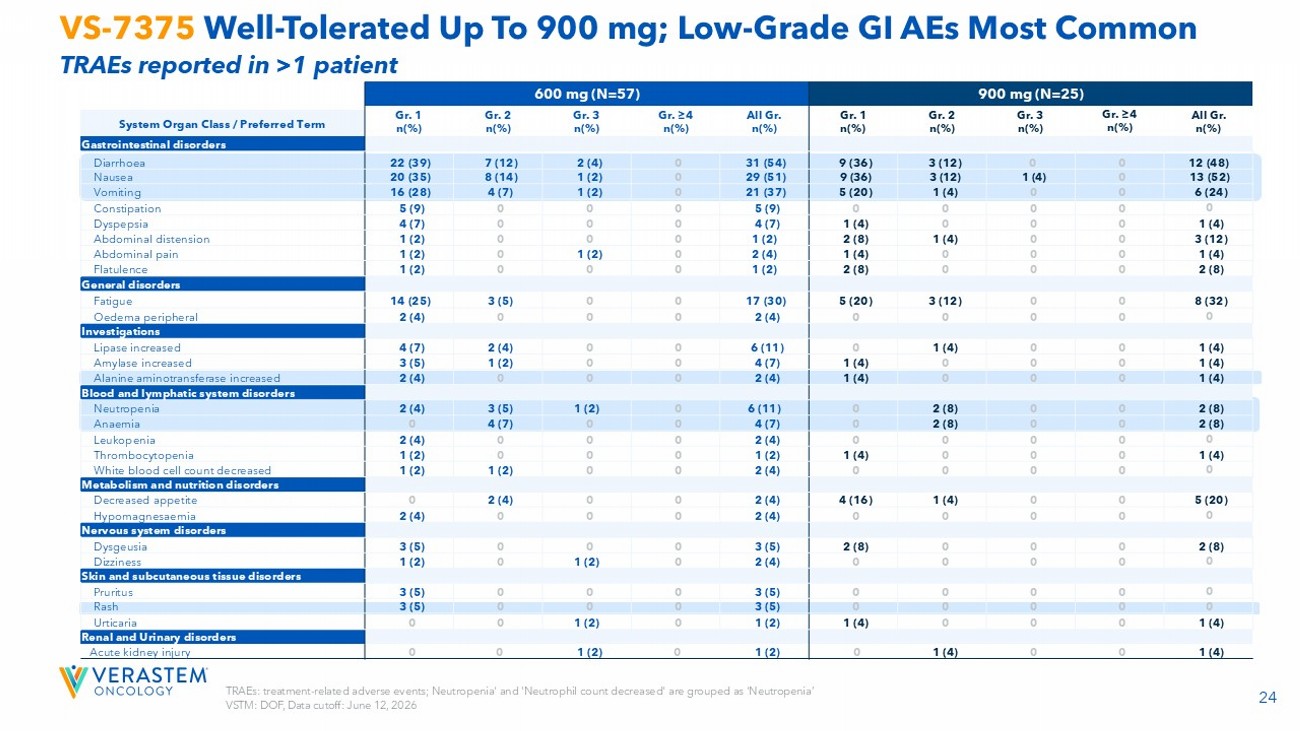
24 TRAEs: treatment - related adverse events; Neutropenia' and 'Neutrophil count decreased' are grouped as 'Neutropenia’ VSTM: DOF, Data cutoff: June 12, 2026 VS - 7375 Well - Tolerated Up To 900 mg; Low - Grade GI AEs Most Common TRAEs reported in >1 patient 900 mg (N=25) 600 mg (N=57) All Gr. n(%) Gr. ≥4 n(%) Gr. 3 n(%) Gr. 2 n(%) Gr. 1 n(%) All Gr. n(%) Gr. ≥4 n(%) Gr. 3 n(%) Gr. 2 n(%) Gr. 1 n(%) System Organ Class / Preferred Term Gastrointestinal disorders 12 (48) 0 0 3 (12) 9 (36) 31 (54) 0 2 (4) 7 (12) 22 (39) Diarrhoea 13 (52) 0 1 (4) 3 (12) 9 (36) 29 (51) 0 1 (2) 8 (14) 20 (35) Nausea 6 (24) 0 0 1 (4) 5 (20) 21 (37) 0 1 (2) 4 (7) 16 (28) Vomiting 0 0 0 0 0 5 (9) 0 0 0 5 (9) Constipation 1 (4) 0 0 0 1 (4) 4 (7) 0 0 0 4 (7) Dyspepsia 3 (12) 0 0 1 (4) 2 (8) 1 (2) 0 0 0 1 (2) Abdominal distension 1 (4) 0 0 0 1 (4) 2 (4) 0 1 (2) 0 1 (2) Abdominal pain 2 (8) 0 0 0 2 (8) 1 (2) 0 0 0 1 (2) Flatulence General disorders 8 (32) 0 0 3 (12) 5 (20) 17 (30) 0 0 3 (5) 14 (25) Fatigue 0 0 0 0 0 2 (4) 0 0 0 2 (4) Oedema peripheral Investigations 1 (4) 0 0 1 (4) 0 6 (11) 0 0 2 (4) 4 (7) Lipase increased 1 (4) 0 0 0 1 (4) 4 (7) 0 0 1 (2) 3 (5) Amylase increased 1 (4) 0 0 0 1 (4) 2 (4) 0 0 0 2 (4) Alanine aminotransferase increased Blood and lymphatic system disorders 2 (8) 0 0 2 (8) 0 6 (11) 0 1 (2) 3 (5) 2 (4) Neutropenia 2 (8) 0 0 2 (8) 0 4 (7) 0 0 4 (7) 0 Anaemia 0 0 0 0 0 2 (4) 0 0 0 2 (4) Leukopenia 1 (4) 0 0 0 1 (4) 1 (2) 0 0 0 1 (2) Thrombocytopenia 0 0 0 0 0 2 (4) 0 0 1 (2) 1 (2) White blood cell count decreased Metabolism and nutrition disorders 5 (20) 0 0 1 (4) 4 (16) 2 (4) 0 0 2 (4) 0 Decreased appetite 0 0 0 0 0 2 (4) 0 0 0 2 (4) Hypomagnesaemia Nervous system disorders 2 (8) 0 0 0 2 (8) 3 (5) 0 0 0 3 (5) Dysgeusia 0 0 0 0 0 2 (4) 0 1 (2) 0 1 (2) Dizziness Skin and subcutaneous tissue disorders 0 0 0 0 0 3 (5) 0 0 0 3 (5) Pruritus 0 0 0 0 0 3 (5) 0 0 0 3 (5) Rash 1 (4) 0 0 0 1 (4) 1 (2) 0 1 (2) 0 0 Urticaria Renal and Urinary disorders 1 (4) 0 0 1 (4) 0 1 (2) 0 1 (2) 0 0 Acute kidney injury
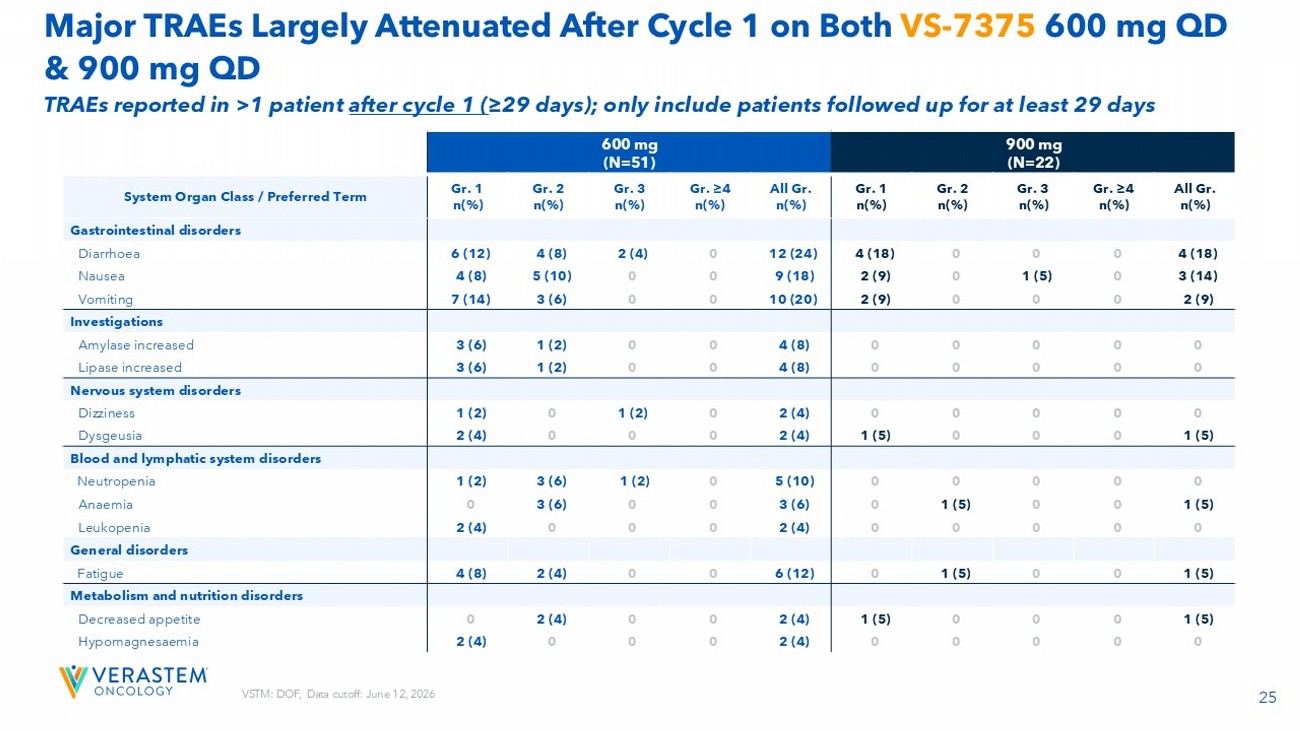
25 VSTM: DOF, Data cutoff: June 12, 2026 Major TRAEs Largely Attenuated After Cycle 1 on Both VS - 7375 600 mg QD & 900 mg QD 900 mg (N=22) 600 mg (N=51) All Gr. n(%) Gr. ≥4 n(%) Gr. 3 n(%) Gr. 2 n(%) Gr. 1 n(%) All Gr. n(%) Gr. ≥4 n(%) Gr. 3 n(%) Gr. 2 n(%) Gr. 1 n(%) System Organ Class / Preferred Term Gastrointestinal disorders 4 (18) 0 0 0 4 (18) 12 (24) 0 2 (4) 4 (8) 6 (12) Diarrhoea 3 (14) 0 1 (5) 0 2 (9) 9 (18) 0 0 5 (10) 4 (8) Nausea 2 (9) 0 0 0 2 (9) 10 (20) 0 0 3 (6) 7 (14) Vomiting Investigations 0 0 0 0 0 4 (8) 0 0 1 (2) 3 (6) Amylase increased 0 0 0 0 0 4 (8) 0 0 1 (2) 3 (6) Lipase increased Nervous system disorders 0 0 0 0 0 2 (4) 0 1 (2) 0 1 (2) Dizziness 1 (5) 0 0 0 1 (5) 2 (4) 0 0 0 2 (4) Dysgeusia Blood and lymphatic system disorders 0 0 0 0 0 5 (10) 0 1 (2) 3 (6) 1 (2) Neutropenia 1 (5) 0 0 1 (5) 0 3 (6) 0 0 3 (6) 0 Anaemia 0 0 0 0 0 2 (4) 0 0 0 2 (4) Leukopenia General disorders 1 (5) 0 0 1 (5) 0 6 (12) 0 0 2 (4) 4 (8) Fatigue Metabolism and nutrition disorders 1 (5) 0 0 0 1 (5) 2 (4) 0 0 2 (4) 0 Decreased appetite 0 0 0 0 0 2 (4) 0 0 0 2 (4) Hypomagnesaemia TRAEs reported in >1 patient after cycle 1 ( ≥29 days); only include patients followed up for at least 29 days
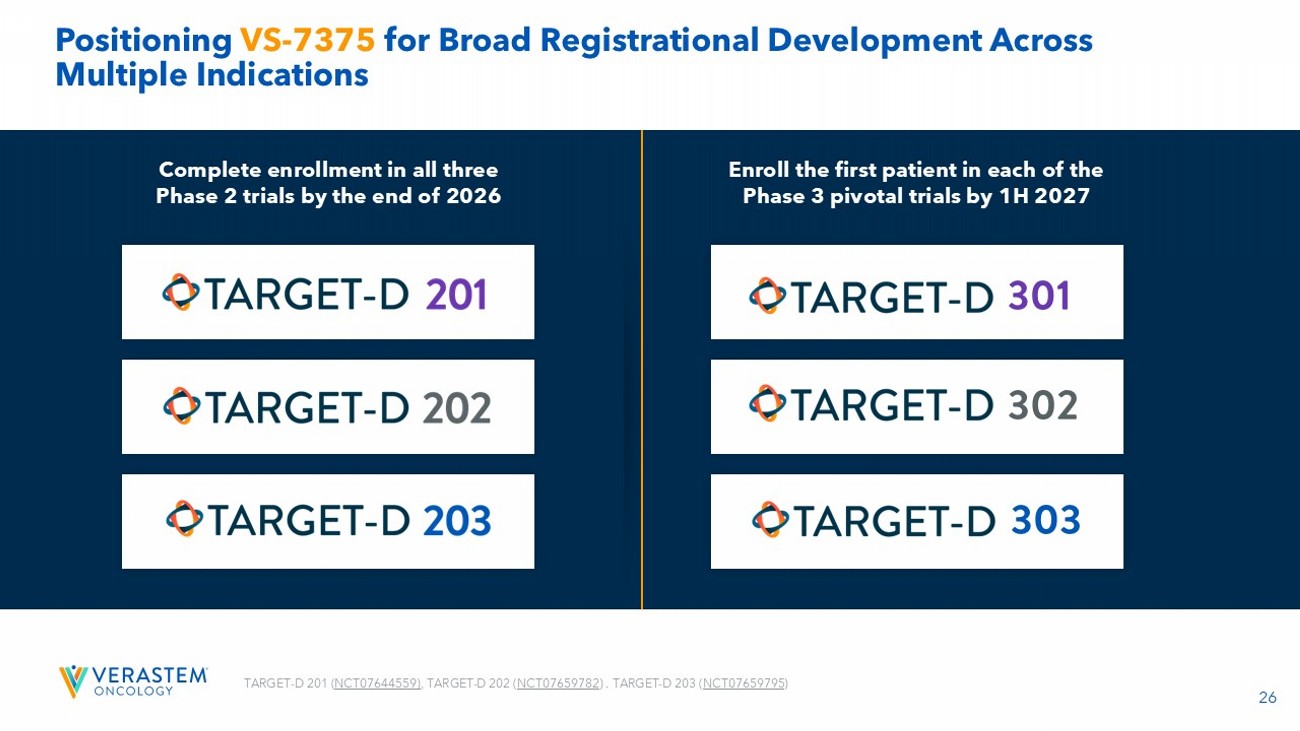
26 Positioning VS - 7375 for Broad Registrational Development Across Multiple Indications Complete enrollment in all three Phase 2 trials by the end of 2026 Enroll the first patient in each of the Phase 3 pivotal trials by 1H 2027 TARGET - D 201 ( NCT07644559 ) , TARGET - D 202 ( NCT07659782 ) . TARGET - D 203 ( NCT07659795 )
Rationale for New Clinical Collaborations with VS - 7375 Jonathan Pachter, PhD Chief Scientific Officer
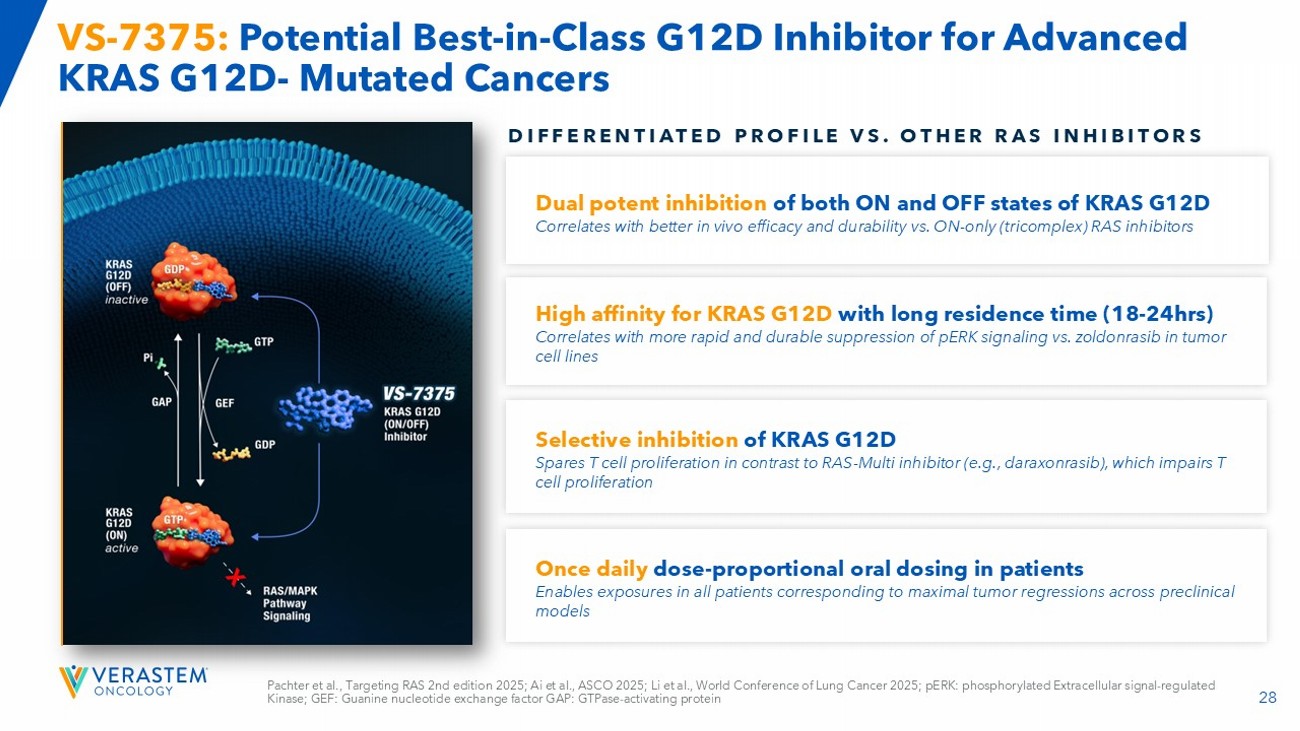
28 Pachter et al., Targeting RAS 2nd edition 2025; Ai et al., ASCO 2025; Li et al., World Conference of Lung Cancer 2025; pERK: pho sphorylated Extracellular signal - regulated Kinase; GEF: Guanine nucleotide exchange factor GAP: GTPase - activating protein VS - 7375: Potential Best - in - Class G12D Inhibitor for Advanced KRAS G12D - Mutated Cancers DIFFERENTIATED PROFILE VS. OTHER RAS INHIBITORS Dual potent i nhibition of both ON and OFF states of KRAS G12D Correlates with better in vivo efficacy and durability vs. ON - only (tricomplex) RAS inhibitors High affinity for KRAS G12D with long residence time (18 - 24hrs) Correlates with more rapid and durable suppression of pERK signaling vs. zoldonrasib in tumor cell lines Selective inhibition of KRAS G12D Spares T cell proliferation in contrast to RAS - Multi inhibitor (e.g., daraxonrasib), which impairs T cell proliferation Once daily dose - proportional oral dosing in patients Enables exposures in all patients corresponding to maximal tumor regressions across preclinical models
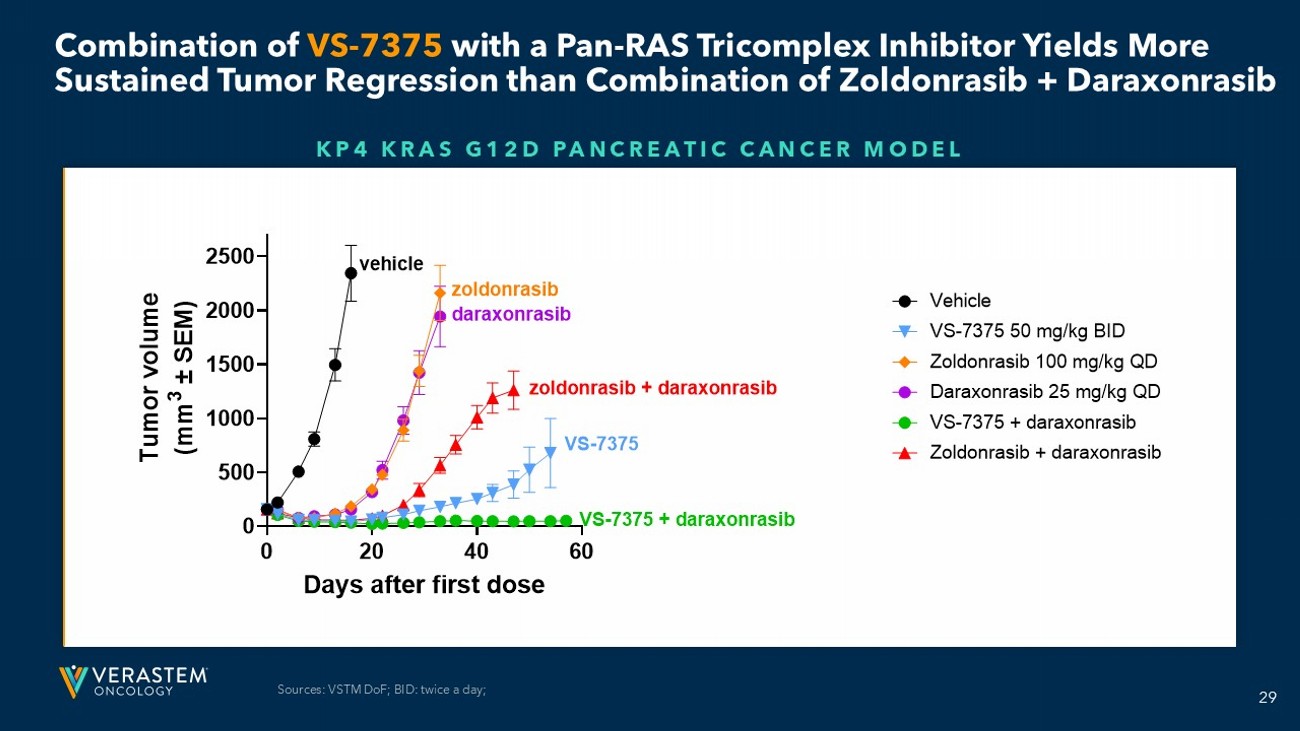
29 Combination of VS - 7375 with a Pan - RAS Tricomplex Inhibitor Yields More Sustained Tumor Regression than Combination of Zoldonrasib + Daraxonrasib KP4 KRAS G12D PANCREATIC CANCER MODEL 0 20 40 60 0 500 1000 1500 2000 2500 Days after first dose T u m o r v o l u m e ( m m 3 ± S E M ) Vehicle VS-7375 50 mg/kg BID Zoldonrasib 100 mg/kg QD Daraxonrasib 25 mg/kg QD VS-7375 + daraxonrasib Zoldonrasib + daraxonrasib vehicle daraxonrasib zoldonrasib zoldonrasib + daraxonrasib VS-7375 VS-7375 + daraxonrasib Sources: VSTM DoF ; BID: twice a day;
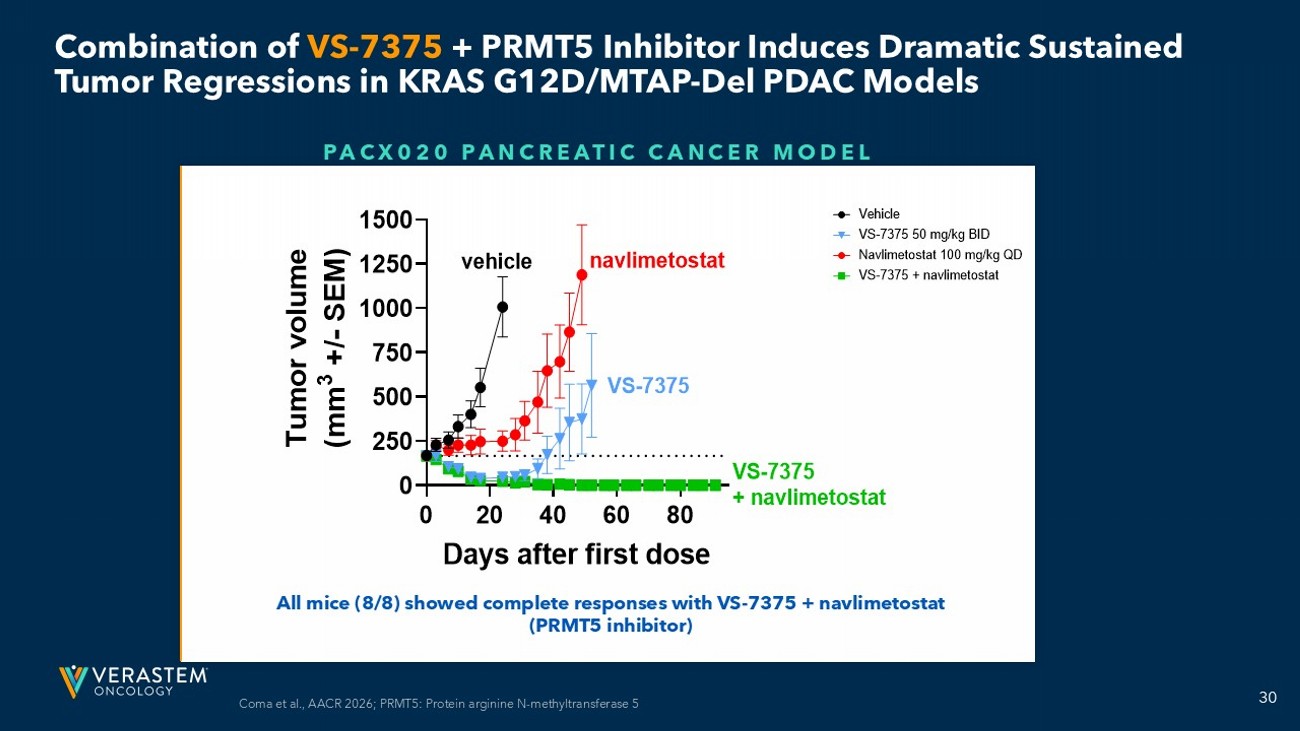
30 Combination of VS - 7375 + PRMT5 Inhibitor Induces Dramatic Sustained Tumor Regressions in KRAS G12D/MTAP - Del PDAC Models PACX020 PANCREATIC CANCER MODEL All mice (8/8) showed complete responses with VS - 7375 + navlimetostat (PRMT5 inhibitor) 0 20 40 60 80 0 250 500 750 1000 1250 1500 Days after first dose T u m o r v o l u m e ( m m 3 + / - S E M ) Vehicle VS-7375 50 mg/kg BID Navlimetostat 100 mg/kg QD VS-7375 + navlimetostat vehicle navlimetostat VS-7375 VS-7375 + navlimetostat 0 20 40 60 80 0 250 500 750 1000 1250 1500 Days after first dose T u m o r v o l u m e ( m m 3 + / - S E M ) Vehicle VS-7375 50 mg/kg BID Navlimetostat 100 mg/kg QD VS-7375 + navlimetostat vehicle navlimetostat VS-7375 VS-7375 + navlimetostat Coma et al., AACR 2026; PRMT5: Protein arginine N - methyltransferase 5

Closing Remarks Dan Paterson, President & CEO
32 VS - 7375 : Aiming to Define Treatment for KRAS G12D - Mutated Cancers Coma et al., AACR 2026 Selective KRAS G12D Inhibition Across Tumor Types Compelling Emerging Clinical Profile Potential Franchise Opportunity Pancreatic Cancer Colorectal Cancer Lung Cancer Other G12D Cancers SœJAJy a^IV_AIV]Vpy 3a]NlAIV]Vpy 91 ¥ ‡ƒ‡…

Thank you!

Q&A

Appendix
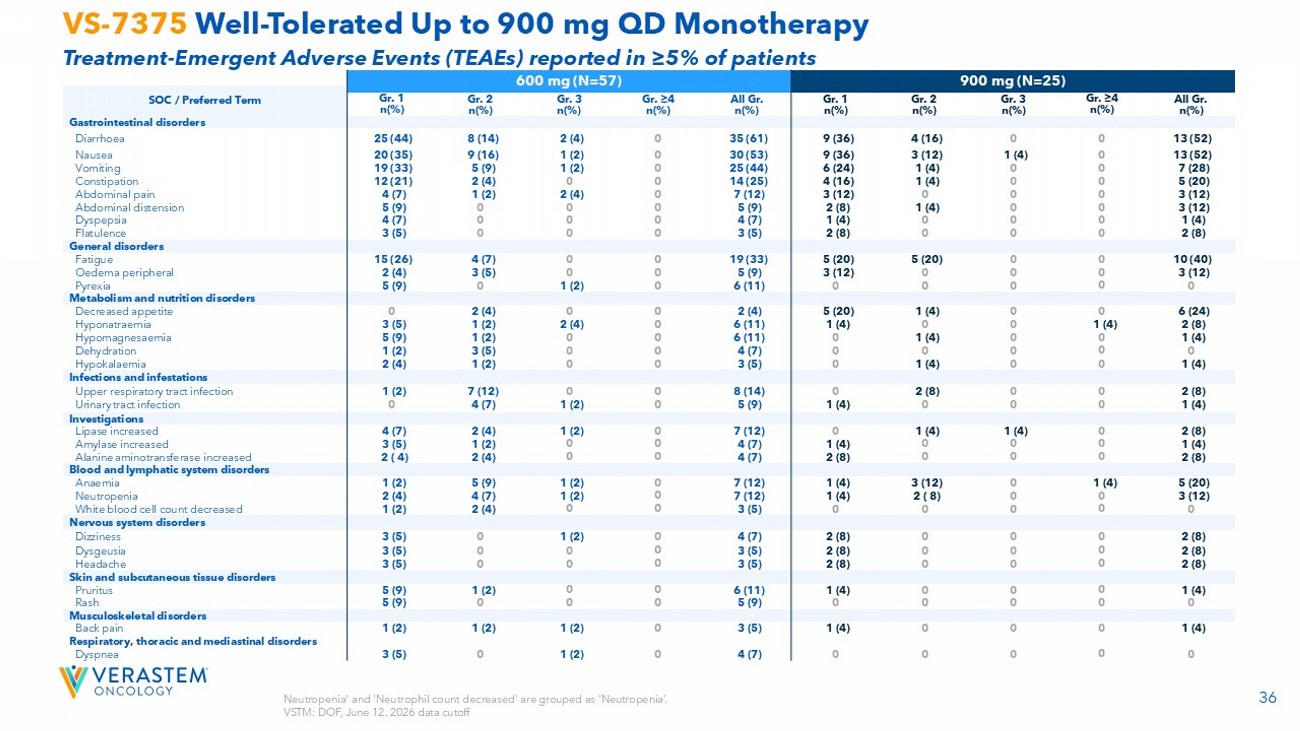
36 Neutropenia' and 'Neutrophil count decreased' are grouped as 'Neutropenia’. VSTM: DOF, June 12. 2026 data cutoff VS - 7375 Well - Tolerated Up to 900 mg QD Monotherapy Treatment - Emergent Adverse Events (TEAEs) reported in ≥5% of patients 900 mg (N=25) 600 mg (N=57) SOC / Preferred Term All Gr. n(%) Gr. ≥4 n(%) Gr. 3 n(%) Gr. 2 n(%) Gr. 1 n(%) All Gr. n(%) Gr. ≥4 n(%) Gr. 3 n(%) Gr. 2 n(%) Gr. 1 n(%) Gastrointestinal disorders 13 (52) 0 0 4 (16) 9 (36) 35 (61) 0 2 (4) 8 (14) 25 (44) Diarrhoea 13 (52) 0 1 (4) 3 (12) 9 (36) 30 (53) 0 1 (2) 9 (16) 20 (35) Nausea 7 (28) 0 0 1 (4) 6 (24) 25 (44) 0 1 (2) 5 (9) 19 (33) Vomiting 5 (20) 0 0 1 (4) 4 (16) 14 (25) 0 0 2 (4) 12 (21) Constipation 3 (12) 0 0 0 3 (12) 7 (12) 0 2 (4) 1 (2) 4 (7) Abdominal pain 3 (12) 0 0 1 (4) 2 (8) 5 (9) 0 0 0 5 (9) Abdominal distension 1 (4) 0 0 0 1 (4) 4 (7) 0 0 0 4 (7) Dyspepsia 2 (8) 0 0 0 2 (8) 3 (5) 0 0 0 3 (5) Flatulence General disorders 10 (40) 0 0 5 (20) 5 (20) 19 (33) 0 0 4 (7) 15 (26) Fatigue 3 (12) 0 0 0 3 (12) 5 (9) 0 0 3 (5) 2 (4) Oedema peripheral 0 0 0 0 0 6 (11) 0 1 (2) 0 5 (9) Pyrexia Metabolism and nutrition disorders 6 (24) 0 0 1 (4) 5 (20) 2 (4) 0 0 2 (4) 0 Decreased appetite 2 (8) 1 (4) 0 0 1 (4) 6 (11) 0 2 (4) 1 (2) 3 (5) Hyponatraemia 1 (4) 0 0 1 (4) 0 6 (11) 0 0 1 (2) 5 (9) Hypomagnesaemia 0 0 0 0 0 4 (7) 0 0 3 (5) 1 (2) Dehydration 1 (4) 0 0 1 (4) 0 3 (5) 0 0 1 (2) 2 (4) Hypokalaemia Infections and infestations 2 (8) 0 0 2 (8) 0 8 (14) 0 0 7 (12) 1 (2) Upper respiratory tract infection 1 (4) 0 0 0 1 (4) 5 (9) 0 1 (2) 4 (7) 0 Urinary tract infection Investigations 2 (8) 0 1 (4) 1 (4) 0 7 (12) 0 1 (2) 2 (4) 4 (7) Lipase increased 1 (4) 0 0 0 1 (4) 4 (7) 0 0 1 (2) 3 (5) Amylase increased 2 (8) 0 0 0 2 (8) 4 (7) 0 0 2 (4) 2 ( 4) Alanine aminotransferase increased Blood and lymphatic system disorders 5 (20) 1 (4) 0 3 (12) 1 (4) 7 (12) 0 1 (2) 5 (9) 1 (2) Anaemia 3 (12) 0 0 2 ( 8) 1 (4) 7 (12) 0 1 (2) 4 (7) 2 (4) Neutropenia 0 0 0 0 0 3 (5) 0 0 2 (4) 1 (2) White blood cell count decreased Nervous system disorders 2 (8) 0 0 0 2 (8) 4 (7) 0 1 (2) 0 3 (5) Dizziness 2 (8) 0 0 0 2 (8) 3 (5) 0 0 0 3 (5) Dysgeusia 2 (8) 0 0 0 2 (8) 3 (5) 0 0 0 3 (5) Headache Skin and subcutaneous tissue disorders 1 (4) 0 0 0 1 (4) 6 (11) 0 0 1 (2) 5 (9) Pruritus 0 0 0 0 0 5 (9) 0 0 0 5 (9) Rash Musculoskeletal disorders 1 (4) 0 0 0 1 (4) 3 (5) 0 1 (2) 1 (2) 1 (2) Back pain Respiratory, thoracic and mediastinal disorders 0 0 0 0 0 4 (7) 0 1 (2) 0 3 (5) Dyspnea

37 VS - 7375 Key Milestones x First patient dosed in TARGET - D 201 Registration - Directed Trial June 2026 • Complete enrollment across all three TARGET - D Phase 2 Trials • Report an update on TARGET - D 101 across tumor types and more follow up Mid - 2026 2H 2026 End of 2026 1H 2027 • Enroll first patient in each of the Phase 3 TARGET - D pivotal prials (PDAC, CRC, NSCLC) • Dose first patient in TARGET - D 202 (NSCLC) & TARGET - D 203 (CRC) Registration - Directed Trials • Complete target enrollment in TARGET - D 101 PDAC, NSCLC and CRC cohorts