Exhibit 99.2
EHA 2026 Recap June 2026 © 2026 Legend Biotech. All rights reserved.
Forward Looking Statements 2 This presentation has been prepared by Legend Biotech Corporation (“Legend Biotech” or the “Company”) solely for information purpose and does not contain all relevant information relating to the Company. The safety and efficacy of the agents and/or uses under investigation discussed in this presentation have not been established, except to the extent specifically provided by marketing authorizations previously received from relevant health authorities. Further, for investigational agents and/or uses, the Company cannot guarantee health authority approval or that such agents and/or uses will become commercially available in any country. Certain information contained in this presentation and statements made orally during this presentation relate to or are based on studies, publications, surveys and other data obtained from third - party sources and Legend Biotech's own internal estimates and research. While Legend Biotech believes these third - party sources to be reliable as of the date of this presentation, it has not independently verified, and makes no representation as to the adequacy, fairness, accuracy or completeness of, any information obtained from third - party sources. While Legend Biotech believes its internal research is reliable, such research has not been verified by any independent source. Statements in this presentation about future expectations, plans and prospects, as well as any other statements regarding matters that are not historical facts, constitute “forward - looking statements” within the meaning of The Private Securities Litigation Reform Act of 1995. These statements include, but are not limited to, statements relating to Legend Biotech’s strategies and objectives; the ongoing Phase 1 clinical trial of LB2501; the potential benefits of LB2501, including the reproducibility and durability of any favorable results initially seen in patients dosed to date in clinical trials; LB2501's potential to be first - in - class; the progress of submissions with the FDA, the EMA and other regulatory authorities; expected results and timing of clinical trials; Legend Biotech’s expectations on advancing its pipeline and product portfolio, including TaVec and LB2501; and the potential benefits of Legend Biotech’s product candidates and its in vivo platform. The words “anticipate,” “believe,” “continue,” “could,” “estimate,” “expect,” “intend,” “may,” “plan,” “potential,” “predict,” “project,” “should,” “target,” “will,” “would” and similar expressions are intended to identify forward - looking statements, although not all forward - looking statements contain these identifying words. Actual results may differ materially from those indicated by such forward - looking statements as a result of various important factors. Legend Biotech’s expectations could be affected by, among other things, uncertainties involved in the development of new pharmaceutical products; unexpected clinical trial results, including as a result of additional analysis of existing clinical data or unexpected new clinical data; unexpected regulatory actions or delays, including requests for additional safety and/or efficacy data or analysis of data, or government regulation generally; unexpected delays as a result of actions undertaken, or failures to act, by our third party partners; uncertainties arising from challenges to Legend Biotech’s patent or other proprietary intellectual property protection, including the uncertainties involved in the U.S. litigation process; competition in general; government, industry, and general product pricing and other political pressures; as well as the other factors discussed in the “Risk Factors” section of Legend Biotech’s Annual Report on Form 20 - F for the year ended December 31, 2025, filed with the Securities and Exchange Commission (SEC) on March 10, 2026 and Legend Biotech’s other filings with the SEC. Should one or more of these risks or uncertainties materialize, or should underlying assumptions prove incorrect, actual results may vary materially from those described in this presentation as anticipated, believed, estimated or expected. Any forward - looking statements contained in this presentation speak only as of the date of this presentation. Legend Biotech specifically disclaims any obligation to update any forward - looking statement, whether as a result of new information, future events or otherwise. .
3 Agenda In Vivo Platform Overview 1 Recap of LB2501 Data from EHA 2026 2 Next Steps 3 Q&A 4

4
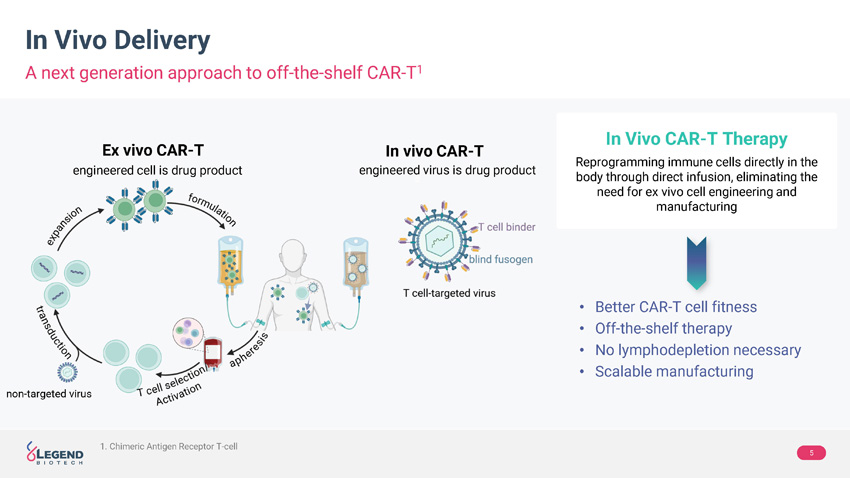
5 In Vivo Delivery A next generation approach to off - the - shelf CAR - T 1 • Better CAR - T cell fitness • Off - the - shelf therapy • No lymphodepletion necessary • Scalable manufacturing Ex vivo CAR - T In vivo CAR - T non - targeted virus engineered cell is drug product engineered virus is drug product In Vivo CAR - T Therapy Reprogramming immune cells directly in the body through direct infusion, eliminating the need for ex vivo cell engineering and manufacturing 1. Chimeric Antigen Receptor T - cell
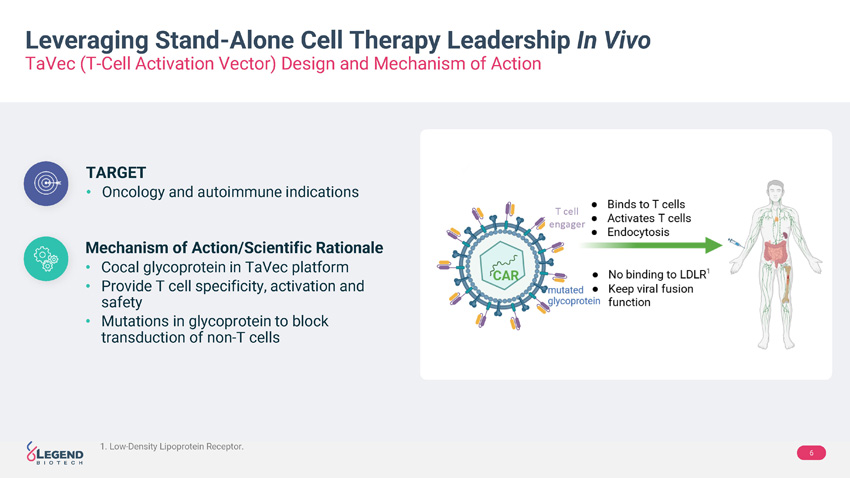
6 Leveraging Stand - Alone Cell Therapy Leadership In Vivo TaVec (T - Cell Activation Vector) Design and Mechanism of Action TARGET • Oncology and autoimmune indications Mechanism of Action/Scientific Rationale • Cocal glycoprotein in TaVec platform • Provide T cell specificity, activation and safety • Mutations in glycoprotein to block transduction of non - T cells T cell engager 1 1. Low - Density Lipoprotein Receptor .
7
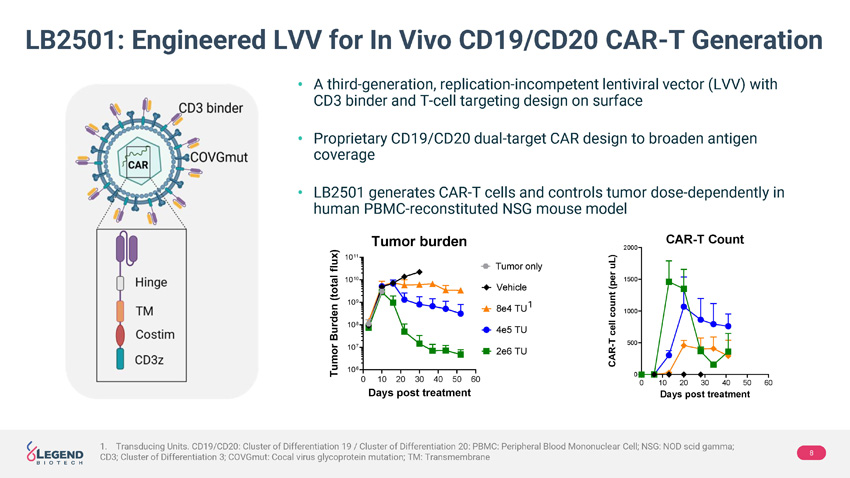
8 LB2501: Engineered LVV for In Vivo CD19/CD20 CAR - T Generation • A third - generation, replication - incompetent lentiviral vector (LVV) with CD3 binder and T - cell targeting design on surface • Proprietary CD19/CD20 dual - target CAR design to broaden antigen coverage • LB2501 generates CAR - T cells and controls tumor dose - dependently in human PBMC - reconstituted NSG mouse model 1 1. Transducing Units. CD19/CD20: Cluster of Differentiation 19 / Cluster of Differentiation 20: PBMC: Peripheral Blood Mononucle ar Cell; NSG: NOD scid gamma; CD3; Cluster of Differentiation 3; COVGmut : Cocal virus glycoprotein mutation; TM: Transmembrane
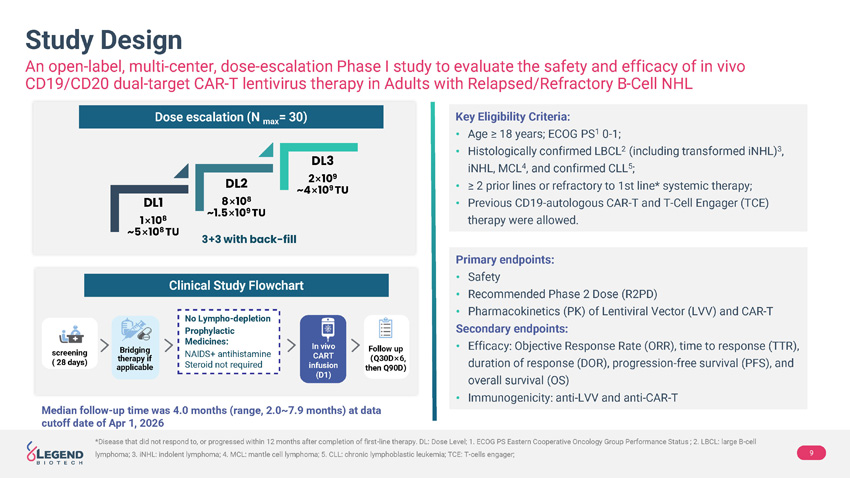
9 *Disease that did not respond to, or progressed within 12 months after completion of first - line therapy. DL: Dose Level; 1. ECOG PS Eastern Cooperative Oncology Group Performance Status ; 2. LBCL: large B - cell lymphoma; 3. iNHL : indolent lymphoma; 4. MCL: mantle cell lymphoma; 5. CLL: chronic lymphoblastic leukemia; TCE: T - cells engager; Study Design An open - label, multi - center, dose - escalation Phase I study to evaluate the safety and efficacy of in vivo CD19/CD20 dual - target CAR - T lentivirus therapy in Adults with Relapsed/Refractory B - Cell NHL Primary endpoint s : • Safety • Recommended Phase 2 D ose (R2PD) • Pharmacokinetics (PK) of Lentiviral Vector (LVV) and CAR - T Secondary endpoints: • Efficacy : Objective Response Rate ( ORR), time to response (TTR), duration of response (DOR), progression - free survival (PFS), and overall survival (OS) • Immunogenicity: anti - LVV and anti - CAR - T Key Eligibility Criteria: • Age ≥ 18 years; ECOG PS 1 0 - 1; • Histologically confirmed LBCL 2 (including transformed iNHL ) 3 , iNHL , MCL 4 , and confirmed CLL 5 ; • ≥ 2 prior lines or refractory to 1st line* systemic therapy; • Previous CD19 - autologous CAR - T and T - Cell Engager (TCE) therapy were allowed. Dose escalation (N max = 30) DL1 1 × 10 8 ~5 × 10 8 TU DL2 8 × 10 8 ~1.5 × 10 9 TU DL3 2 × 10 9 ~4 × 10 9 TU 3+3 with back - fill Clinical Study Flowchart screening ( 28 days) Bridging therapy if applicable In vivo CART infusion (D1) Follow up ( Q30D × 6, then Q90D ) No Lympho - depletion P rophylactic Medicines: NAIDS+ antihistamine Steroid not required Median follow - up time was 4.0 months (range, 2.0~7.9 months) at data cutoff date of Apr 1, 2026
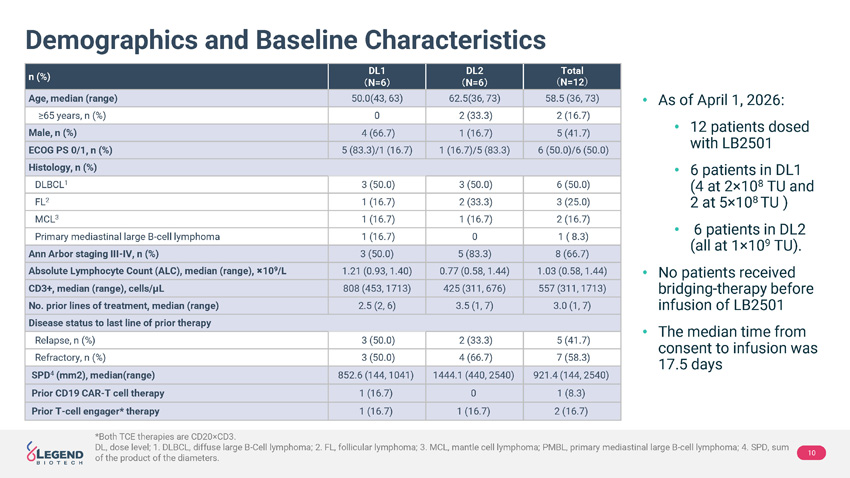
10 *Both TCE therapies are CD20 × CD3. DL, dose level; 1. DLBCL, diffuse large B - Cell lymphoma; 2. FL, follicular lymphoma; 3. MCL, mantle cell lymphoma; PMBL, primary mediastinal large B - cell lymphoma; 4. SPD, sum of the product of the diameters. Demographics and Baseline Characteristics Total ʤ N=12 ʥ DL2 㸦 N=6 㸧 DL1 㸦 N=6 㸧 n (%) 58.5 (36, 73) 62.5(36, 73) 50.0(43, 63) Age, median (range) 2 (16.7) 2 (33.3) 0 ≥ 65 years, n (%) 5 (41.7) 1 (16.7) 4 (66.7) Male, n (%) 6 (50.0)/6 (50.0) 1 (16.7)/5 (83.3) 5 (83.3)/1 (16.7) ECOG PS 0/1, n (%) Histology, n (%) 6 (50.0) 3 (50.0) 3 (50.0) DLBCL 1 3 (25.0) 2 (33.3) 1 (16.7) FL 2 2 (16.7) 1 (16.7) 1 (16.7) MCL 3 1 ( 8.3) 0 1 (16.7) Primary mediastinal large B - cell lymphoma 8 (66.7) 5 (83.3) 3 (50.0) Ann Arbor staging III - IV, n (%) 1.03 (0.58, 1.44) 0.77 (0.58, 1.44) 1.21 (0.93, 1.40) Absolute Lymphocyte Count (ALC), median (range), ̩ 10 9 /L 557 (311, 1713) 425 (311, 676) 808 (453, 1713) CD3+, median (range), cells/ μL 3.0 (1, 7) 3.5 (1, 7) 2.5 (2, 6) No. prior lines of treatment, median (range) Disease status to last line of prior therapy 5 (41.7) 2 (33.3) 3 (50.0) Relapse, n (%) 7 (58.3) 4 (66.7) 3 (50.0) Refractory, n (%) 921.4 (144, 2540) 1444.1 (440, 2540) 852.6 (144, 1041) SPD 4 (mm2), median(range) 1 (8.3) 0 1 (16.7) Prior CD19 CAR - T cell therapy 2 (16.7) 1 (16.7) 1 (16.7) Prior T - cell engager* therapy • As of April 1, 2026: • 12 patients dosed with LB2501 • 6 patients in DL1 (4 at 2 × 10 8 TU and 2 at 5 × 10 8 TU ) • 6 patients in DL2 (all at 1 × 10 9 TU). • No patients received bridging - therapy before infusion of LB2501 • The median time from consent to infusion was 17.5 days
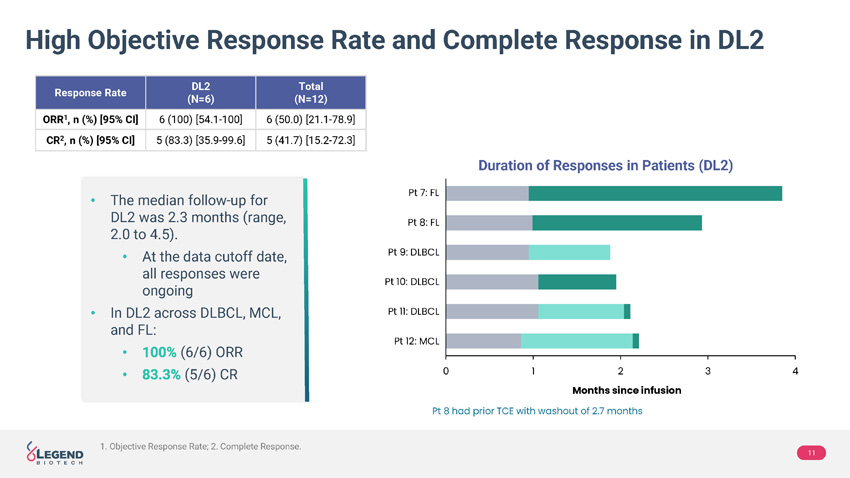
11 • The median follow - up for DL2 was 2.3 months (range, 2.0 to 4.5). • At the data cutoff date, all responses were ongoing • In DL2 across DLBCL, MCL, and FL: • (6/6) ORR • (5/6) CR High Objective Response Rate and Complete Response in DL2 Duration of Responses in Patients (DL2) Total (N=12) DL2 (N=6) Response Rate 6 (50.0) [21.1 - 78.9] 6 (100) [54.1 - 100] ORR 1 , n (%) [95% CI] 5 (41.7) [15.2 - 72.3] 5 (83.3) [35.9 - 99.6] CR 2 , n (%) [95% CI] 0 1 2 3 4 Pt 7: FL Pt 8: FL Pt 9: DLBCL Pt 10: DLBCL Pt 12: MCL Pt 11: DLBCL Pt 8 had prior TCE with washout of 2.7 months Months since infusion 1. Objective Response Rate; 2. Complete Response.
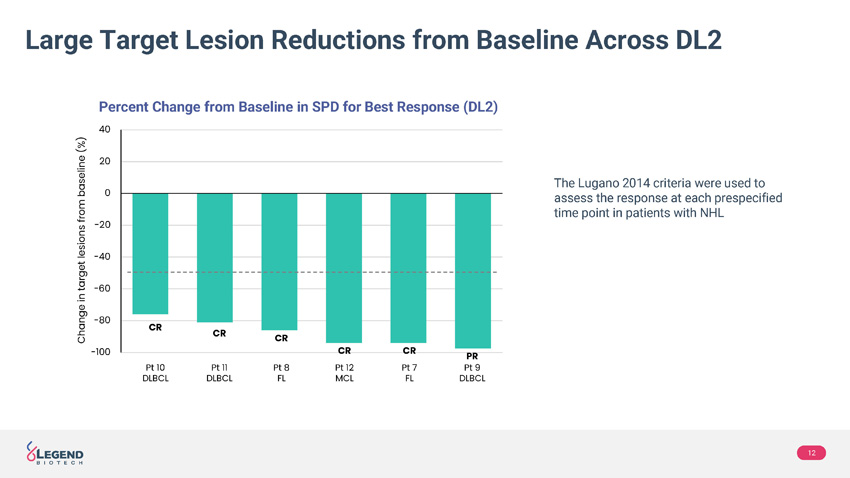
12 Large Target Lesion Reductions from Baseline Across DL2 The Lugano 2014 criteria were used to assess the response at each prespecified time point in patients with NHL Percent C hange from B aseline in SPD for B est R esponse (DL2) -100 -80 -60 -40 -20 0 20 40 Change in target lesions from baseline (%) CR CR CR CR CR PR Pt 10 DLBCL Pt 11 DLBCL Pt 8 FL Pt 12 MCL Pt 7 FL Pt 9 DLBCL
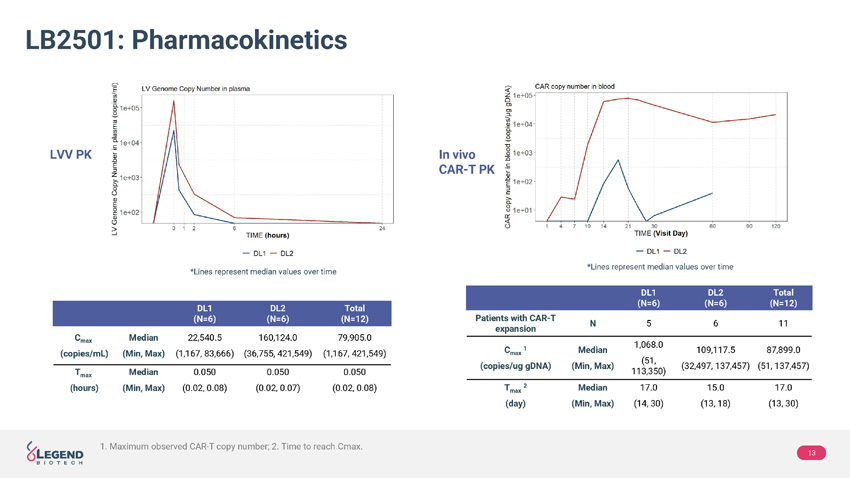
13 LB2501: Pharmacokinetics Total (N=12) DL2 (N=6) DL1 (N=6) 11 6 5 N Patients with CAR - T expansion 87,899.0 ( 51, 137,457 ) 109,117.5 ( 32,497, 137,457 ) 1,068.0 (51, 113,350) Median (Min, Max) C max 1 (copies/ug gDNA) 17.0 ( 13, 30 ) 15.0 ( 13, 18 ) 17.0 ( 14, 30 ) Median (Min, Max) T max 2 (day) Total (N=12) DL2 (N=6) DL1 (N=6) 79,905.0 (1,167, 421,549) 160,124.0 ( 36,755, 421,549 ) 22,540.5 ( 1,167, 83,666 ) Median (Min, Max) C max (copies/mL) 0.050 ( 0.02, 0.08 ) 0.050 ( 0.02, 0.07 ) 0.050 ( 0.02, 0.08 ) Median (Min, Max) T max (hours) LVV PK In vivo CAR - T PK *Lines represent median values over time *Lines represent median values over time 1. Maximum observed CAR - T copy number; 2. Time to reach Cmax .
14 Confirmed Expansion and Persistent PK • Viral copy number in peripheral blood peaked immediately after infusion and decreased to undetectable concentrations within 24 hours • In vivo CAR - T expansion was detected by qPCR 1 in 5/6 patients (83%) at DL1 and all patients (6/6, 100%) at DL2 in a dose - dependent manner . At the time of data cutoff, patients exhibited persistent PK • In DL2: • 109,117.5 copies/ μ g DNA • 15 days 1. Quantitative Polymerase Chain Reaction.
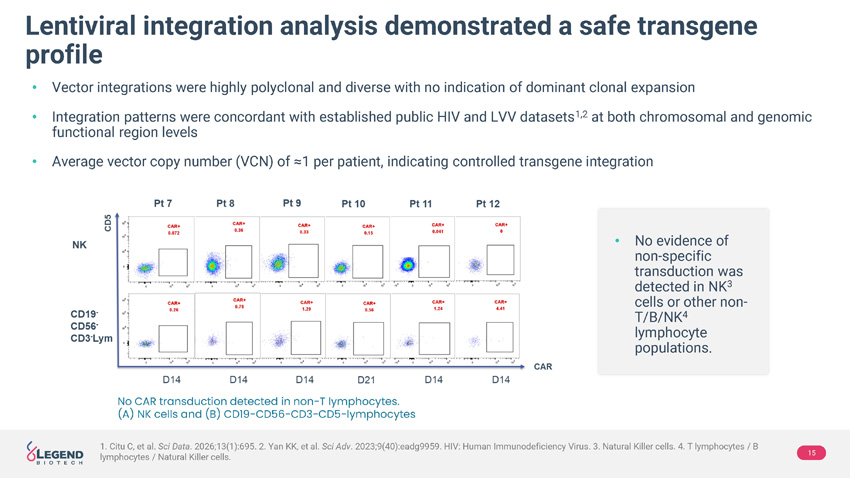
15 Lentiviral integration analysis demonstrated a safe transgene profile • Vector integrations were highly polyclonal and diverse with no indication of dominant clonal expansion • Integration patterns were concordant with established public HIV and LVV datasets 1,2 at both chromosomal and genomic functional region levels • Average vector copy number (VCN) of ≈1 per patient, indicating controlled transgene integration • No evidence of non - specific transduction was detected in NK 3 cells or other non - T/B/NK 4 lymphocyte populations. No CAR transduction detected in non - T lymphocytes. ( A) NK cells and (B) CD19−CD56−CD3−CD5−lymphocytes 1. Citu C, et al. Sci Data . 2026;13(1):695. 2. Yan KK, et al. Sci Adv . 2023;9(40):eadg9959. HIV: Human Immunodeficiency Virus. 3. Natural Killer cells. 4. T lymphocytes / B lymphocytes / Natural Killer cells.
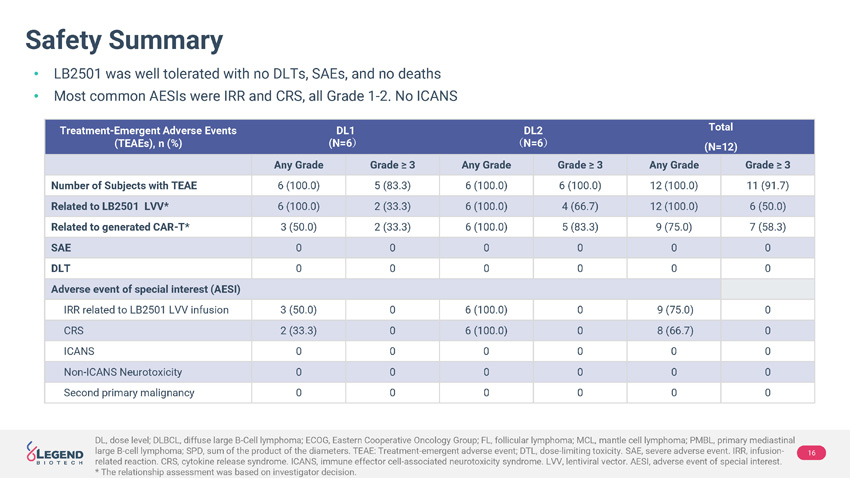
16 DL, dose level; DLBCL, diffuse large B - Cell lymphoma; ECOG, Eastern Cooperative Oncology Group; FL, follicular lymphoma; MCL, ma ntle cell lymphoma; PMBL, primary mediastinal large B - cell lymphoma; SPD, sum of the product of the diameters. TEAE: Treatment - emergent adverse event; DTL, dose - limiting toxi city. SAE, severe adverse event. IRR, infusion - related reaction. CRS, cytokine release syndrome. ICANS, immune effector cell - associated neurotoxicity syndrome. LVV, lentiviral vector. AESI, adverse event of special interest. * The relationship assessment was based on investigator decision. Safety Summary • LB2501 was well tolerated with no DLTs, SAEs, and no deaths • Most common AESIs were IRR and CRS, all Grade 1 - 2. No ICANS Total (N=12) DL2 ʤ N=6 ʥ DL1 (N=6 ʥ Treatment - Emergent Adverse Events (TEAEs), n (%) Grade ≥ 3 Any Grade Grade ≥ 3 Any Grade Grade ≥ 3 Any Grade 11 (91.7) 12 (100.0) 6 (100.0) 6 (100.0) 5 (83.3) 6 (100.0) Number of Subjects with TEAE 6 (50.0) 12 (100.0) 4 (66.7) 6 (100.0) 2 (33.3) 6 (100.0) Related to LB2501 LVV* 7 (58.3) 9 (75.0) 5 (83.3) 6 (100.0) 2 (33.3) 3 (50.0) Related to generated CAR - T* 0 0 0 0 0 0 SAE 0 0 0 0 0 0 DLT Adverse event of special interest (AESI) 0 9 (75.0) 0 6 (100.0) 0 3 (50.0) IRR related to LB2501 LVV infusion 0 8 (66.7) 0 6 (100.0) 0 2 (33.3) CRS 0 0 0 0 0 0 ICANS 0 0 0 0 0 0 Non - ICANS Neurotoxicity 0 0 0 0 0 0 Second primary malignancy
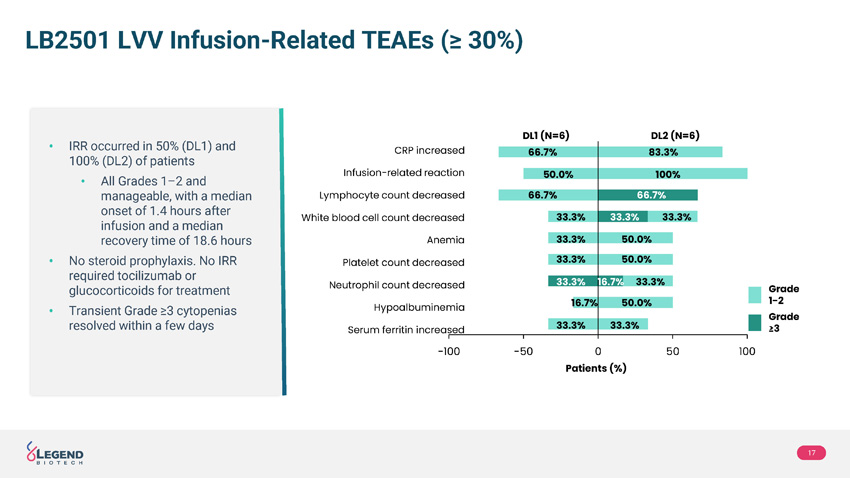
17 LB2501 LVV Infusion - Related TEAEs (≥ 30%) • IRR occurred in 50% (DL1) and 100% (DL2) of patients • All Grades 1 – 2 and manageable, with a median onset of 1.4 hours after infusion and a median recovery time of 18.6 hours • No steroid prophylaxis. No IRR required tocilizumab or glucocorticoids for treatment • Transient Grade ≥3 cytopenias resolved within a few days -100 -50 0 50 100 66.7% 66.7% 50.0% 33.3% 33.3% 33.3% 33.3% 33.3% 33.3% 33.3% 33.3% 50.0% 50.0% 50.0% 33.3% 66.7% 16.7% 16.7% 100% 83.3% CRP increased Lymphocyte count decreased Infusion - related reaction White blood cell count decreased Anemia Platelet count decreased Neutrophil count decreased Serum ferritin increased Hypoalbuminemia Patients (%) DL2 (N=6) DL1 (N=6) Grade 1 - 2 Grade ≥3
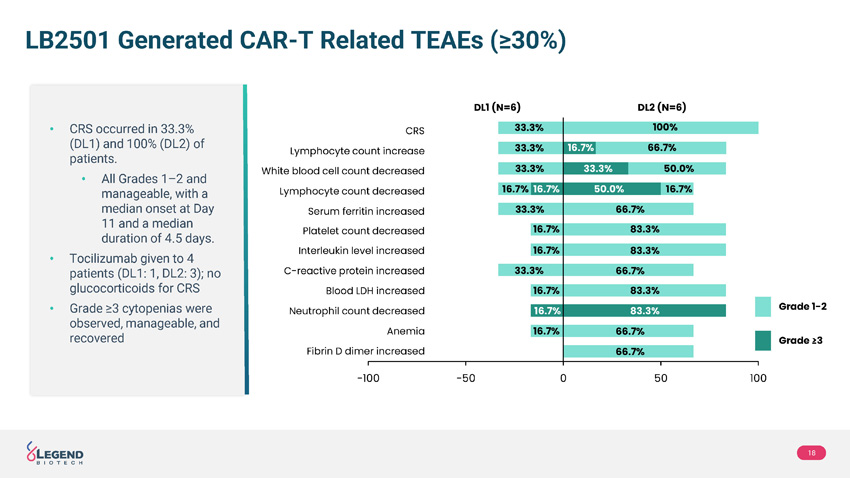
18 LB2501 Generated CAR - T Related TEAEs (≥30%) • CRS occurred in 33.3% (DL1) and 100% (DL2) of patients. • All Grades 1 – 2 and manageable, with a median onset at Day 11 and a median duration of 4.5 days. • Tocilizumab given to 4 patients (DL1: 1, DL2: 3); no glucocorticoids for CRS • Grade ≥3 cytopenias were observed, manageable, and recovered -100 -50 0 50 100 33.3% 33.3% 33.3% 16.7% 33.3% 16.7% 16.7% 66.7% 16.7% 50.0% 100% CRS White blood cell count decreased Lymphocyte count increase Lymphocyte count decreased Serum ferritin increased Platelet count decreased C - reactive protein increased Fibrin D dimer increased Neutrophil count decreased DL2 (N=6) DL1 (N=6) Grade 1 - 2 Grade ≥3 Interleukin level increased Anemia Blood LDH increased 33.3% 16.7% 16.7% 16.7% 16.7% 50.0% 16.7% 66.7% 83.3% 83.3% 83.3% 83.3% 66.7% 66.7% 66.7% 33.3%
19 Conclusions • In this First - In - Human Phase 1 study in R/R B - NHL, LB2501 showed a favorable safety profile and promising efficacy results: • LB2501 was well tolerated: no DLT, no SAE, no ICANS, and no deaths • IRR and CRS were all Grade 1 – 2, no glucocorticoid treatment • At DL2, 100% ORR and 83.3% CR achieved across DLBCL, MCL and FL • Dose - dependent expansion was observed, with consistent expansion at DL2 • LB2501 establishes a proof - of - concept for TaVec in vivo CAR - T platform in clinic; it showed T - cell specific transduction and robust CAR - T expansion, polyclonal random integration, and rapid vector clearance Legend believes t hese findings support further development of LB2501 as potential first - in class off - the - shelf, single - infusion, outpatient use, in vivo CD19/CD20 dual - target CAR - T therapy in R/R B - NHL

20
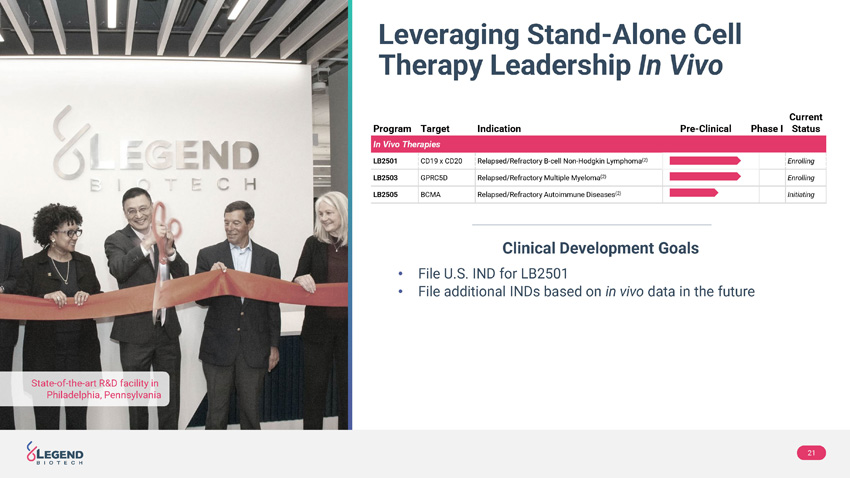
Leveraging Stand - Alone Cell Therapy Leadership In Vivo State - of - the - art R&D facility in Philadelphia, Pennsylvania 21 Current Status Phase I Pre - Clinical Indication Target Program In Vivo Therapies Enrolling Relapsed/Refractory B - cell Non - Hodgkin Lymphoma (2) CD19 x CD20 LB2501 Enrolling Relapsed/Refractory Multiple Myeloma (2) GPRC5D LB2503 Initiating Relapsed/Refractory Autoimmune Diseases (2) BCMA LB2505 Clinical Development Goals • File U.S. IND for LB2501 • File additional INDs based on in vivo data in the future

22

24