
Exhibit 99.2 Vopimetostat and RAS(ON) combination data June 8, 2026
Disclaimer and safe harbor statement Certain statements in this presentation may be considered forward-looking statements. All statements other than statements of historical fact are statements that could be deemed forward-looking statements, including all statements regarding the intent, belief, or current expectation of Tango and members of the Tango senior management team. Forward-looking statements are not purely historical and may be accompanied by terminology such as “may”, “should”, “expect”, “intend”, “will”, “plan”, “path”, “achievable”, “milestones”, “goal”, “forecast”, “estimate”, “potential”, “anticipate”, “believe”, “predict”, or “continue”, or the negatives of these terms or variations of them or similar terminology. For example, express or implied statements concerning the following include or constitute forward- looking statements: the potential anticipated benefits, tolerability, efficacy and therapeutic profile of Tango's PRMT5 inhibitors, as both standalone treatments and in combination with RAS(ON)-inhibitors; Tango’s belief that it has a competitive advantage; Tango’s regulatory plans and expectations, including its expectation that the combination of vopimetostat and RAS inhibitors could support a pivotal study in first line pancreatic cancer and an innovative and fast path to first line approvals and accelerated second line approval; Tango’s expected cash runway; Tango’s plans for future trials, including combination trials, and the design, initiation and the release of clinical data, and timing related thereto, for vopimetostat and TNG456, including with RAS(ON) inhibitors for vopimetostat; the expected benefits of the Company's development candidates and other product candidates (including for combination studies); the Company’s expectations around the size and value of the potential patient population for PRMT5 inhibitors (including for lung and pancreatic cancers); potential combination strategies and uses for PRMT5 inhibitors, including vopimetostat and TNG456; and the development and regulatory plans for the PRMT5 franchise. Such forward-looking statements are subject to risks, uncertainties, and other factors which could cause actual results to differ materially from those expressed or implied by such forward looking statements. These forward-looking statements are based upon estimates and assumptions that, while considered reasonable by Tango and its management at the time of this presentation, are inherently uncertain. New risks and uncertainties may emerge from time to time, and it is not possible to predict all risks and uncertainties. Factors that may cause actual results to differ materially from current expectations include, but are not limited to: the benefits of product candidates seen in preclinical tests and analyses may not be evident when tested in later preclinical studies or in clinical trials or when used in broader patient populations (if approved for commercial sale); future clinical trial data releases may differ materially from initial or interim data from our current and future clinical trials; Tango has limited experience with conducting clinical trials (and does and will rely on third parties to operate its clinical trials) and may not be able to commence or progress its clinical trials when expected, may not be able to continue dosing, initiate dose escalation and/or dose expansion on anticipated timelines, and may not generate or report clinical trial results (including final, initial, interim, updated clinical trial results or additional safety and efficacy data and the establishment of proof-of-mechanism and proof-of-concept) in the anticipated timeframe (or at all); Tango's pipeline products may not be safe and/or effective in humans; Tango may utilize cash resources more quickly than anticipated; Tango will need to raise capital in the future and if it is unable to raise capital when needed or on attractive terms, Tango would be forced to delay, reduce, or eliminate or discontinue some development programs or future commercialization efforts (which may delay filing of INDs, dosing patients, initiation of dose expansion, reporting clinical trial results and filing new drug applications); the expected benefits of Tango’s product candidates in patients as single agents and/or in combination may not be realized; Tango may experience delays or difficulties in the initiation, enrollment, or dosing of patients in clinical trials or the announcement of initial, interim, or final clinical trial results; Tango’s product candidates may cause adverse or other undesirable side effects (or may not show requisite efficacy) that could, among other things, delay or prevent regulatory approval; Tango’s dependence on or a limited number third parties for conducting clinical trials and supplying and producing drug substance and drug product (including drug substance, which is currently sole sourced); government regulation may negatively impact Tango's business, including the potential approval of the BIOSECURE Act; the impact of trade restrictions such as sanctions, tariffs, reciprocal and retaliatory tariffs, legal actions or enforcement and inflation rates on our business, financial condition, and results of operations; inadequate funding for or disruptions at the U.S. Food and Drug Administration or other government agencies may slow the time necessary for new drugs to be reviewed and/or approved or prevent these agencies from performing business functions on which the operation of our business may rely (which could negatively impact our business). Additional information concerning risks, uncertainties and assumptions can be found in Tango’s filings with the SEC, including the risk factors referenced in Tango’s Annual Report on Form 10-K for the year ended December 31, 2025, as may be supplemented and/or modified by its most recent Quarterly Report on Form 10-Q. You should not place undue reliance on forward-looking statements in this presentation, which speak only as of the date they are made and are qualified in their entirety by reference to the cautionary statements herein. Tango specifically disclaims any duty to update these forward- looking statements. Certain information contained in this Presentation relates to or is based on studies, publications, surveys and Tango’s own internal estimates and research. In addition, market data included in this presentation involve assumptions and limitations, and there can be no guarantee as to the accuracy or reliability of such assumption. Finally, while Tango believe its internal research is reliable, such research has not been verified by any independent source.
Agenda for today Leader in PRMT5 targeted therapy for cancer Malte Peters, MD | President and Chief Executive Officer Vopimetostat + RAS(ON) combination data show transformative potential in pancreatic cancer Brian Wolpin, MD | Dana-Farber Cancer Institute & Harvard Medical School Malte Peters, MD Brian Wolpin, MD Strategy to accelerate registration-directed development of vopimetostat Adam Crystal, MD PhD | President of Research and Development Capital allocation plan and financial highlights Matthew Gall | Chief Financial Officer Closing remarks Malte Peters, MD | President and Chief Executive Officer Adam Crystal, MD PhD Matthew Gall Q&A All 3

Leader in PRMT5 targeted therapy for cancer Malte Peters, MD, President and Chief Executive Officer 4
At the forefront of transformative shift in pancreatic cancer treatment Clear strategy Transformative Scientific leader for front line development 92% ORR in 2/3L PDAC in PRMT5 inhibition with chemotherapy free in combination with daraxonrasib regimen Near-term focus on potential blockbuster PDAC opportunity Pipeline supporting data-driven indication expansion to drive long-term growth PDAC, pancreatic ductal adenocarcinoma; 2/3L, second/third line. Data from ongoing Phase 1/2 clinical trial. Data as of 28 May 2026. 5
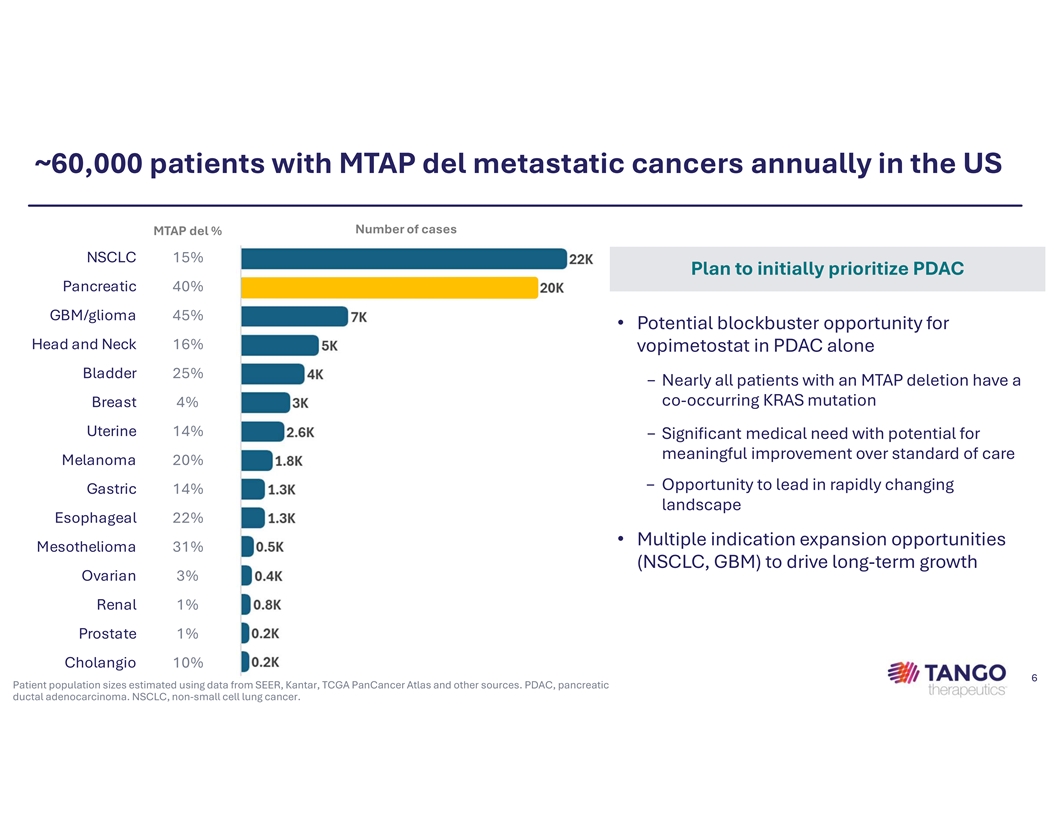
~60,000 patients with MTAP del metastatic cancers annually in the US Number of cases MTAP del % NSCLC 15% Plan to initially prioritize PDAC Pancreatic 40% GBM/glioma 45% • Potential blockbuster opportunity for Head and Neck 16% vopimetostat in PDAC alone Bladder 25% − Nearly all patients with an MTAP deletion have a co-occurring KRAS mutation Breast 4% Uterine 14% − Significant medical need with potential for meaningful improvement over standard of care Melanoma 20% − Opportunity to lead in rapidly changing Gastric 14% landscape Esophageal 22% • Multiple indication expansion opportunities Mesothelioma 31% (NSCLC, GBM) to drive long-term growth Ovarian 3% Renal 1% Prostate 1% Cholangio 10% 6 Patient population sizes estimated using data from SEER, Kantar, TCGA PanCancer Atlas and other sources. PDAC, pancreatic ductal adenocarcinoma. NSCLC, non-small cell lung cancer.

Brian Wolpin is a leader in the study and treatment of pancreatic cancer v Professor of Medicine, Harvard Medical School v Robert T. & Judith B. Hale Chair in Pancreatic Cancer, Dana-Farber Cancer Institute v Director, Hale Family Center for Pancreatic Cancer Research and Gastrointestinal Cancer Center, Dana-Farber Cancer Institute v Director, Dana-Farber – Lustgarten Foundation Dedicated Laboratory for Pancreatic Cancer Research v Medical oncologist with clinical specialty in pancreatic cancer v Research laboratory dedicated to the investigation of pancreatic ductal adenocarcinoma (PDAC) biology and treatment 7
Vopimetostat + RAS(ON) combination data show transformative potential in pancreatic cancer Dr. Brian Wolpin, MD, MPH Dana-Farber Cancer Institute & Harvard Medical School 8
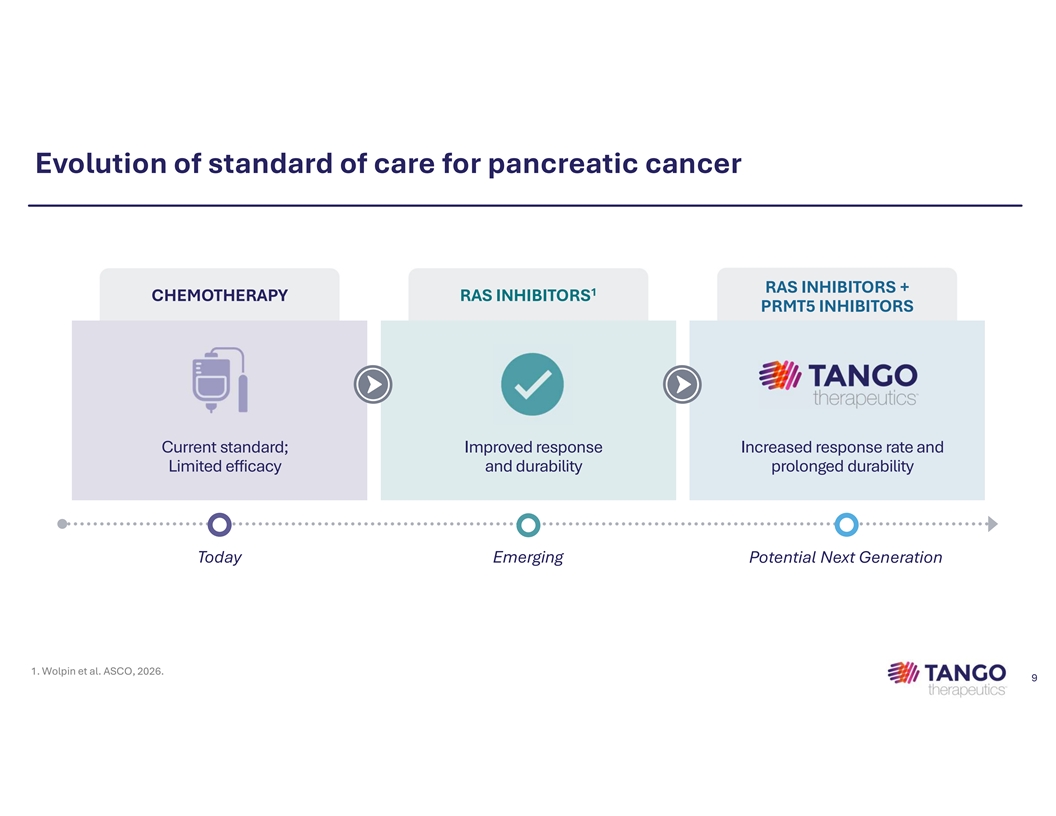
Evolution of standard of care for pancreatic cancer RAS INHIBITORS + 1 CHEMOTHERAPY RAS INHIBITORS PRMT5 INHIBITORS Current standard; Improved response Increased response rate and Limited efficacy and durability prolonged durability Today Emerging Potential Next Generation 1. Wolpin et al. ASCO, 2026. 9
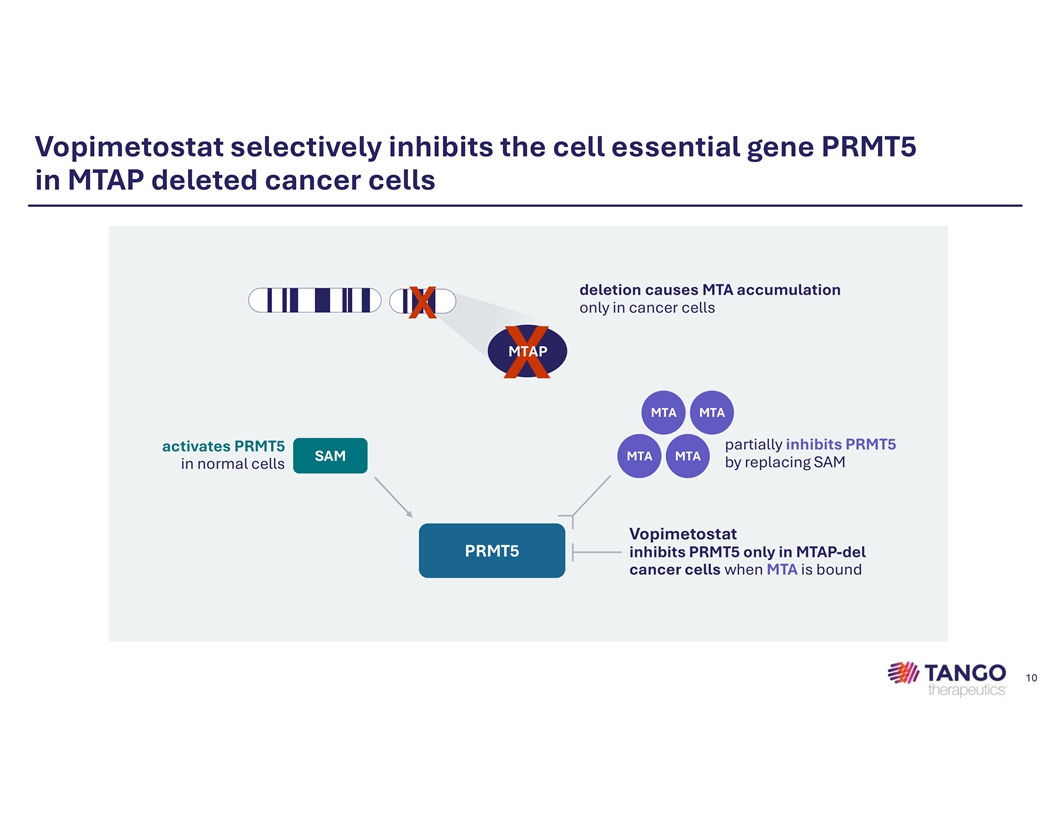
Vopimetostat selectively inhibits the cell essential gene PRMT5 in MTAP deleted cancer cells deletion causes MTA accumulation only in cancer cells X MTAP X MTA MTA partially inhibits PRMT5 activates PRMT5 MTA MTA SAM by replacing SAM in normal cells Vopimetostat PRMT5 inhibits PRMT5 only in MTAP-del cancer cells when MTA is bound 10
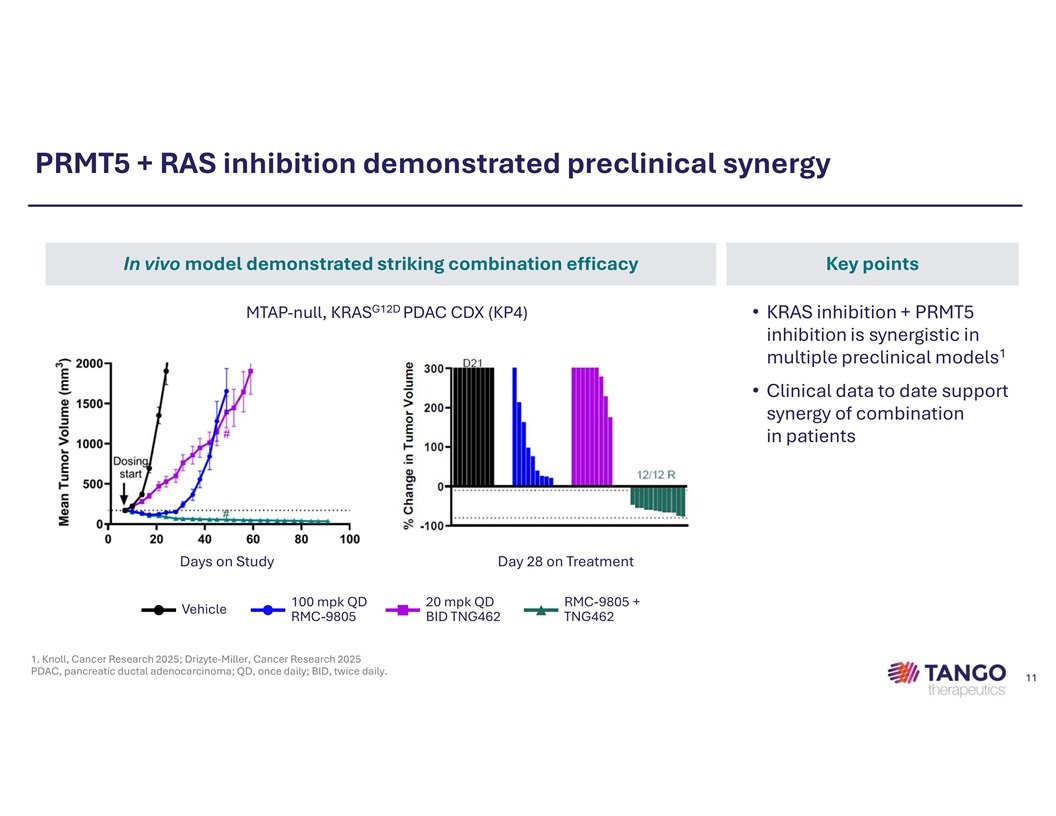
PRMT5 + RAS inhibition demonstrated preclinical synergy In vivo model demonstrated striking combination efficacy Key points G12D MTAP-null, KRAS PDAC CDX (KP4) • KRAS inhibition + PRMT5 inhibition is synergistic in 1 multiple preclinical models • Clinical data to date support synergy of combination in patients Days on Study Day 28 on Treatment 100 mpk QD 20 mpk QD RMC-9805 + Vehicle RMC-9805 BID TNG462 TNG462 1. Knoll, Cancer Research 2025; Drizyte-Miller, Cancer Research 2025 PDAC, pancreatic ductal adenocarcinoma; QD, once daily; BID, twice daily. 11
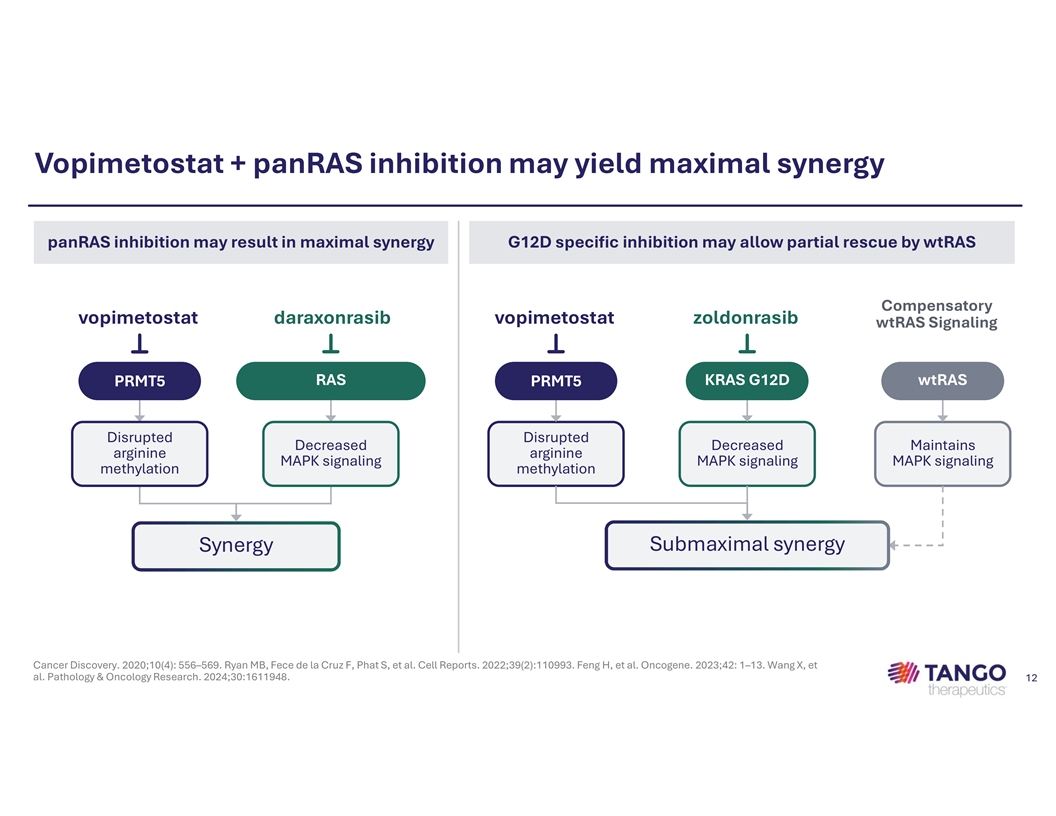
Vopimetostat + panRAS inhibition may yield maximal synergy panRAS inhibition may result in maximal synergy G12D specific inhibition may allow partial rescue by wtRAS Compensatory vopimetostat daraxonrasib vopimetostat zoldonrasib wtRAS Signaling RAS KRAS G12D wtRAS PRMT5 PRMT5 Disrupted Disrupted Decreased Decreased Maintains arginine arginine MAPK signaling MAPK signaling MAPK signaling methylation methylation Submaximal synergy Synergy Cancer Discovery. 2020;10(4): 556–569. Ryan MB, Fece de la Cruz F, Phat S, et al. Cell Reports. 2022;39(2):110993. Feng H, et al. Oncogene. 2023;42: 1–13. Wang X, et al. Pathology & Oncology Research. 2024;30:1611948. 12
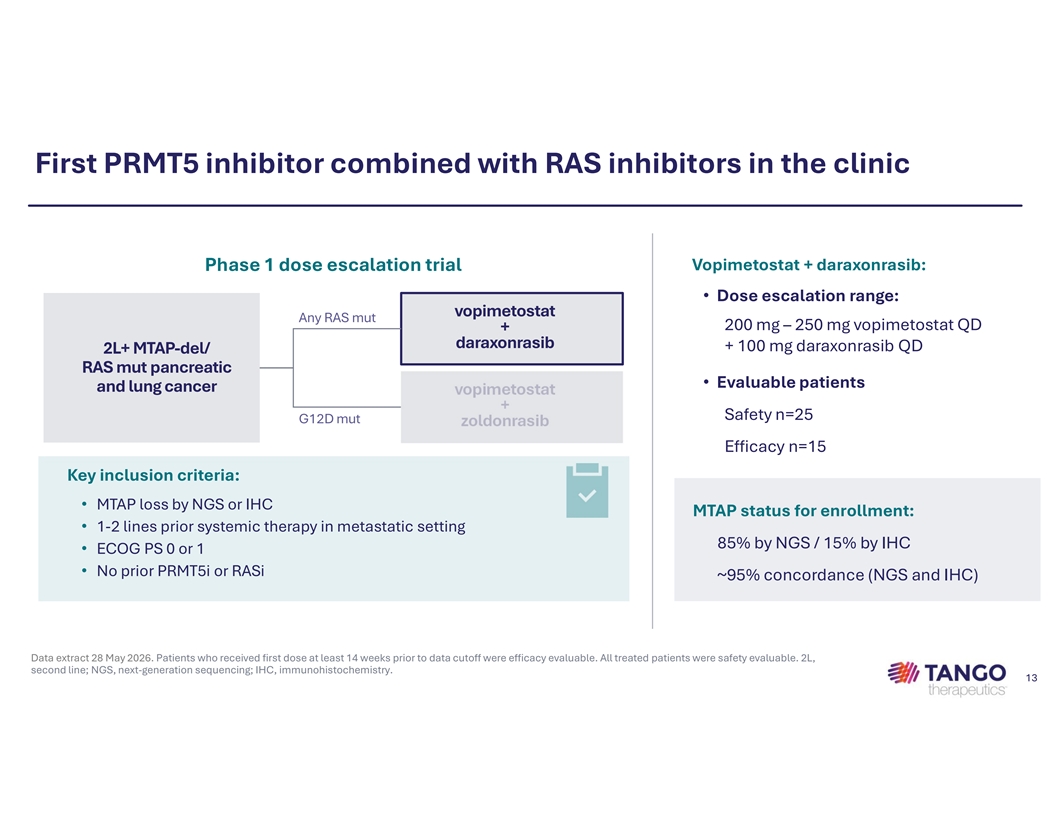
First PRMT5 inhibitor combined with RAS inhibitors in the clinic Phase 1 dose escalation trial Vopimetostat + daraxonrasib: • Dose escalation range: vopimetostat Any RAS mut 200 mg – 250 mg vopimetostat QD + daraxonrasib + 100 mg daraxonrasib QD 2L+ MTAP-del/ RAS mut pancreatic • Evaluable patients and lung cancer vopimetostat + Safety n=25 G12D mut zoldonrasib Efficacy n=15 Key inclusion criteria: • MTAP loss by NGS or IHC MTAP status for enrollment: • 1-2 lines prior systemic therapy in metastatic setting 85% by NGS / 15% by IHC • ECOG PS 0 or 1 • No prior PRMT5i or RASi ~95% concordance (NGS and IHC) Data extract 28 May 2026. Patients who received first dose at least 14 weeks prior to data cutoff were efficacy evaluable. All treated patients were safety evaluable. 2L, second line; NGS, next-generation sequencing; IHC, immunohistochemistry. 13
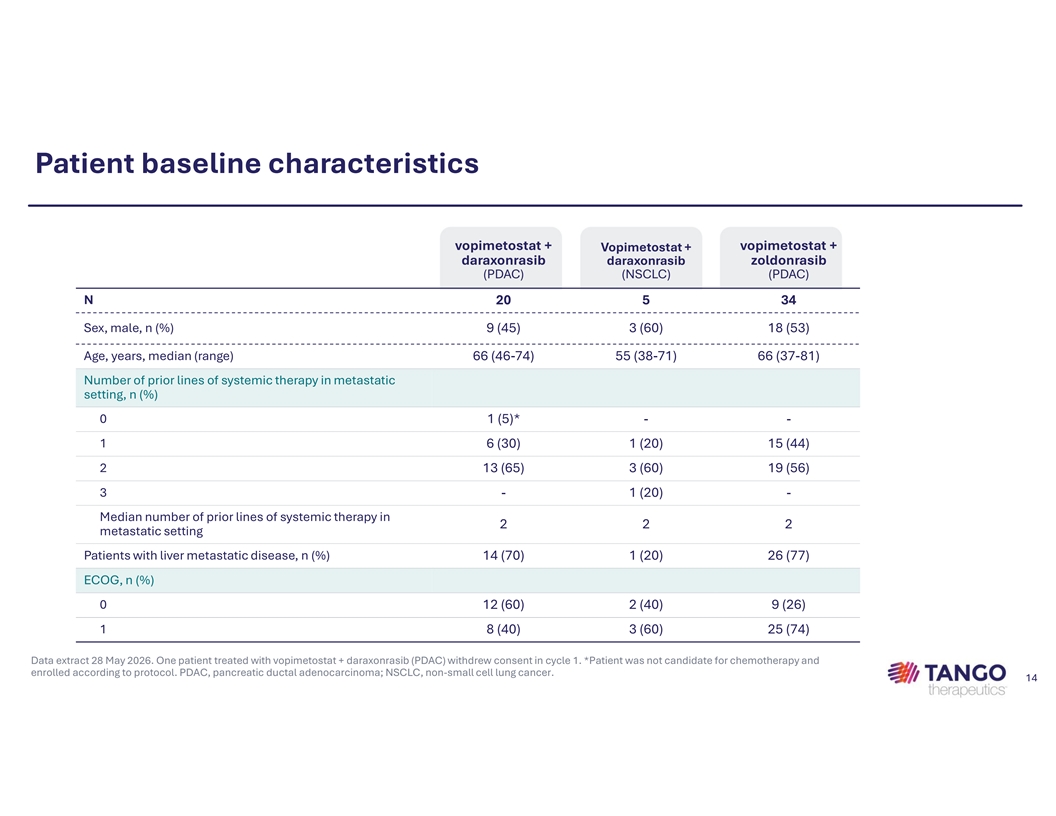
Patient baseline characteristics vopimetostat + vopimetostat + Vopimetostat + daraxonrasib daraxonrasib zoldonrasib (PDAC) (NSCLC) (PDAC) N 20 5 34 Sex, male, n (%) 9 (45) 3 (60) 18 (53) Age, years, median (range) 66 (46-74) 55 (38-71) 66 (37-81) Number of prior lines of systemic therapy in metastatic setting, n (%) 0 1 (5)* - - 1 6 (30) 1 (20) 15 (44) 2 13 (65) 3 (60) 19 (56) 3 - 1 (20) - Median number of prior lines of systemic therapy in 2 2 2 metastatic setting Patients with liver metastatic disease, n (%) 14 (70) 1 (20) 26 (77) ECOG, n (%) 0 12 (60) 2 (40) 9 (26) 1 8 (40) 3 (60) 25 (74) Data extract 28 May 2026. One patient treated with vopimetostat + daraxonrasib (PDAC) withdrew consent in cycle 1. *Patient was not candidate for chemotherapy and enrolled according to protocol. PDAC, pancreatic ductal adenocarcinoma; NSCLC, non-small cell lung cancer. 14
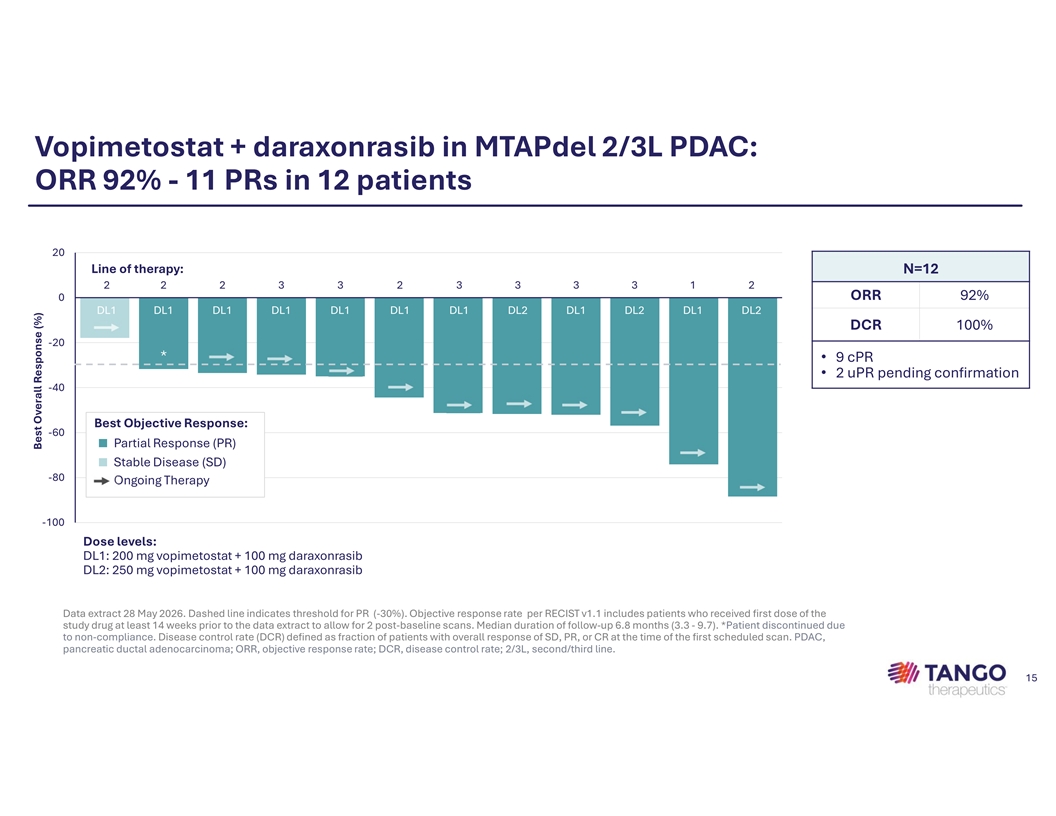
Vopimetostat + daraxonrasib in MTAPdel 2/3L PDAC: ORR 92% - 11 PRs in 12 patients 20 Line of therapy: N=12 2 2 2 3 3 2 3 3 3 3 1 2 ORR 92% 0 DL1 DL1 DL1 DL1 DL1 DL1 DL1 DL2 DL1 DL2 DL1 DL2 DCR 100% -20 * • 9 cPR • 2 uPR pending confirmation -40 Best Objective Response: -60 ■ Partial Response (PR) ■ Stable Disease (SD) -80 Ongoing Therapy -100 Dose levels: DL1: 200 mg vopimetostat + 100 mg daraxonrasib DL2: 250 mg vopimetostat + 100 mg daraxonrasib Data extract 28 May 2026. Dashed line indicates threshold for PR (-30%). Objective response rate per RECIST v1.1 includes patients who received first dose of the study drug at least 14 weeks prior to the data extract to allow for 2 post-baseline scans. Median duration of follow-up 6.8 months (3.3 - 9.7). *Patient discontinued due to non-compliance. Disease control rate (DCR) defined as fraction of patients with overall response of SD, PR, or CR at the time of the first scheduled scan. PDAC, pancreatic ductal adenocarcinoma; ORR, objective response rate; DCR, disease control rate; 2/3L, second/third line. 15 Best Overall Response (%)
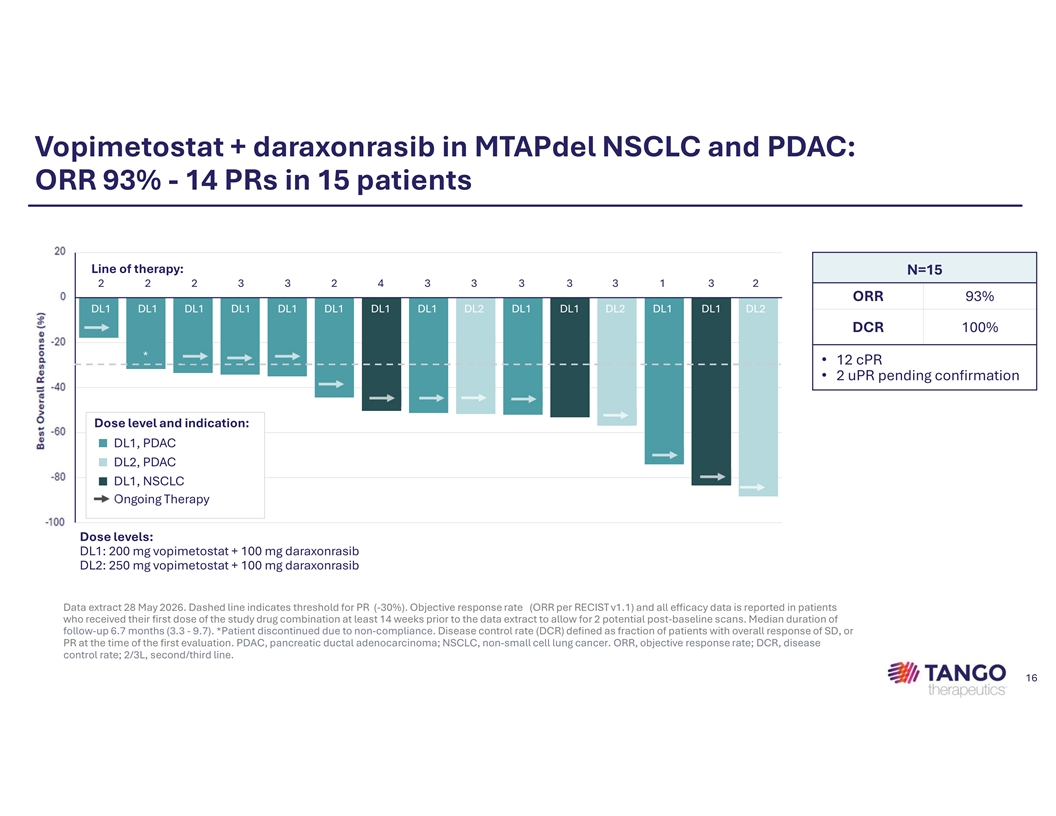
Vopimetostat + daraxonrasib in MTAPdel NSCLC and PDAC: ORR 93% - 14 PRs in 15 patients 20.0 Line of therapy: N=15 2 2 2 3 3 2 4 3 3 3 3 3 1 3 2 .0 ORR 93% DL1 DL1 DL1 DL1 DL1 DL1 DL1 DL1 DL2 DL1 DL1 DL2 DL1 DL1 DL2 DCR 100% -20.0 * • 12 cPR • 2 uPR pending confirmation -40.0 Dose level and indication: -60.0 ■ DL1, PDAC ■ DL2, PDAC -80.0 ■ DL1, NSCLC Ongoing Therapy -100.0 Dose levels: DL1: 200 mg vopimetostat + 100 mg daraxonrasib DL2: 250 mg vopimetostat + 100 mg daraxonrasib Data extract 28 May 2026. Dashed line indicates threshold for PR (-30%). Objective response rate (ORR per RECIST v1.1) and all efficacy data is reported in patients who received their first dose of the study drug combination at least 14 weeks prior to the data extract to allow for 2 potential post-baseline scans. Median duration of follow-up 6.7 months (3.3 - 9.7). *Patient discontinued due to non-compliance. Disease control rate (DCR) defined as fraction of patients with overall response of SD, or PR at the time of the first evaluation. PDAC, pancreatic ductal adenocarcinoma; NSCLC, non-small cell lung cancer. ORR, objective response rate; DCR, disease control rate; 2/3L, second/third line. 16 Best Overall Response (%)
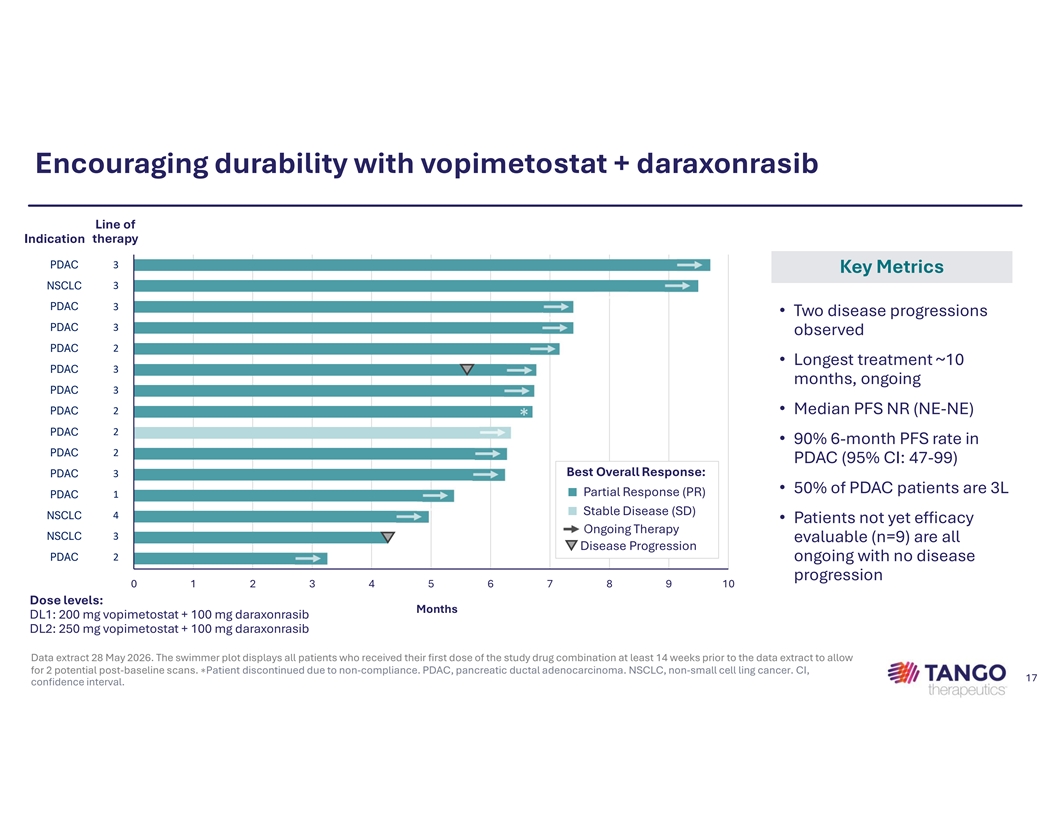
Encouraging durability with vopimetostat + daraxonrasib Line of Indication therapy PDAC3 Key Metrics NSCLC3 PDAC3 • Two disease progressions 3 PDAC observed PDAC2 • Longest treatment ~10 PDAC3 months, ongoing 3 PDAC PDAC2 • Median PFS NR (NE-NE) ∗ PDAC2 • 90% 6-month PFS rate in PDAC2 PDAC (95% CI: 47-99) Best Overall Response: PDAC3 • 50% of PDAC patients are 3L ■ Partial Response (PR) PDAC1 ■ Stable Disease (SD) 4 NSCLC • Patients not yet efficacy Ongoing Therapy * NSCLC3 evaluable (n=9) are all Disease Progression PDAC2 ongoing with no disease progression 0 1 2 3 4 5 6 7 8 9 10 Dose levels: Months DL1: 200 mg vopimetostat + 100 mg daraxonrasib DL2: 250 mg vopimetostat + 100 mg daraxonrasib Data extract 28 May 2026. The swimmer plot displays all patients who received their first dose of the study drug combination at least 14 weeks prior to the data extract to allow for 2 potential post-baseline scans. ∗Patient discontinued due to non-compliance. PDAC, pancreatic ductal adenocarcinoma. NSCLC, non-small cell ling cancer. CI, 17 confidence interval.
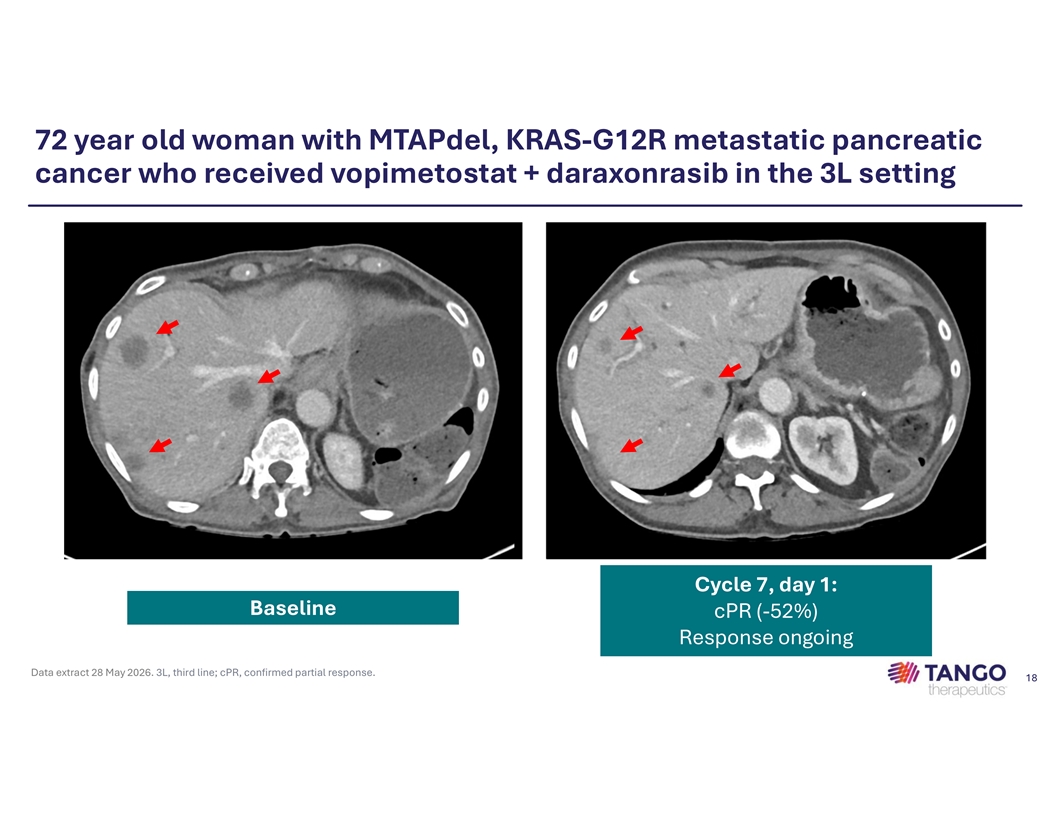
72 year old woman with MTAPdel, KRAS-G12R metastatic pancreatic cancer who received vopimetostat + daraxonrasib in the 3L setting Cycle 7, day 1: Baseline cPR (-52%) Response ongoing Data extract 28 May 2026. 3L, third line; cPR, confirmed partial response. 18
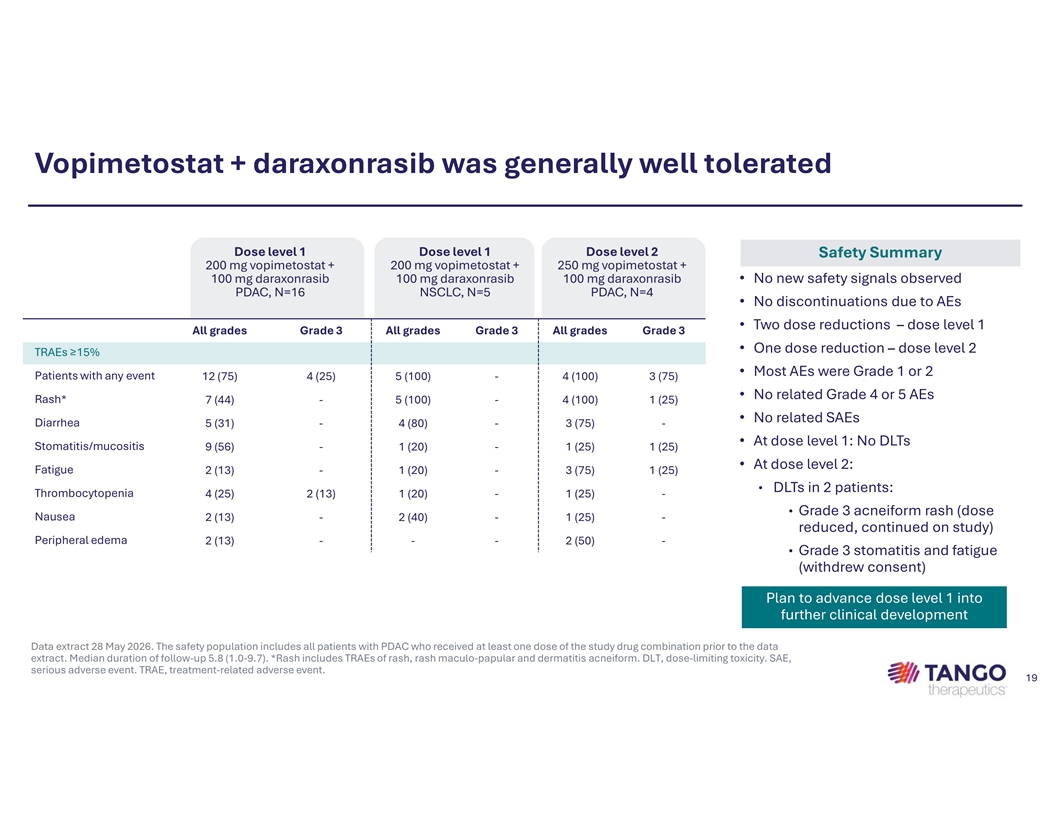
Vopimetostat + daraxonrasib was generally well tolerated Dose level 1 Dose level 1 Dose level 2 Safety Summary 200 mg vopimetostat + 200 mg vopimetostat + 250 mg vopimetostat + 100 mg daraxonrasib 100 mg daraxonrasib 100 mg daraxonrasib • No new safety signals observed PDAC, N=16 NSCLC, N=5 PDAC, N=4 • No discontinuations due to AEs • Two dose reductions – dose level 1 All grades Grade 3 All grades Grade 3 All grades Grade 3 • One dose reduction – dose level 2 TRAEs ≥15% • Most AEs were Grade 1 or 2 Patients with any event 12 (75) 4 (25) 5 (100) - 4 (100) 3 (75) • No related Grade 4 or 5 AEs Rash* 7 (44) - 5 (100) - 4 (100) 1 (25) • No related SAEs Diarrhea 5 (31) - 4 (80) - 3 (75) - • At dose level 1: No DLTs Stomatitis/mucositis 9 (56) - 1 (20) - 1 (25) 1 (25) • At dose level 2: Fatigue 2 (13) - 1 (20) - 3 (75) 1 (25) • DLTs in 2 patients: Thrombocytopenia 4 (25) 2 (13) 1 (20) - 1 (25) - • Grade 3 acneiform rash (dose Nausea 2 (13) - 2 (40) - 1 (25) - reduced, continued on study) Peripheral edema 2 (13) - - - 2 (50) - • Grade 3 stomatitis and fatigue (withdrew consent) Plan to advance dose level 1 into further clinical development Data extract 28 May 2026. The safety population includes all patients with PDAC who received at least one dose of the study drug combination prior to the data extract. Median duration of follow-up 5.8 (1.0-9.7). *Rash includes TRAEs of rash, rash maculo-papular and dermatitis acneiform. DLT, dose-limiting toxicity. SAE, serious adverse event. TRAE, treatment-related adverse event. 19
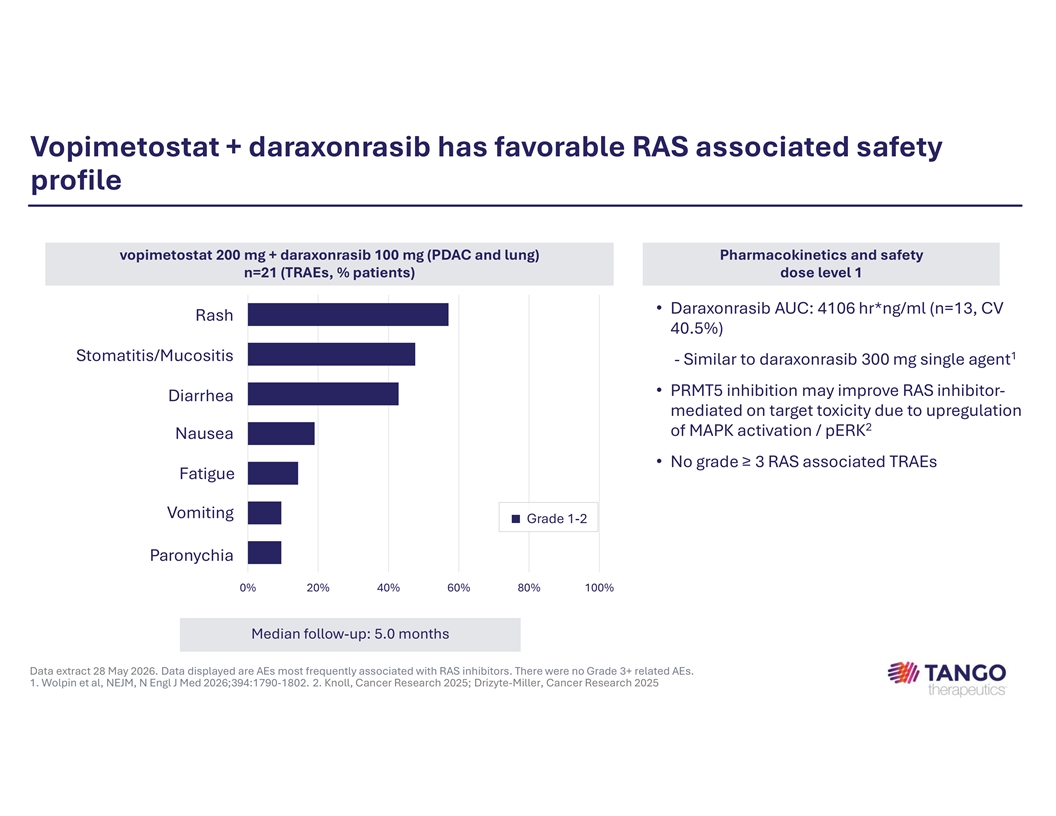
Vopimetostat + daraxonrasib has favorable RAS associated safety profile vopimetostat 200 mg + daraxonrasib 100 mg (PDAC and lung) Pharmacokinetics and safety n=21 (TRAEs, % patients) dose level 1 • Daraxonrasib AUC: 4106 hr*ng/ml (n=13, CV Rash 40.5%) 1 Stomatitis/Mucositis - Similar to daraxonrasib 300 mg single agent • PRMT5 inhibition may improve RAS inhibitor- Diarrhea mediated on target toxicity due to upregulation 2 of MAPK activation / pERK Nausea • No grade ≥ 3 RAS associated TRAEs Fatigue Vomiting ■ Grade 1-2 Paronychia 0% 20% 40% 60% 80% 100% Median follow-up: 5.0 months Data extract 28 May 2026. Data displayed are AEs most frequently associated with RAS inhibitors. There were no Grade 3+ related AEs. 1. Wolpin et al, NEJM, N Engl J Med 2026;394:1790-1802. 2. Knoll, Cancer Research 2025; Drizyte-Miller, Cancer Research 2025
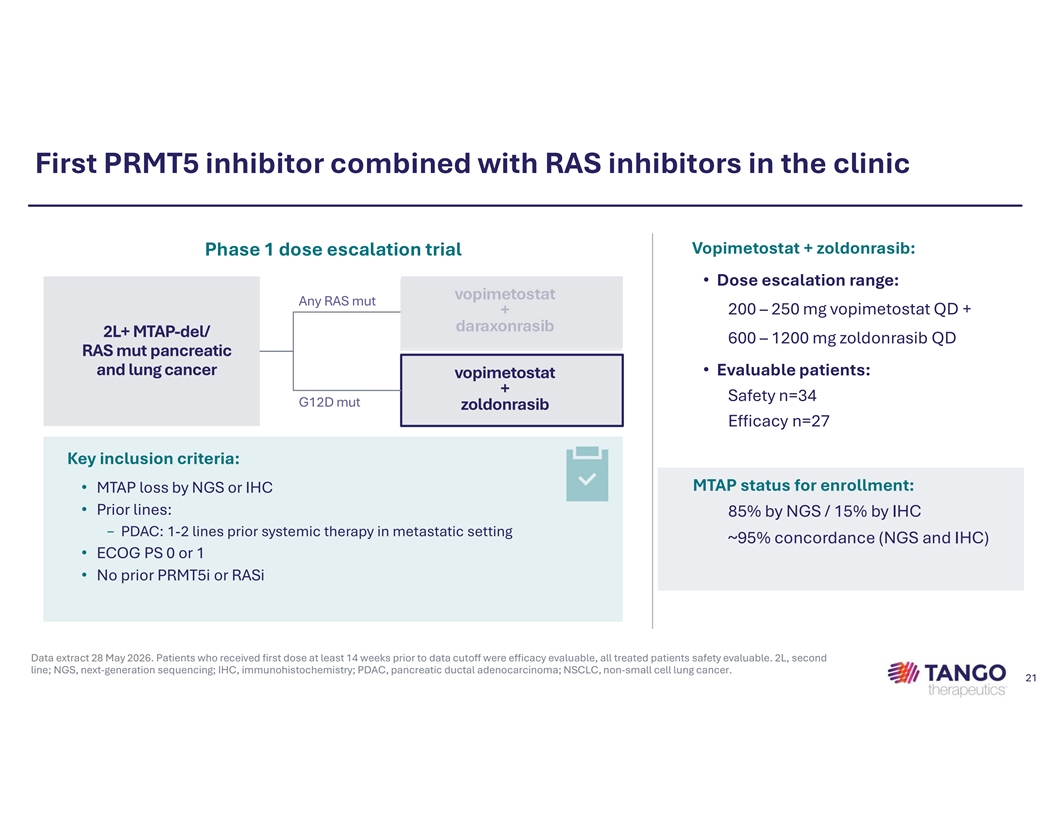
First PRMT5 inhibitor combined with RAS inhibitors in the clinic Vopimetostat + zoldonrasib: Phase 1 dose escalation trial • Dose escalation range: vopimetostat Any RAS mut 200 – 250 mg vopimetostat QD + + daraxonrasib 2L+ MTAP-del/ 600 – 1200 mg zoldonrasib QD RAS mut pancreatic and lung cancer • Evaluable patients: vopimetostat + Safety n=34 G12D mut zoldonrasib Efficacy n=27 Key inclusion criteria: MTAP status for enrollment: • MTAP loss by NGS or IHC • Prior lines: 85% by NGS / 15% by IHC − PDAC: 1-2 lines prior systemic therapy in metastatic setting ~95% concordance (NGS and IHC) • ECOG PS 0 or 1 • No prior PRMT5i or RASi Data extract 28 May 2026. Patients who received first dose at least 14 weeks prior to data cutoff were efficacy evaluable, all treated patients safety evaluable. 2L, second line; NGS, next-generation sequencing; IHC, immunohistochemistry; PDAC, pancreatic ductal adenocarcinoma; NSCLC, non-small cell lung cancer. 21
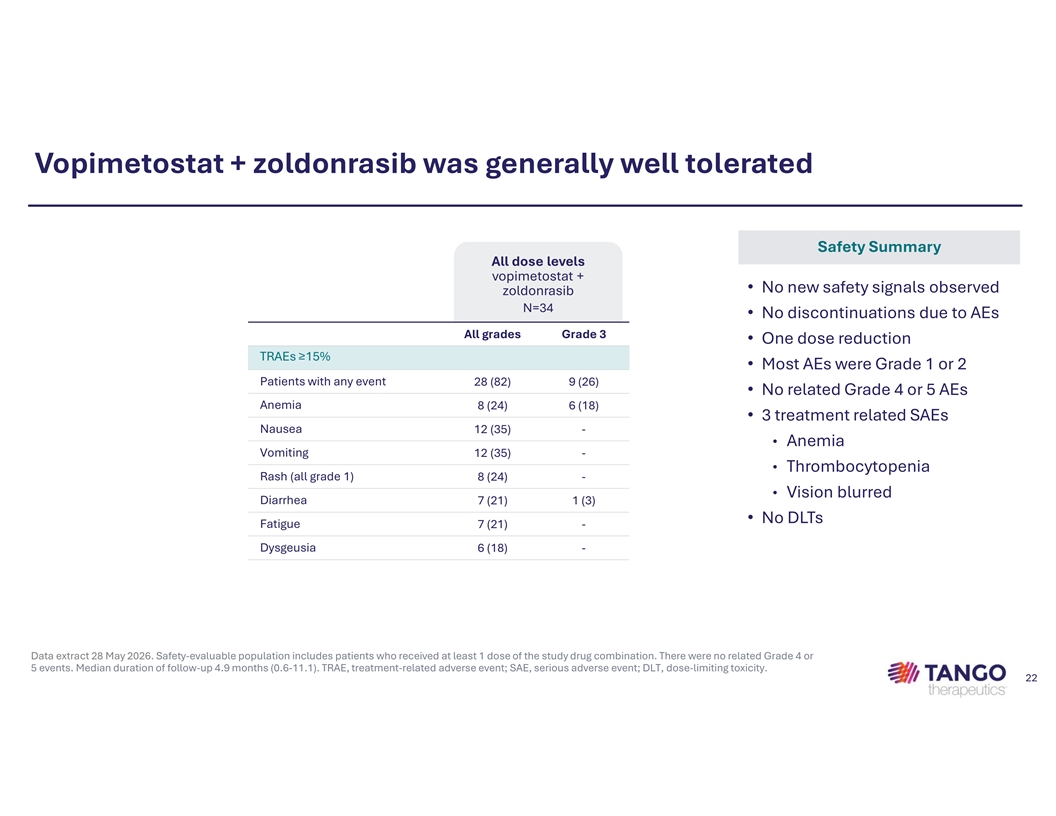
Vopimetostat + zoldonrasib was generally well tolerated Safety Summary All dose levels vopimetostat + • No new safety signals observed zoldonrasib N=34 • No discontinuations due to AEs All grades Grade 3 • One dose reduction TRAEs ≥15% • Most AEs were Grade 1 or 2 Patients with any event 28 (82) 9 (26) • No related Grade 4 or 5 AEs Anemia 8 (24) 6 (18) • 3 treatment related SAEs Nausea 12 (35) - • Anemia Vomiting 12 (35) - • Thrombocytopenia Rash (all grade 1) 8 (24) - • Vision blurred Diarrhea 7 (21) 1 (3) • No DLTs Fatigue 7 (21) - Dysgeusia 6 (18) - Data extract 28 May 2026. Safety-evaluable population includes patients who received at least 1 dose of the study drug combination. There were no related Grade 4 or 5 events. Median duration of follow-up 4.9 months (0.6-11.1). TRAE, treatment-related adverse event; SAE, serious adverse event; DLT, dose-limiting toxicity. 22
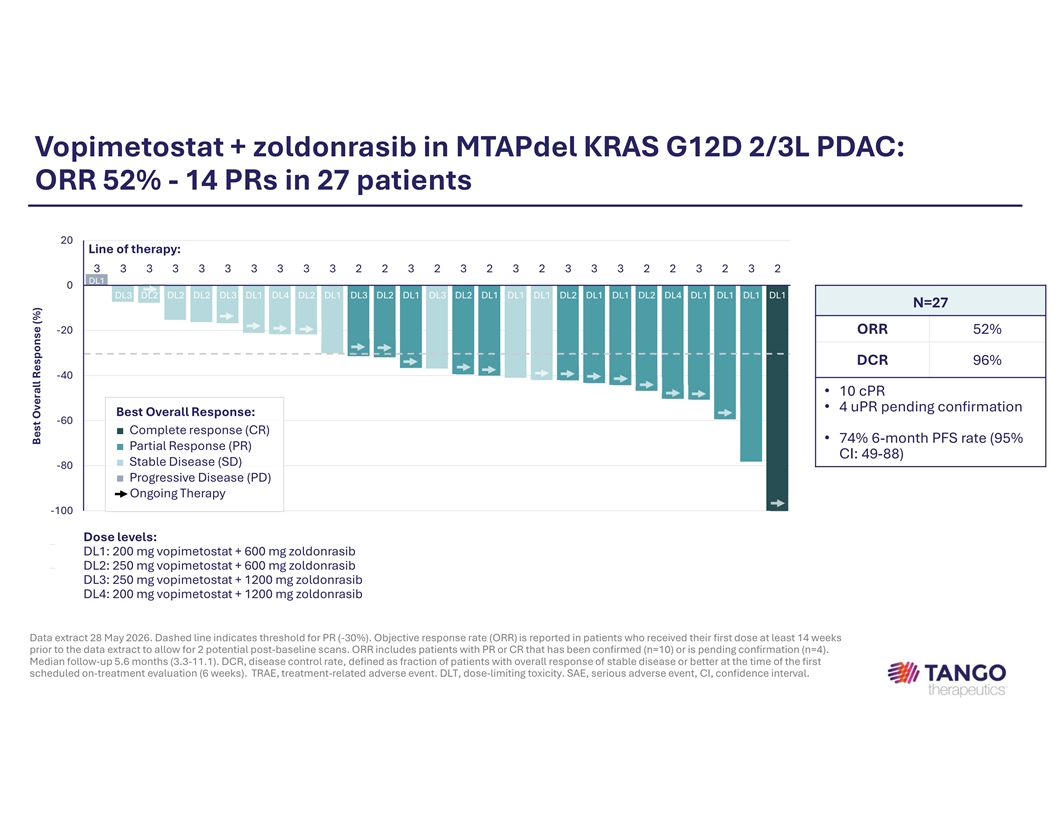
Vopimetostat + zoldonrasib in MTAPdel KRAS G12D 2/3L PDAC: ORR 52% - 14 PRs in 27 patients 20 Line of therapy: 3 3 3 3 3 3 3 3 3 3 2 2 3 2 3 2 3 2 3 3 3 2 2 3 2 3 2 DL1 0 DL3 DL2 DL2 DL2 DL3 DL1 DL4 DL2 DL1 DL3 DL2 DL1 DL3 DL2 DL1 DL1 DL1 DL2 DL1 DL1 DL2 DL4 DL1 DL1 DL1 DL1 N=27 -20 ORR 52% DCR 96% -40 • 10 cPR • 4 uPR pending confirmation Best Overall Response: -60 ■ Complete response (CR) • 74% 6-month PFS rate (95% ■ Partial Response (PR) CI: 49-88) ■ Stable Disease (SD) -80 ■ Progressive Disease (PD) Ongoing Therapy -100 DL DL2 DL2 DL2 DL1 DL2 DL1 DL1 DL1 DL2 DL1 DL1 DL1 DL2 DL1 DL1 DL1 Dose levels: DL1: 200 mg vopimetostat + 600 mg zoldonrasib LoT 3 3 2 3 3 3 3 2 3 3 3 2 2 2 3 2 DL2: 250 mg vopimetostat + 600 mg zoldonrasib DL3: 250 mg vopimetostat + 1200 mg zoldonrasib DL4: 200 mg vopimetostat + 1200 mg zoldonrasib Data extract 28 May 2026. Dashed line indicates threshold for PR (-30%). Objective response rate (ORR) is reported in patients who received their first dose at least 14 weeks prior to the data extract to allow for 2 potential post-baseline scans. ORR includes patients with PR or CR that has been confirmed (n=10) or is pending confirmation (n=4). Median follow-up 5.6 months (3.3-11.1). DCR, disease control rate, defined as fraction of patients with overall response of stable disease or better at the time of the first scheduled on-treatment evaluation (6 weeks). TRAE, treatment-related adverse event. DLT, dose-limiting toxicity. SAE, serious adverse event, CI, confidence interval. Best Overall Response (%)
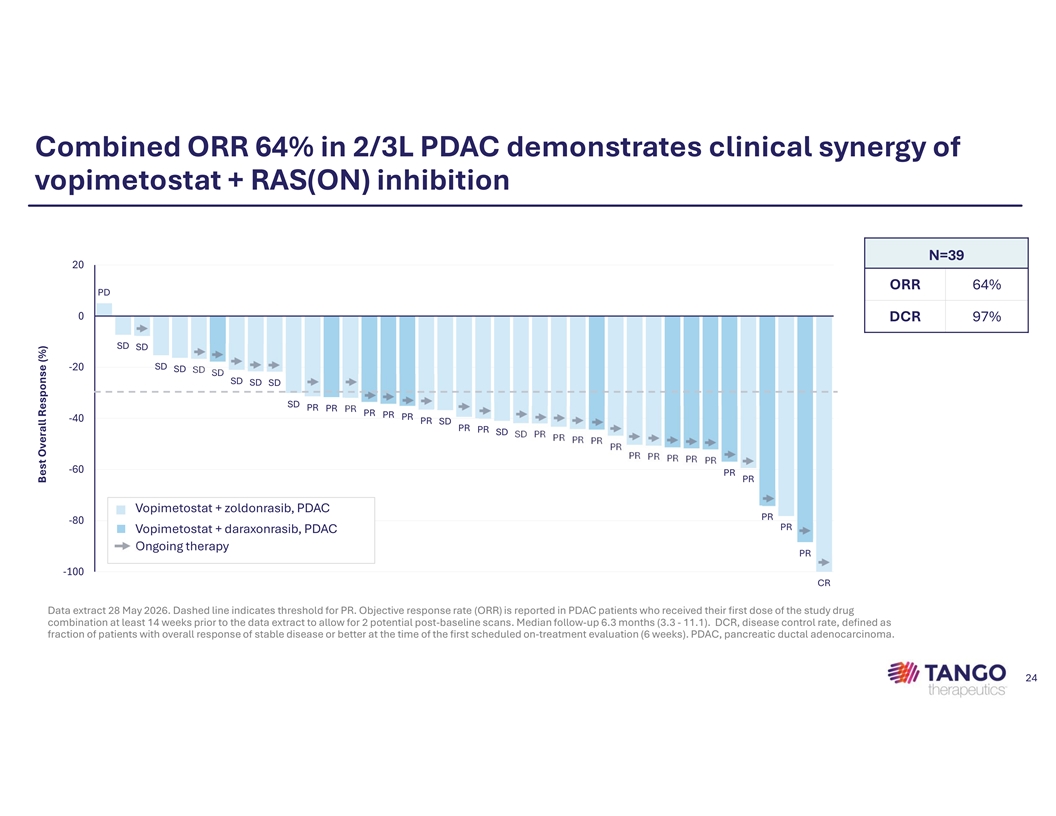
Combined ORR 64% in 2/3L PDAC demonstrates clinical synergy of vopimetostat + RAS(ON) inhibition N=39 20 ORR 64% PD 0 DCR 97% SD SD SD -20 SD SD SD SD SD SD SD PR PR PR PR PR PR -40 PR SD PR PR SD SD PR PR PR PR PR PR PR PR PR PR -60 PR PR Vopimetostat + zoldonrasib, PDAC PR -80 PR ■ Vopimetostat + daraxonrasib, PDAC Ongoing therapy PR -100 CR Data extract 28 May 2026. Dashed line indicates threshold for PR. Objective response rate (ORR) is reported in PDAC patients who received their first dose of the study drug combination at least 14 weeks prior to the data extract to allow for 2 potential post-baseline scans. Median follow-up 6.3 months (3.3 - 11.1). DCR, disease control rate, defined as fraction of patients with overall response of stable disease or better at the time of the first scheduled on-treatment evaluation (6 weeks). PDAC, pancreatic ductal adenocarcinoma. 24 Best Overall Response (%)

Strategy to accelerate registration-directed development of vopimetostat Adam Crystal, MD PhD, President of Research and Development 25
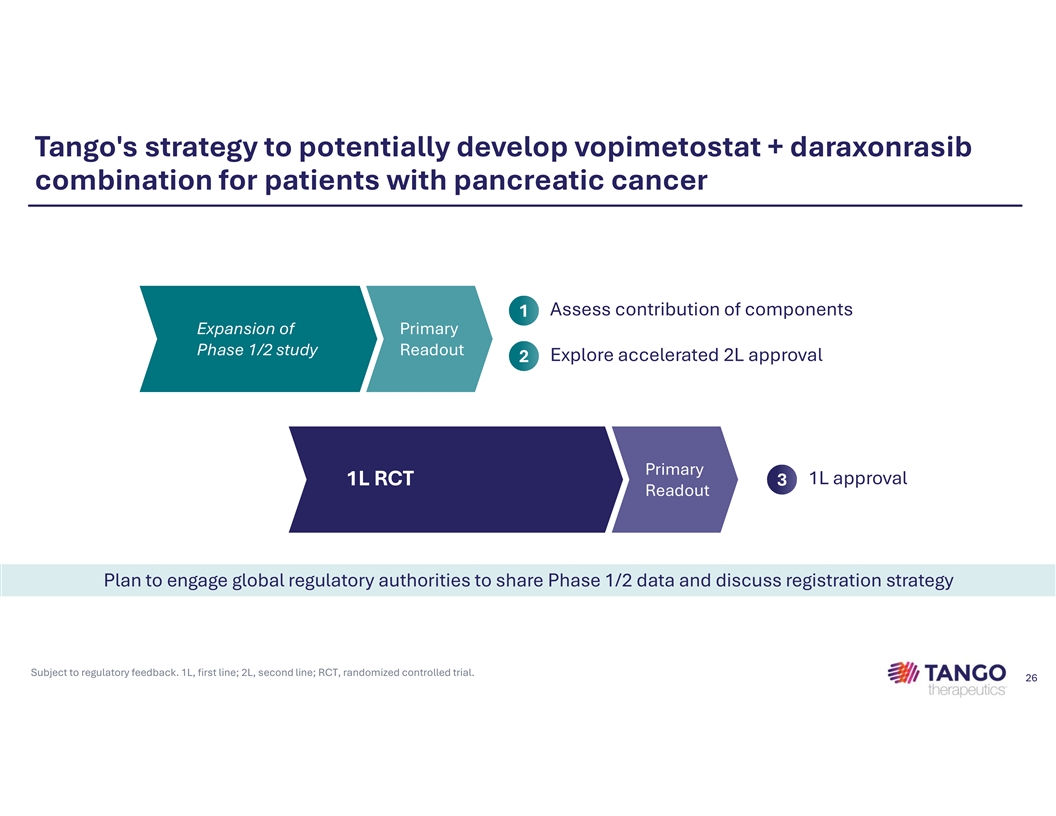
Tango's strategy to potentially develop vopimetostat + daraxonrasib combination for patients with pancreatic cancer Assess contribution of components 1 Expansion of Primary Phase 1/2 study Readout Explore accelerated 2L approval 2 Primary 1L approval 1L RCT 3 Readout Plan to engage global regulatory authorities to share Phase 1/2 data and discuss registration strategy Subject to regulatory feedback. 1L, first line; 2L, second line; RCT, randomized controlled trial. 26

Capital allocation plan and financial highlights Matthew Gall, Chief Financial Officer 27
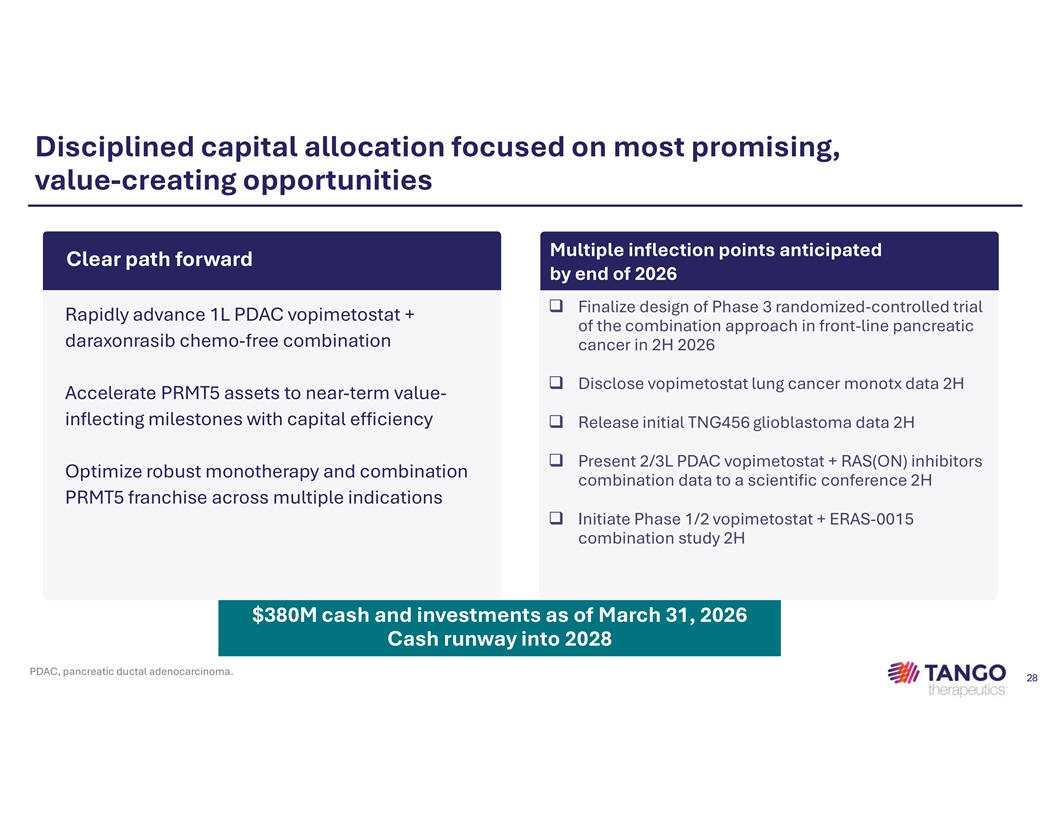
Disciplined capital allocation focused on most promising, value-creating opportunities Multiple inflection points anticipated Clear path forward by end of 2026 q Finalize design of Phase 3 randomized-controlled trial Rapidly advance 1L PDAC vopimetostat + of the combination approach in front-line pancreatic daraxonrasib chemo-free combination cancer in 2H 2026 q Disclose vopimetostat lung cancer monotx data 2H Accelerate PRMT5 assets to near-term value- inflecting milestones with capital efficiency q Release initial TNG456 glioblastoma data 2H q Present 2/3L PDAC vopimetostat + RAS(ON) inhibitors Optimize robust monotherapy and combination combination data to a scientific conference 2H PRMT5 franchise across multiple indications q Initiate Phase 1/2 vopimetostat + ERAS-0015 combination study 2H $380M cash and investments as of March 31, 2026 Cash runway into 2028 PDAC, pancreatic ductal adenocarcinoma. 28
Closing remarks Malte Peters, MD, Chief Executive Officer 29
At the forefront of transformative shift in pancreatic cancer treatment Clear strategy Transformative Scientific leader for front line development 92% ORR in 2/3L PDAC in PRMT5 inhibition with chemotherapy free in combination with daraxonrasib regimen Near-term focus on potential blockbuster PDAC opportunity Pipeline supporting data-driven indication expansion to drive long-term growth PDAC, pancreatic ductal adenocarcinoma; 2/3L, second/third line. Data from ongoing Phase 1/2 clinical trial. Data as of 28 May 2026. 30

CONFIDENTIAL