| CNTY-813: Scalable Production of Allo-Evasion 5.0- Engineered iPSC Islets for Off-the-Shelf Cell Therapies Leonardo Velazco-Cruz, PhD |
| 2 • Presenter – Leonardo Velazco-Cruz, PhD • Relevant Financial Relationship – Employee, Century Therapeutics – Stock/Shareholder: Century Therapeutics • Presentation Information: – This presentation describes preclinical research related to CNTY-813, an investigational iPSC-derived islet cell therapy for T1D – The content is intended for scientific and educational discussion – No clinical recommendations will be made Disclosures |
| 3 Forward-looking statements This presentation contains forward-looking statements within the meaning of, and made pursuant to the safe harbor provisions of, The Private Securities Litigation Reform Act of 1995. All statements contained in this presentation, other than statements of historical facts or statements that relate to present facts or current conditions, including but not limited to, statements regarding our clinical development plans and timelines and the initial safety and efficacy profiles of CNTY-813 and statements regarding our preclinical development programs, including initial preclinical data and development plans and timelines are forward-looking statements. These statements involve known and unknown risks, uncertainties and other important factors that may cause our actual results, performance, or achievements to be materially different from any future results, performance or achievements expressed or implied by the forward-looking statements. In some cases, you can identify forward-looking statements by terms such as “may,” “might,” “will,” “should,” “expect,” “plan,” “aim,” “seek,” “anticipate,” “could,” “intend,” “target,” “project,” “contemplate,” “believe,” “estimate,” “predict,” “forecast,” “potential” or “continue” or the negative of these terms or other similar expressions. The forward-looking statements in this presentation are only predictions. We have based these forward-looking statements largely on our current expectations and projections about future events and financial trends that we believe may affect our business, financial condition, and results of operations. These forward-looking statements speak only as of the date of this presentation and are subject to a number of risks, uncertainties and assumptions, some of which cannot be predicted or quantified and some of which are beyond our control, including, among others: our ability to successfully advance our current and future product candidates through development activities, preclinical studies, and clinical trials; our ability to progress CNTY-813 through clinical development; our ability to meet development milestones on anticipated timelines; uncertainties inherent in the results of preliminary data, pre-clinical studies and earlier-stage clinical trials, which may not be predictive of final results or the results of later-stage clinical trials; our ability to obtain clearance of our future IND or CTA submissions and commence and complete clinical trials on expected timelines, or at all; our reliance on the maintenance of certain key collaborative relationships for the manufacturing and development of our product candidates; the timing, scope and likelihood of regulatory filings and approvals, including final regulatory approval of our product candidates; the impact of geopolitical issues, trade disputes and tariffs, banking instability and inflation on our business and operations, supply chain and labor force; the performance of third parties in connection with the development of our product candidates, including third parties conducting our clinical trials as well as third-party suppliers and manufacturers; our ability to successfully commercialize our product candidates and develop sales and marketing capabilities, if our product candidates are approved; our ability to recruit and maintain key members of management and our ability to maintain and successfully enforce adequate intellectual property protection. These and other risks and uncertainties are described more fully in the “Risk Factors” section of our most recent filings with the Securities and Exchange Commission and available at www.sec.gov. You should not rely on these forward-looking statements as predictions of future events. The events and circumstances reflected in our forward-looking statements may not be achieved or occur, and actual results could differ materially from those projected in the forward-looking statements. Moreover, we operate in a dynamic industry and economy. New risk factors and uncertainties may emerge from time to time, and it is not possible for management to predict all risk factors and uncertainties that we may face. Except as required by applicable law, we do not plan to publicly update or revise any forward-looking statements contained herein, whether as a result of any new information, future events, changed circumstances or otherwise. |
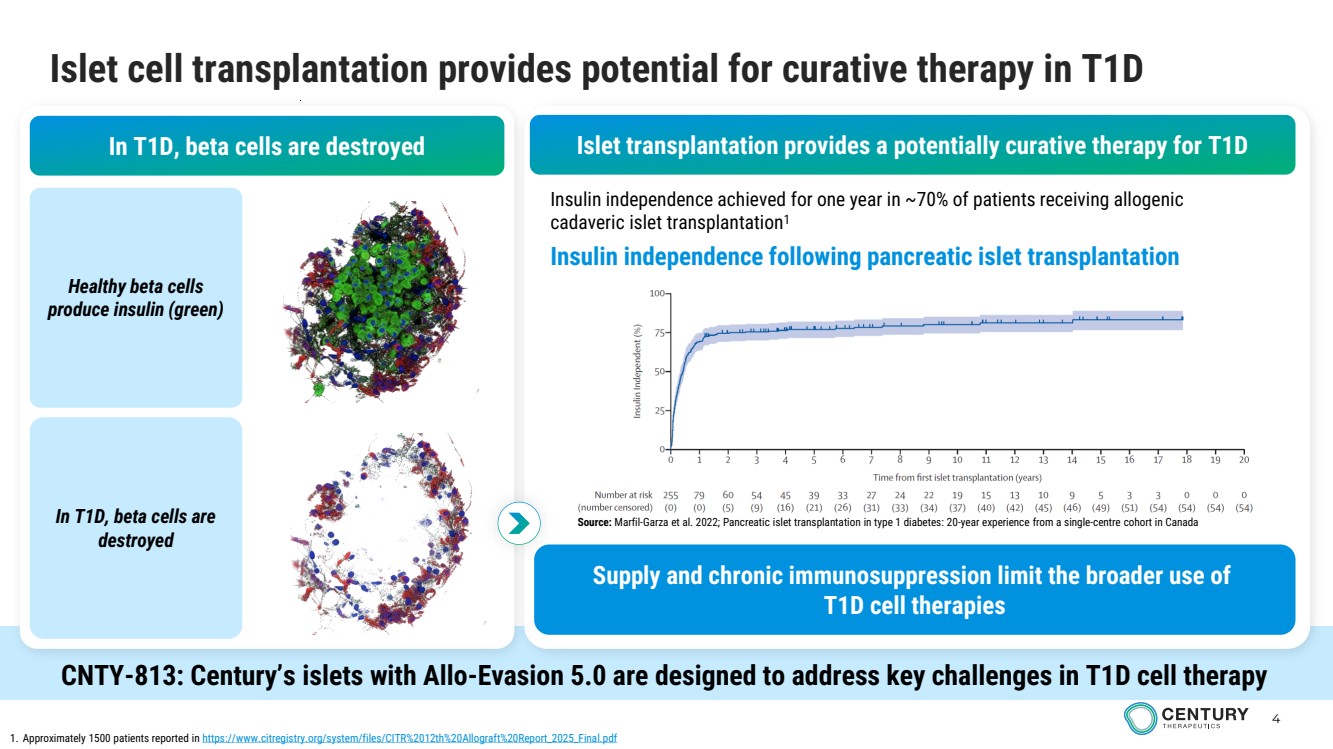
| 4 Islet cell transplantation provides potential for curative therapy in T1D In T1D, beta cells are destroyed Healthy beta cells produce insulin (green) In T1D, beta cells are destroyed Insulin independence following pancreatic islet transplantation 1. Approximately 1500 patients reported in https://www.citregistry.org/system/files/CITR%2012th%20Allograft%20Report_2025_Final.pdf Islet transplantation provides a potentially curative therapy for T1D Insulin independence achieved for one year in ~70% of patients receiving allogenic cadaveric islet transplantation1 Source: Marfil-Garza et al. 2022; Pancreatic islet transplantation in type 1 diabetes: 20-year experience from a single-centre cohort in Canada Supply and chronic immunosuppression limit the broader use of T1D cell therapies CNTY-813: Century’s islets with Allo-Evasion 5.0 are designed to address key challenges in T1D cell therapy |
| 5 Scalable manufacturing, islet function, and immune-evasive engineering address key barriers for T1D cell replacement DIFFERENTIATION PLATFORM • Scalable iPSC-derived islet manufacturing • Reproducible islet differentiation • Clinical manufacturing process from GMP MCB CNTY-813 design integrates key capabilities for off-the-shelf T1D cell therapy FUNCTIONAL ISLETS • Glucose-responsive insulin secretion • In vivo glucose control in diabetic mice • No safety events observed to date in preclinical models – i.e., cyst or tumor formation ALLO-EVASION 5.0 • T cell protection • NK cell protection • Reduced humoral immune clearance |
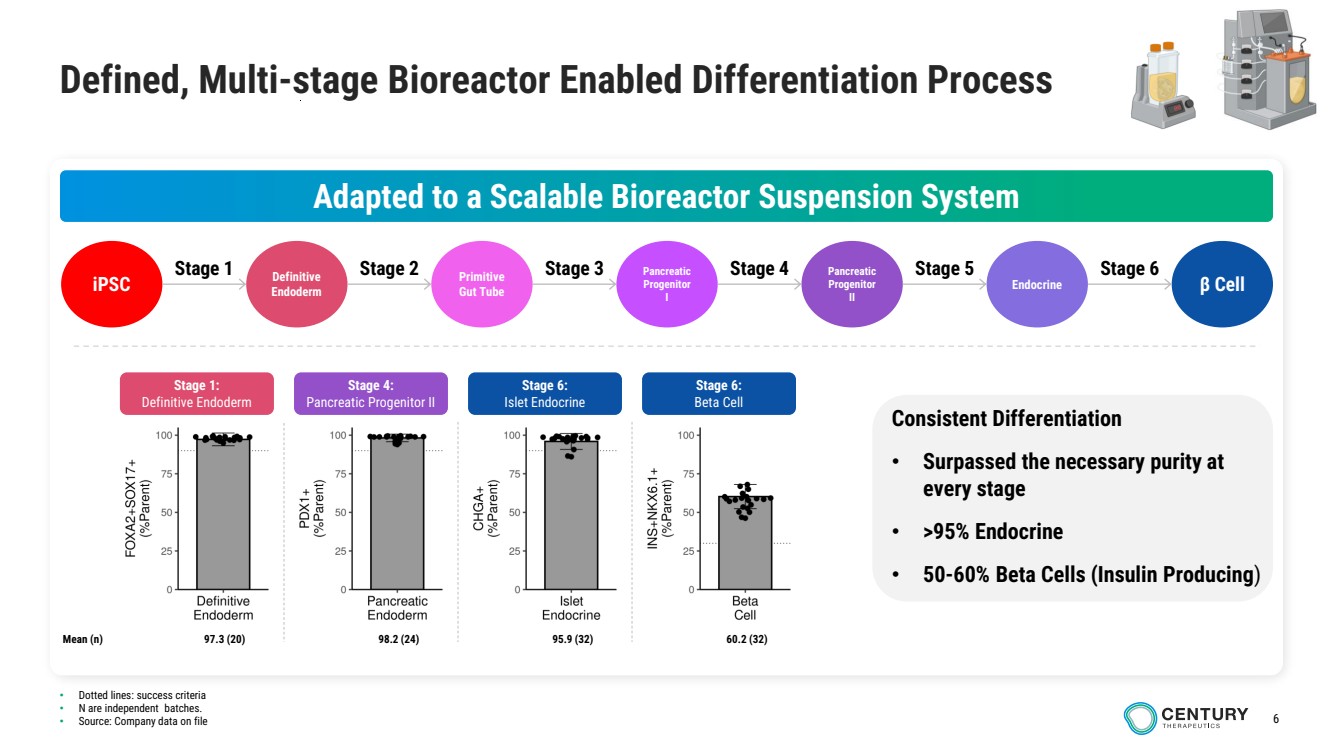
| 6 • Dotted lines: success criteria • N are independent batches. • Source: Company data on file Defined, Multi-stage Bioreactor Enabled Differentiation Process Adapted to a Scalable Bioreactor Suspension System iPSC Definitive Endoderm Primitive Gut Tube Pancreatic Progenitor I Pancreatic Progenitor II Endocrine β Cell Stage 1 Stage 2 Stage 3 Stage 4 Stage 5 Stage 6 Consistent Differentiation • Surpassed the necessary purity at every stage • >95% Endocrine • 50-60% Beta Cells (Insulin Producing) Stage 1: Definitive Endoderm Stage 4: Pancreatic Progenitor II Stage 6: Islet Endocrine Stage 6: Beta Cell Mean (n) 97.3 (20) 98.2 (24) 95.9 (32) 60.2 (32) |
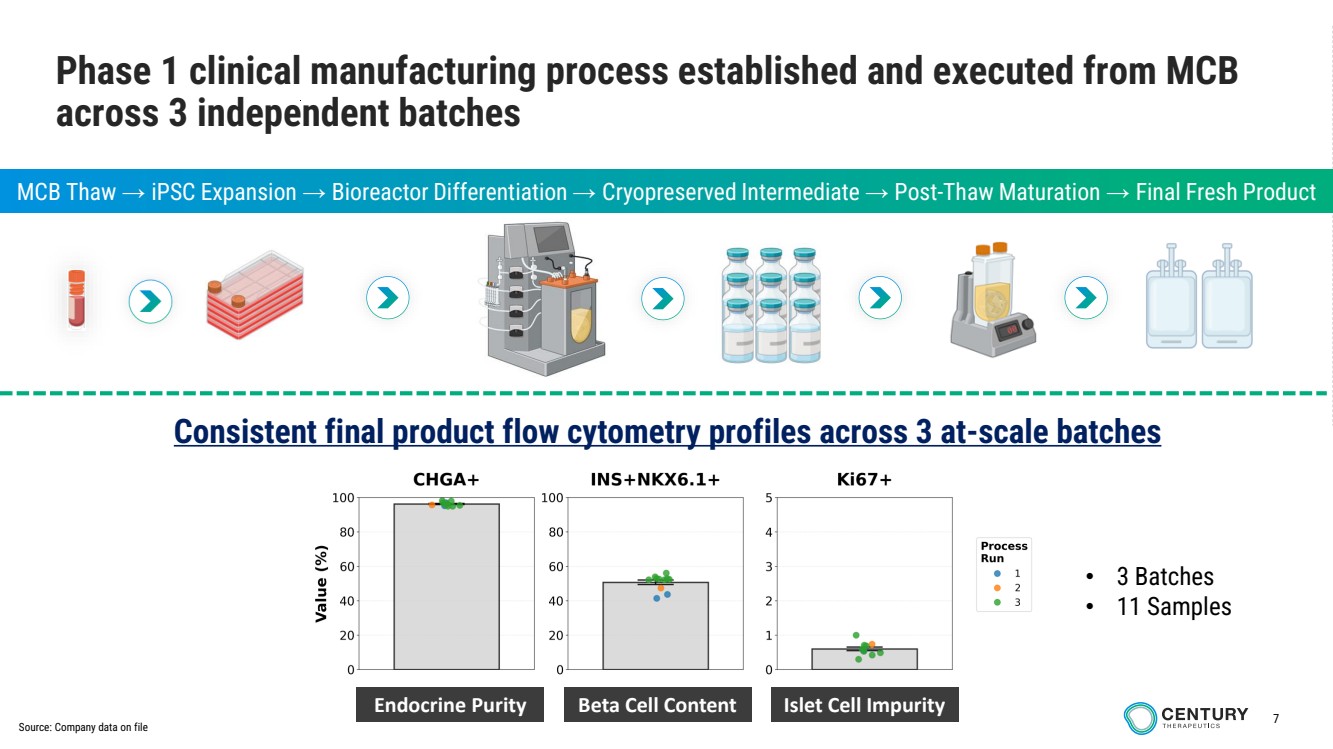
| 7 4X 300um CONFIDENTIAL Endocrine Purity Beta Cell Content Islet Cell Impurity • 3 Batches • 11 Samples Phase 1 clinical manufacturing process established and executed from MCB across 3 independent batches MCB Thaw → iPSC Expansion → Bioreactor Differentiation → Cryopreserved Intermediate → Post-Thaw Maturation → Final Fresh Product Consistent final product flow cytometry profiles across 3 at-scale batches Source: Company data on file |
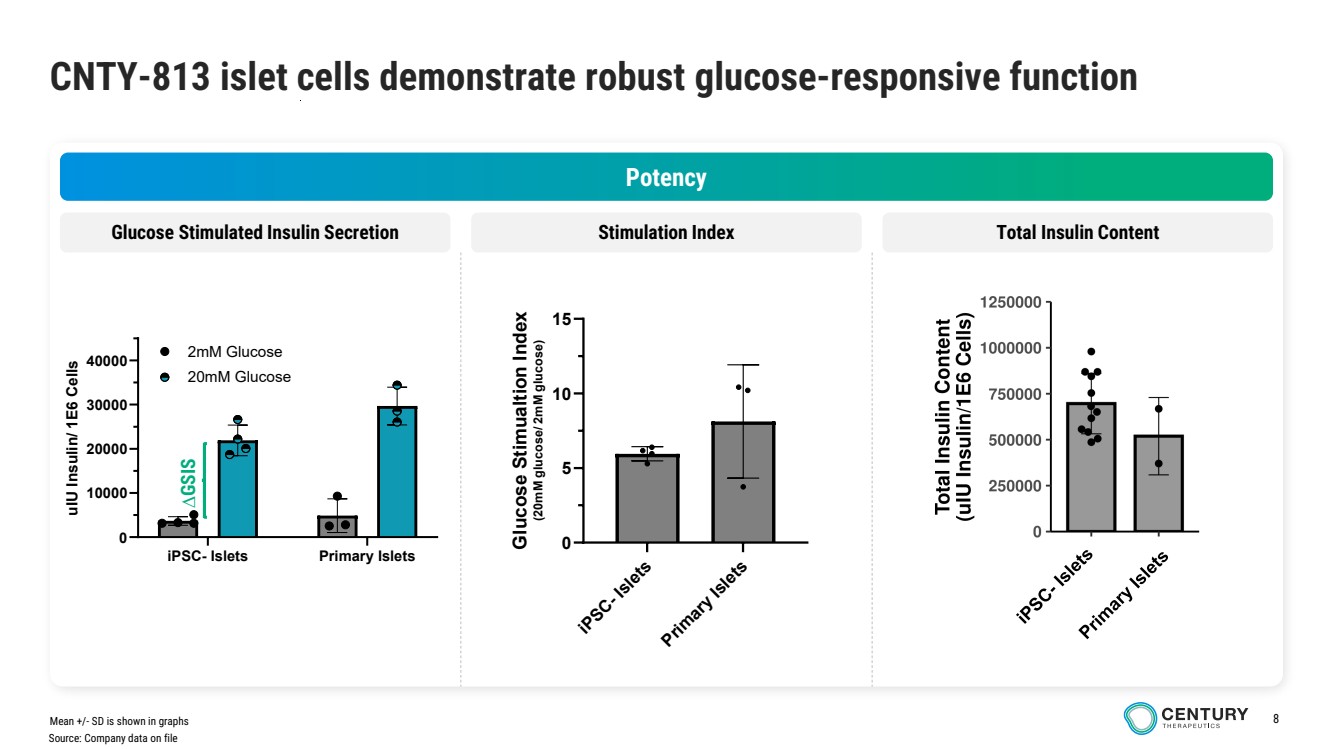
| 8 CNTY-813 islet cells demonstrate robust glucose-responsive function Potency Glucose Stimulated Insulin Secretion Stimulation Index Total Insulin Content iPSC- Islets Primary Islets 0 5 10 15 Glucose Stimualtion Index (20mM glucose/ 2mM glucose) Mean +/- SD is shown in graphs iPSC- Islets Primary Islets 0 10000 20000 30000 40000 u UI Insulin/ 1E6 Cells 2mM Glucose 20mM Glucose Source: Company data on file ∆GSIS |
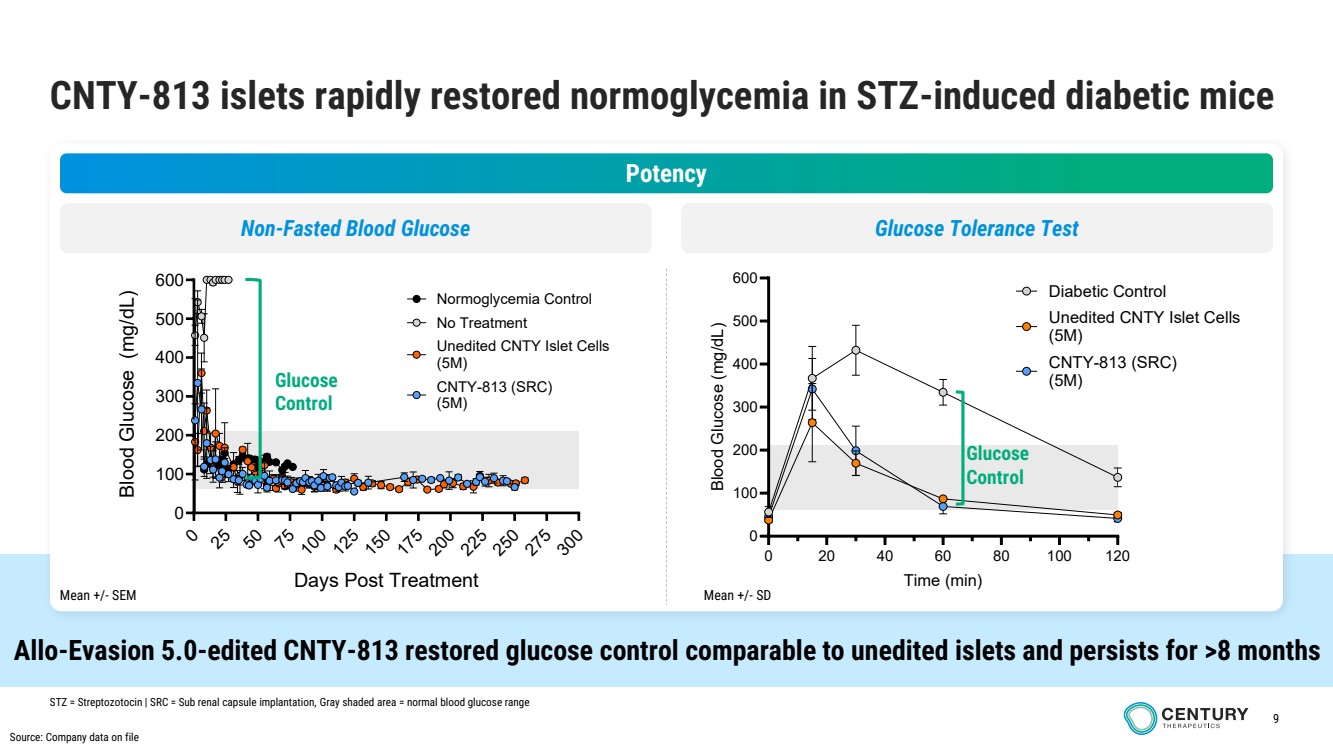
| 9 CNTY-813 islets rapidly restored normoglycemia in STZ-induced diabetic mice Allo-Evasion 5.0-edited CNTY-813 restored glucose control comparable to unedited islets and persists for >8 months Potency Non-Fasted Blood Glucose STZ = Streptozotocin | SRC = Sub renal capsule implantation, Gray shaded area = normal blood glucose range 0 25 50 75 10 125 150 175 20 2 5 250 275 30 0 100 200 300 400 500 600 Days Post Treatment Blood Glucose m( g/dL) No Treatment Normoglycemia Control CNTY-813 (SRC) (5M) Unedited CNTY Islet Cells (5M) 0 20 40 60 80 100 120 0 100 200 300 400 500 600 Time (min) Blood Glucose (mg/dL) Diabetic Control Unedited CNTY Islet Cells (5M) CNTY-813 (SRC) (5M) Glucose Control Glucose Control Glucose Tolerance Test Source: Company data on file Mean +/- SEM Mean +/- SD |
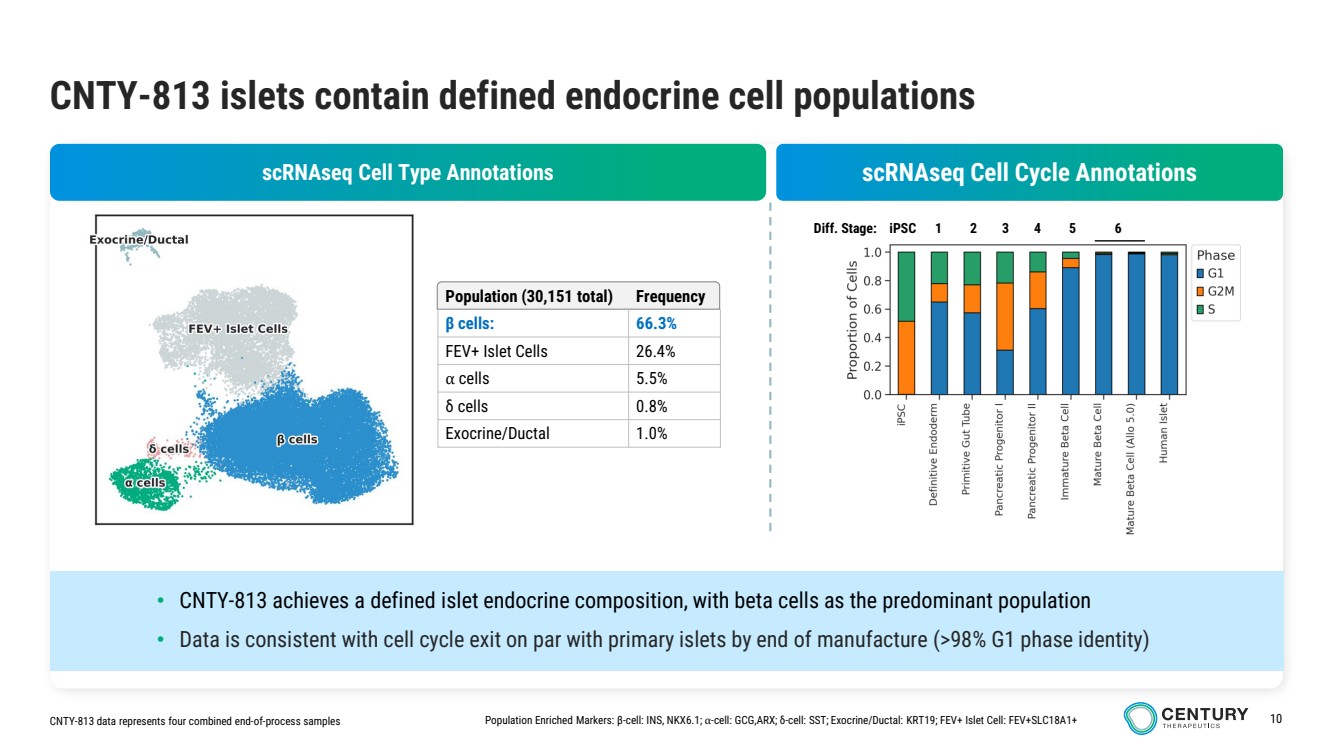
| 10 CNTY-813 islets contain defined endocrine cell populations Population (30,151 total) Frequency β cells: 66.3% FEV+ Islet Cells 26.4% ⍺ cells 5.5% δ cells 0.8% Exocrine/Ductal 1.0% CNTY-813 data represents four combined end-of-process samples Population Enriched Markers: β-cell: INS, NKX6.1; ⍺-cell: GCG,ARX; δ-cell: SST; Exocrine/Ductal: KRT19; FEV+ Islet Cell: FEV+SLC18A1+ scRNAseq Cell Cycle Annotations Diff. Stage: iPSC 1 2 3 4 5 6 scRNAseq Cell Type Annotations • CNTY-813 achieves a defined islet endocrine composition, with beta cells as the predominant population • Data is consistent with cell cycle exit on par with primary islets by end of manufacture (>98% G1 phase identity) |
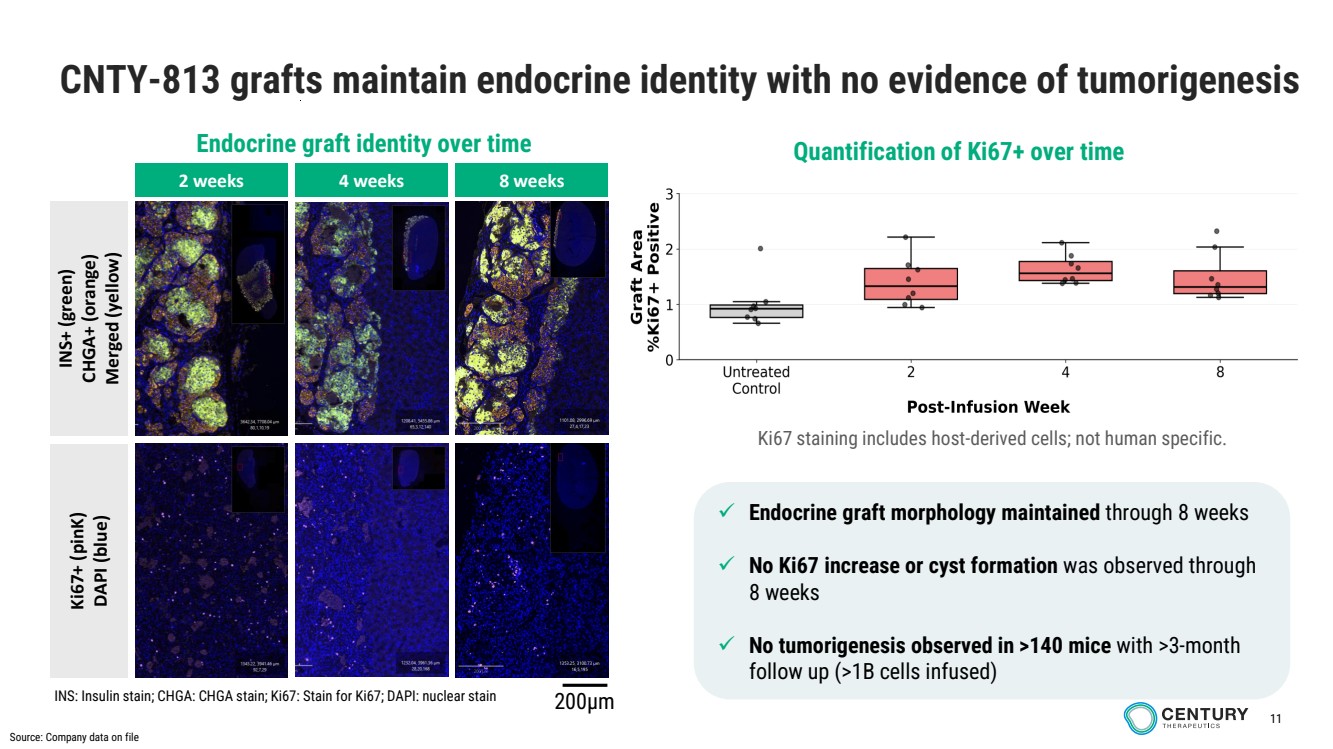
| 11 CNTY-813 grafts maintain endocrine identity with no evidence of tumorigenesis 2 weeks INS+ (green) CHGA+ (orange) Merged (yellow) 4 weeks 8 weeks Ki67+ (pinK) DAPI (blue) Endocrine graft identity over time ✓ Endocrine graft morphology maintained through 8 weeks ✓ No Ki67 increase or cyst formation was observed through 8 weeks ✓ No tumorigenesis observed in >140 mice with >3-month follow up (>1B cells infused) Quantification of Ki67+ over time Ki67 staining includes host-derived cells; not human specific. INS: Insulin stain; CHGA: CHGA stain; Ki67: Stain for Ki67; DAPI: nuclear stain 200µm Source: Company data on file |
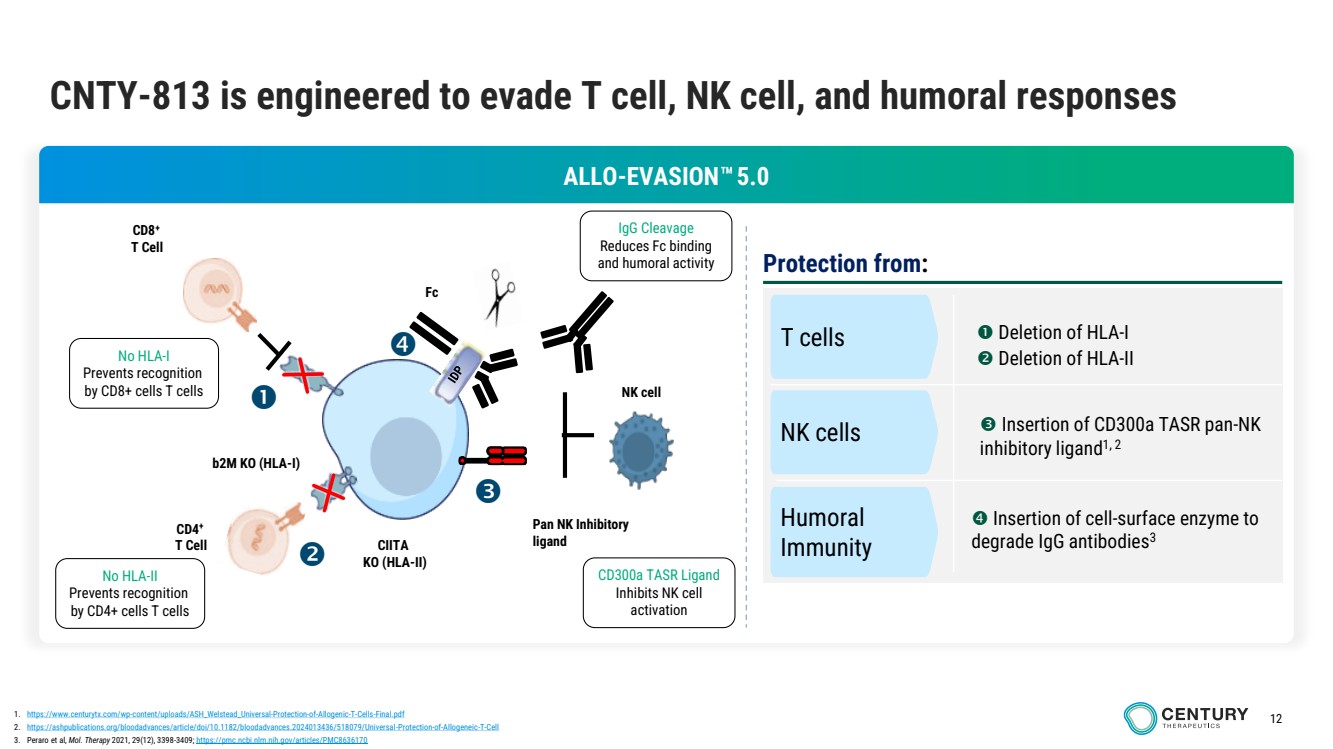
| 12 CNTY-813 is engineered to evade T cell, NK cell, and humoral responses Protection from: T cells NK cells Humoral Immunity Deletion of HLA-I Deletion of HLA-II Insertion of CD300a TASR pan-NK inhibitory ligand1, 2 Insertion of cell-surface enzyme to degrade IgG antibodies3 1. https://www.centurytx.com/wp-content/uploads/ASH_Welstead_Universal-Protection-of-Allogenic-T-Cells-Final.pdf 2. https://ashpublications.org/bloodadvances/article/doi/10.1182/bloodadvances.2024013436/518079/Universal-Protection-of-Allogeneic-T-Cell 3. Peraro et al, Mol. Therapy 2021, 29(12), 3398-3409; https://pmc.ncbi.nlm.nih.gov/articles/PMC8636170 b2M KO (HLA-I) CIITA KO (HLA-II) CD8+ T Cell CD4+ T Cell Pan NK Inhibitory ligand Fc NK cell No HLA-I Prevents recognition by CD8+ cells T cells No HLA-II Prevents recognition by CD4+ cells T cells IgG Cleavage Reduces Fc binding and humoral activity CD300a TASR Ligand Inhibits NK cell activation ALLO-EVASION 5.0 |
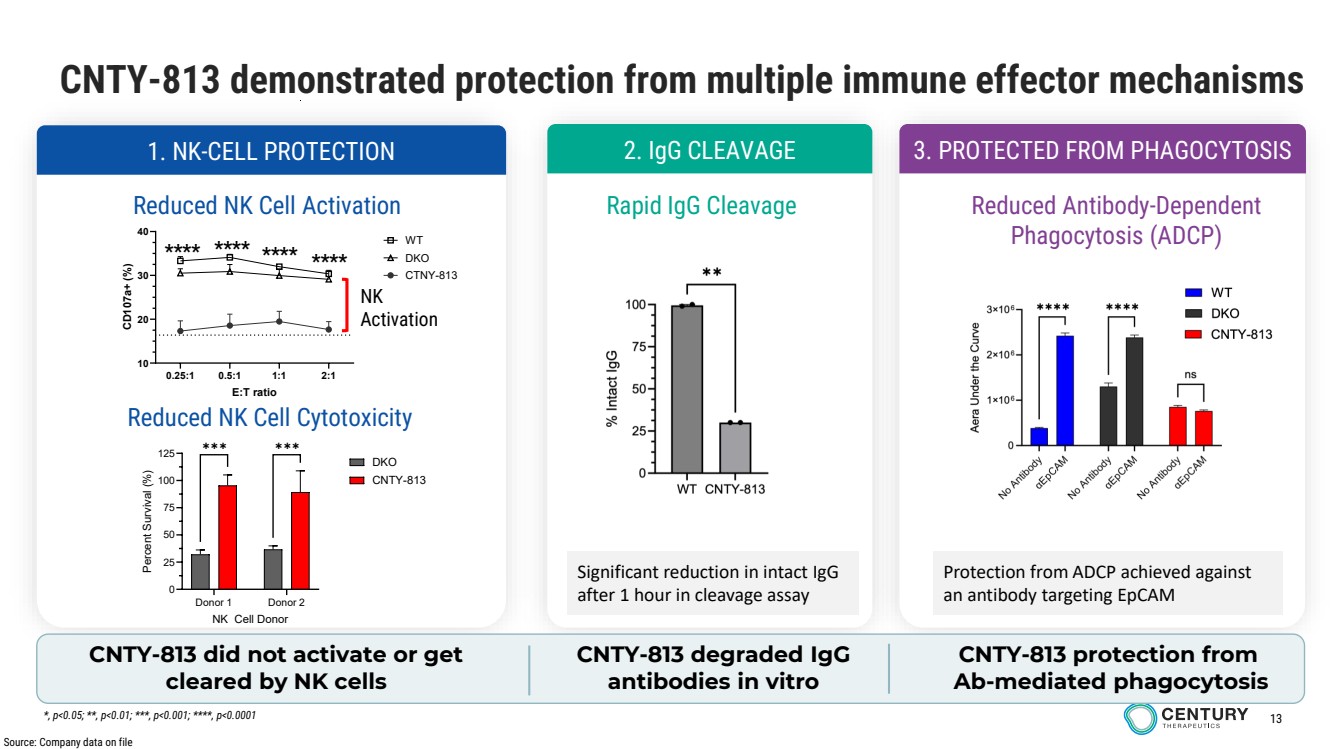
| 13 CNTY-813 demonstrated protection from multiple immune effector mechanisms 1. NK-CELL PROTECTION 2. IgG CLEAVAGE 3. PROTECTED FROM PHAGOCYTOSIS Reduced NK Cell Activation Reduced NK Cell Cytotoxicity Rapid IgG Cleavage Reduced Antibody-Dependent Phagocytosis (ADCP) Significant reduction in intact IgG after 1 hour in cleavage assay CNTY-813 did not activate or get cleared by NK cells CNTY-813 degraded IgG antibodies in vitro CNTY-813 protection from Ab-mediated phagocytosis Protection from ADCP achieved against an antibody targeting EpCAM 0.25:1 0.5:1 1:1 2:1 10 20 30 40 E:T ratio CD107a+ (%) WT DKO CTNY-813 **** **** **** **** NK Activation Source: Company data on file *, p<0.05; **, p<0.01; ***, p<0.001; ****, p<0.0001 Donor 1 Donor 2 0 25 50 75 100 125 NK Cell Donor Percent Survival (%) DKO CNTY-813 ✱✱✱ ✱✱✱ |
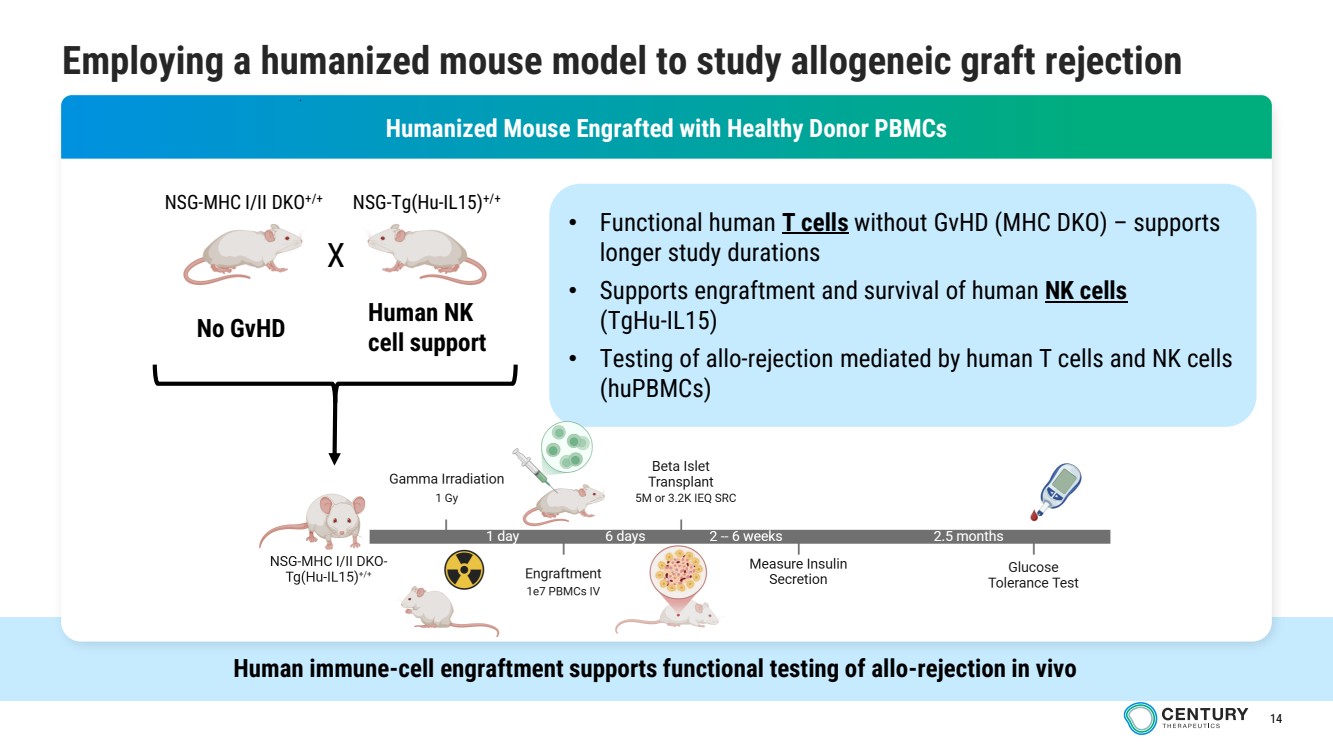
| 14 Employing a humanized mouse model to study allogeneic graft rejection d Humanized Mouse Engrafted with Healthy Donor PBMCs • Functional human T cells without GvHD (MHC DKO) – supports longer study durations • Supports engraftment and survival of human NK cells (TgHu-IL15) • Testing of allo-rejection mediated by human T cells and NK cells (huPBMCs) NSG-MHC I/II DKO+/+ NSG-Tg(Hu-IL15)+/+ X No GvHD Human NK cell support Human immune-cell engraftment supports functional testing of allo-rejection in vivo |
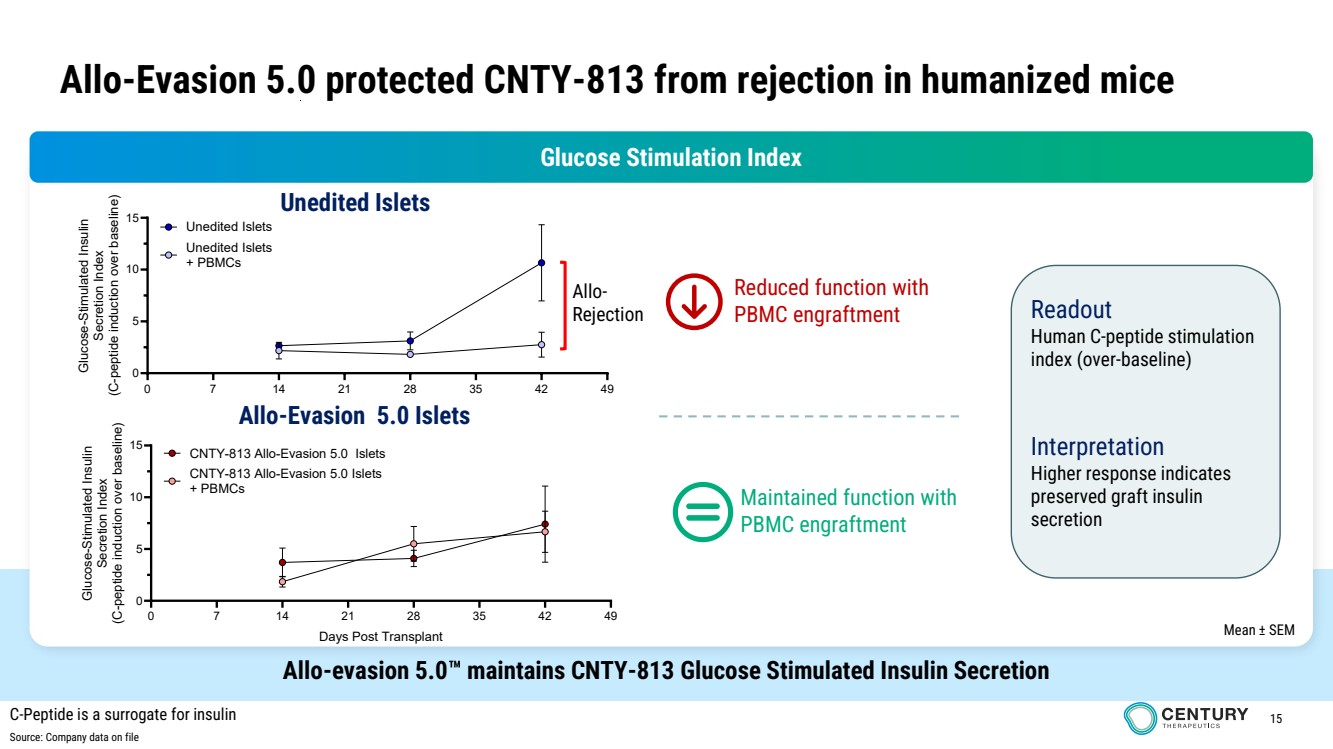
| 15 Allo-evasion 5.0 maintains CNTY-813 Glucose Stimulated Insulin Secretion Allo-Evasion 5.0 protected CNTY-813 from rejection in humanized mice 0 7 14 21 28 35 42 49 0 5 10 15 Days Post Transplant Glucose-Stimulated Insulin Secretion Index (C-peptide induction over baseline) Unedited Islets + PBMCs Unedited Islets 0 7 14 21 28 35 42 49 0 5 10 15 Days Post Transplant Glucose-Stimulated Insulin Secretion Index (C-peptide induction over baseline) CNTY-813 Allo-Evasion 5.0 Islets + PBMCs CNTY-813 Allo-Evasion 5.0 Islets Glucose Stimulation Index Mean ± SEM Allo-Rejection Reduced function with PBMC engraftment Maintained function with PBMC engraftment Unedited Islets Allo-Evasion 5.0 Islets Readout Human C-peptide stimulation index (over-baseline) Interpretation Higher response indicates preserved graft insulin secretion C-Peptide is a surrogate for insulin Source: Company data on file |
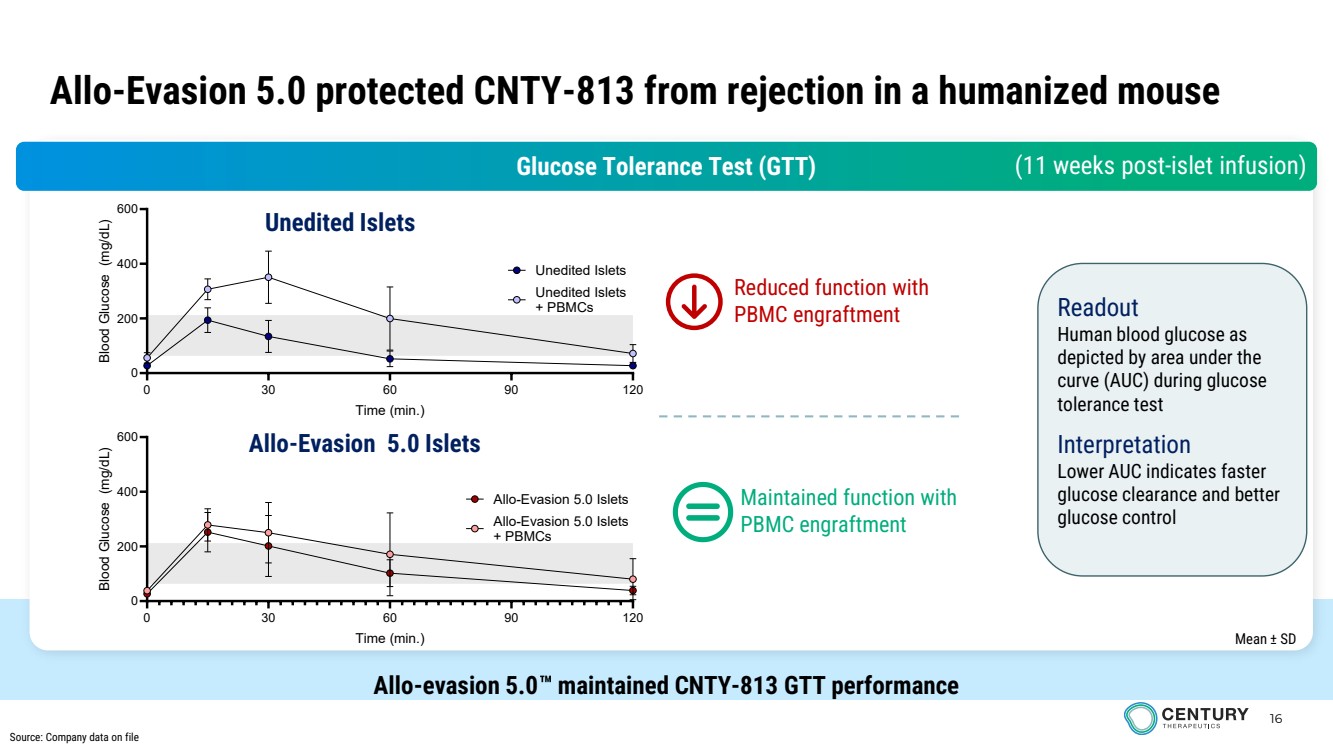
| 16 Allo-evasion 5.0 maintained CNTY-813 GTT performance 0 30 60 90 120 0 200 400 600 Time (min.) Blood Glucose (mg/dL) Unedited Islets + PBMCs Unedited Islets 0 30 60 90 120 0 200 400 600 Time (min.) Blood Glucose (mg/dL) Allo-Evasion 5.0 Islets + PBMCs Allo-Evasion 5.0 Islets Glucose Tolerance Test (GTT) Unedited Islets Allo-Evasion 5.0 Islets (11 weeks post-islet infusion) Mean ± SD Readout Human blood glucose as depicted by area under the curve (AUC) during glucose tolerance test Interpretation Lower AUC indicates faster glucose clearance and better glucose control Allo-Evasion 5.0 protected CNTY-813 from rejection in a humanized mouse Reduced function with PBMC engraftment Maintained function with PBMC engraftment Source: Company data on file |
| 17 These data support the development of CNTY-813 as a potentially broadly accessible off-the-shelf cell therapy for Type 1 Diabetes DIFFERENTIATION PLATFORM • Reproducible, bioreactor-enabled differentiation from GMP MCB • Phase 1 clinical manufacturing process established • CNTY-813 specs: – >95% islet endocrine – >50% beta cell identity CNTY-813 demonstrated reproducible differentiation, durable glucose control, and immune-evasive function in preclinical models FUNCTIONAL ISLETS • GSIS potency similar to primary islets • Rapid and durable glucose control observed in diabetic mice • Maintained graft identity with a favorable safety profile ALLO-EVASION 5.0 • Engineered to reduce T-cell, NK-cell, and humoral immune recognition • Protection from NK and humoral clearance demonstrated • Preserved graft function under alloimmune pressure in vivo |