Exhibit 99.1
https://cogrx.com COGNITION THERAPEUTICS · NASDAQ: CGTX An Investigational Oral Therapy Advancing Toward Registrational Development June 2026 · Jefferies Global Healthcare Conference Zervimesine in DLB Psychosis
2 COGNITION THERAPEUTICS | NASDAQ: CGTX FORWARD - LOOKING STATEMENTS This presentation contains forward - looking statements within the meaning of The Private Securities Litigation Reform Act of 1995 . All statements contained in this presentation, other than statements of historical facts or statements that relate to present facts or current conditions, including but not limited to, product candidates, including ze rvi mesine, also known as zervimesine, and any expected or implied benefits or results, including that initial clinical results observed with respect to zervimesine will be replicated in later trials, and our clinical developmen t p lans, including statements regarding our clinical studies of zervimesine and our regulatory plans, expectations regarding potential patient populations, expectations regarding our patent portfolio, and our expected cash runw ay, are forward - looking statements. These statements, including statements related to the timing and expected results of our clinical trials, involve known and unknown risks, uncertainties and other important factors that may cau se our actual results, performance, or achievements to be materially different from any future results, performance, or achievements expressed or implied by the forward - looking statements. In some cases, you can identify fo rward - looking statements by terms such as “may,” “might,” “will,” “should,” “expect,” “plan,” “aim,” “seek,” “anticipate,” “could,” “intend,” “target,” “project,” “contemplate,” “believe,” “estimate,” “predict,” “foreca st, ” “potential” or “continue” or the negative of these terms or other similar expressions. We have based these forward - looking statements largely on our current expectations and projections about future events and financial tre nds that we believe may affect our business, financial condition, and results of operations. These forward - looking statements speak only as of the date of this presentation and are subject to a number of risks, uncertainties and assumptions, some of which cannot be predicted or quantified and some of which are beyond our control. Factors that may cause actual results to differ materially from current expectations include, but are not limited to : o ur ability to successfully advance our current and future product candidates through development activities, preclinical studies and clinical trials and costs related thereto; uncertainties inherent in the results of preli min ary data, preclinical studies and earlier - stage clinical trials being predictive of the results of early or later - stage clinical trials; the timing, scope and likelihood of regulatory filings and approvals, including regulatory approval of ou r product candidates; competition, our ability to secure new (and retain existing) grant funding, our ability to grow and manage growth, maintain relationships with suppliers and retain our management and key employees; changes in appl ica ble laws or regulations; the possibility that the we may be adversely affected by other economic, business or competitive factors, including ongoing economic uncertainty; our estimates of expenses and profitabilit y; the evolution of the markets in which we compete; our ability to implement our strategic initiatives and continue to innovate our existing products; our ability to defend our intellectual property; impacts of global political cha nges and global economic conditions on our business, supply chain and labor force; our ability to maintain the listing of our common stock on the Nasdaq Global Market; and the risks and uncertainties described more fully in th e “Risk Factors” section of our annual and quarterly reports filed with the Securities & Exchange Commission that are available on www.sec.gov. These risks are not exhaustive, and we face both known and unknown risks. You shou ld not rely on these forward - looking statements as predictions of future events. The events and circumstances reflected in our forward - looking statements may not be achieved or occur, and actual results could differ mate rially from those projected in the forward - looking statements. Moreover, we operate in a dynamic industry and economy. New risk factors and uncertainties may emerge from time to time, and it is not possible for management to predict all risk factors and uncertainties that we may face. Except as required by applicable law, we do not plan to publicly update or revise any forward - looking statements contained herein, whether as a result of any new information, future events, changed circumstances or otherwise. TRADEMARKS This presentation may contain trademarks, service marks, trade names and copyrights of other companies, which are the propert y o f their respective owners. Solely for convenience, some of the trademarks, service marks, trade names and copyrights referred to in this presentation may be listed without the TM, SM © or ® symbols, but we will asse rt, to the fullest extent under applicable law, the rights of the applicable owners, if any, to these trademarks, service marks, trade names and copyrights. MARKET & INDUSTRY DATA Projections, estimates, industry data and information contained in this presentation, including the size of and growth in key en d markets, are based on information from third - party sources and management estimates. Although we believe that these third party - sources are reliable, we cannot guarantee the accuracy or completeness of these sources. Our m anagement’s estimates are derived from third - party sources, publicly available information, our knowledge of our industry and assumptions based on such information and knowledge. Our management’s estimates have not been v eri fied by any independent source. All of the projections, estimates, market data and industry information used in this presentation involve a number of assumptions and limitations, and you are cautioned not to give undue weight to such information. In addition, projections, es ti mates and assumptions relating to us and our industry's future performance are necessarily subject to a high degree of uncertainty and risk due to a variety of fa ctors, including, but not limited to, those described above, that could cause future performance to differ materially from our expressed projections, estimates and assumptions or those provided by third parties.
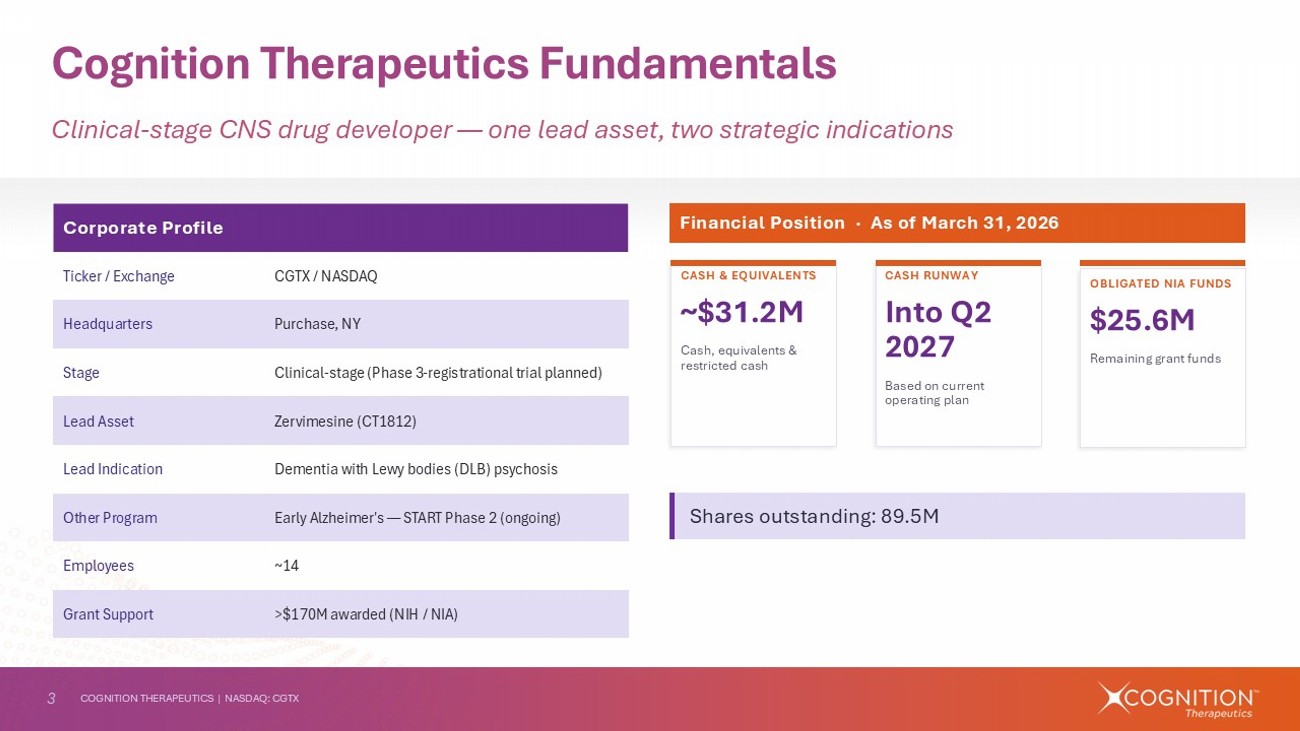
3 COGNITION THERAPEUTICS | NASDAQ: CGTX Cognition Therapeutics Fundamentals Clinical - stage CNS drug developer — one lead asset, two strategic indications Corporate Profile CGTX / NASDAQ Ticker / Exchange Purchase, NY Headquarters Clinical - stage (Phase 3 - registrational trial planned) Stage Zervimesine (CT1812) Lead Asset Dementia with Lewy bodies (DLB) psychosis Lead Indication Early Alzheimer's — START Phase 2 (ongoing) Other Program ~14 Employees >$170M awarded (NIH / NIA) Grant Support Financial Position · As of March 31, 2026 CASH & EQUIVALENTS ~$31.2M Cash, equivalents & restricted cash OBLIGATED NIA FUNDS $25.6M Remaining grant funds CASH RUNWAY Into Q2 2027 Based on current operating plan Shares outstanding: 89.5M AS1
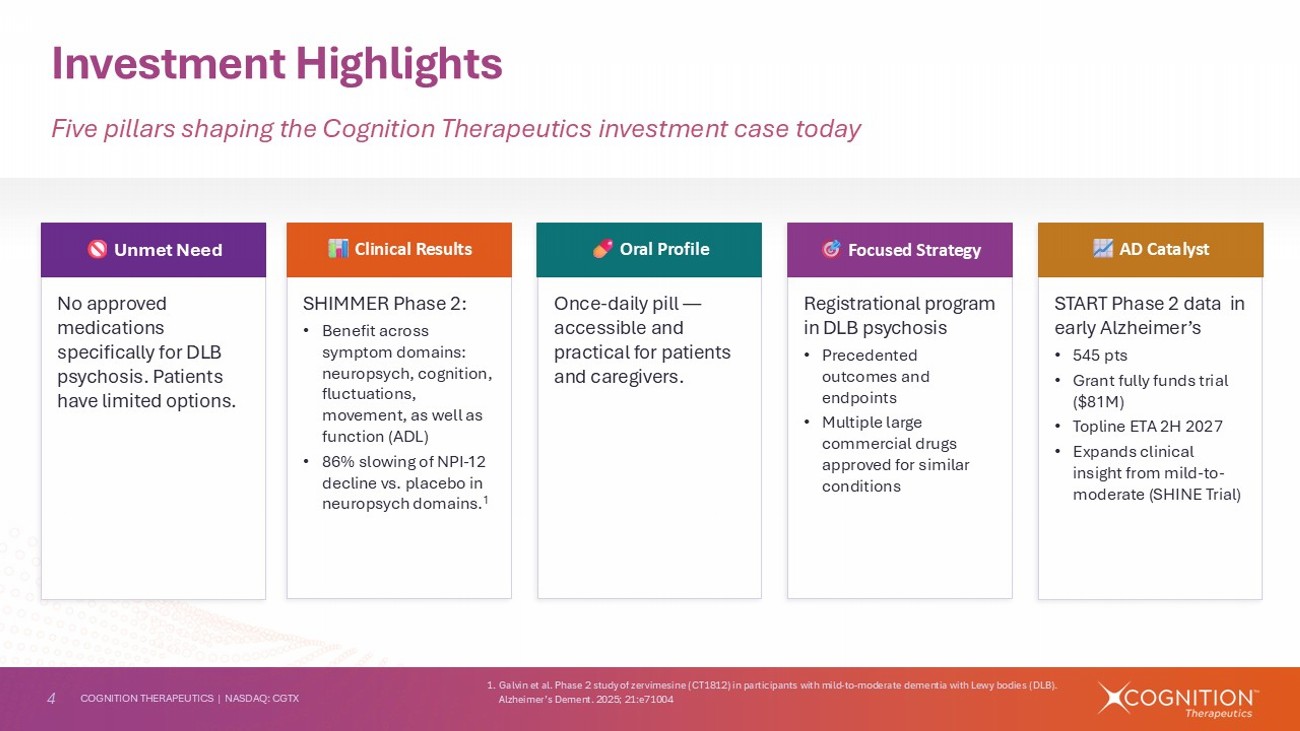
4 COGNITION THERAPEUTICS | NASDAQ: CGTX Investment Highlights Five pillars shaping the Cognition Therapeutics investment case today No approved medications specifically for DLB psychosis. Patients have limited options. Unmet Need SHIMMER Phase 2: • Benefit across symptom domains: neuropsych , cognition, fluctuations, movement, as well as function (ADL) • 86% slowing of NPI - 12 decline vs. placebo in neuropsych domains. 1 Clinical Results Once - daily pill — accessible and practical for patients and caregivers. Oral Profile Registrational program in DLB psychosis • Precedented outcomes and endpoints • Multiple large commercial drugs approved for similar conditions Focused Strategy START Phase 2 data in early Alzheimer’s • 545 pts • Grant fully funds trial ($81M) • Topline ETA 2H 2027 • Expands clinical insight from mild - to - moderate (SHINE Trial) AD Catalyst 1. Galvin et al. Phase 2 study of zervimesine (CT1812) in participants with mild - to - moderate dementia with Lewy bodies (DLB). Alzheimer’s Dement. 2025; 21:e71004
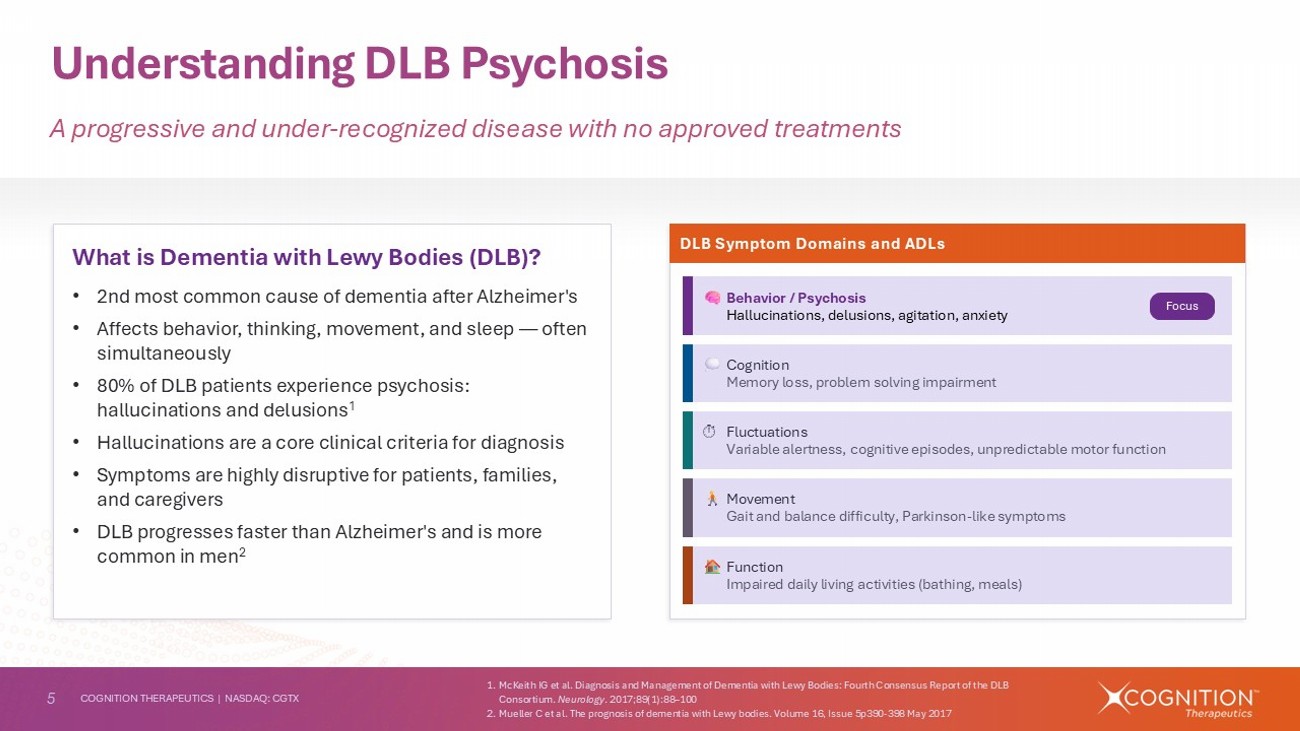
5 COGNITION THERAPEUTICS | NASDAQ: CGTX Understanding DLB Psychosis A progressive and under - recognized disease with no approved treatments What is Dementia with Lewy Bodies (DLB)? • 2nd most common cause of dementia after Alzheimer's • Affects behavior, thinking, movement, and sleep — often simultaneously • 80% of DLB patients experience psychosis: hallucinations and delusions 1 • Hallucinations are a core clinical criteria for diagnosis • Symptoms are highly disruptive for patients, families, and caregivers • DLB progresses faster than Alzheimer's and is more common in men 2 DLB Symptom Domains and ADLs Behavior / Psychosis Hallucinations, delusions, agitation, anxiety Function Impaired daily living activities (bathing, meals) Cognition Memory loss, problem solving impairment Movement Gait and balance difficulty, Parkinson - like symptoms Fluctuations Variable alertness, cognitive episodes, unpredictable motor function Focus 1. McKeith IG et al. Diagnosis and Management of Dementia with Lewy Bodies: Fourth Consensus Report of the DLB Consortium. Neurology . 2017;89(1):88 – 100 2. Mueller C et al. The prognosis of dementia with Lewy bodies. Volume 16, Issue 5p390 - 398 May 2017
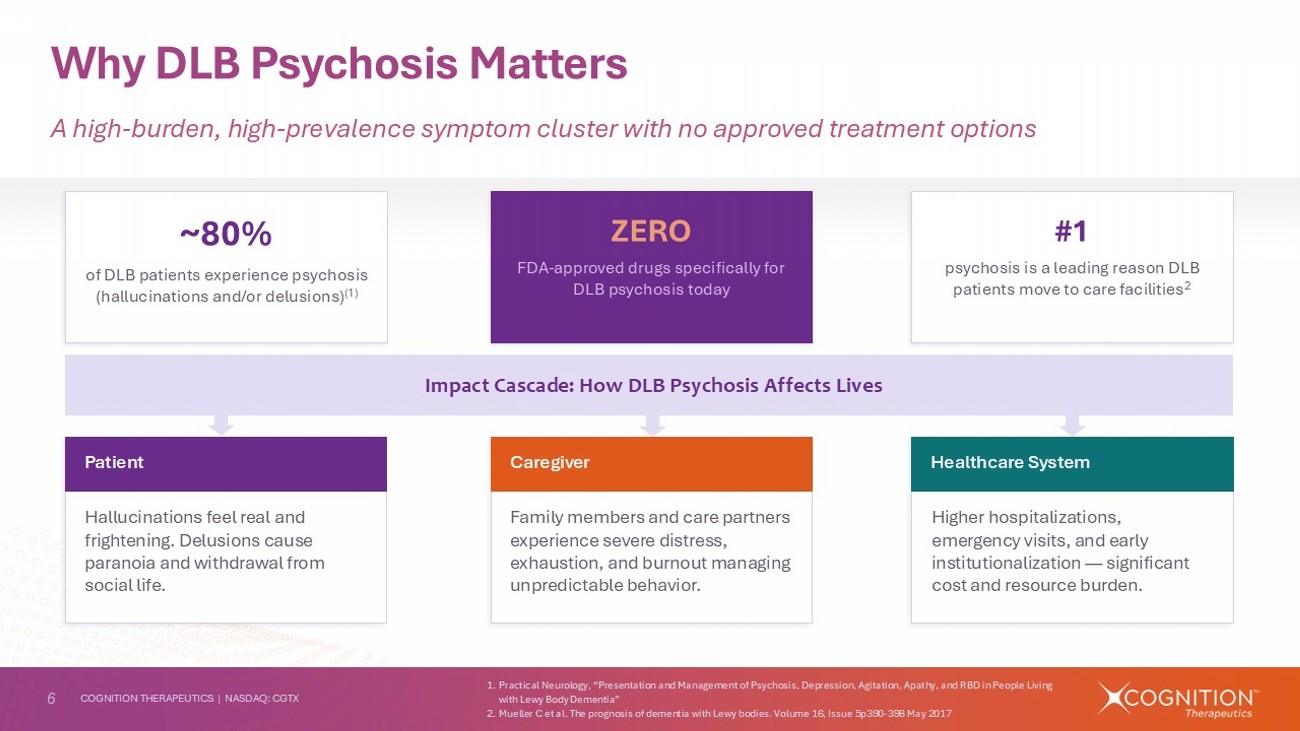
6 COGNITION THERAPEUTICS | NASDAQ: CGTX Why DLB Psychosis Matters A high - burden, high - prevalence symptom cluster with no approved treatment options ~80% of DLB patients experience psychosis (hallucinations and/or delusions) (1) ZERO FDA - approved drugs specifically for DLB psychosis today #1 psychosis is a leading reason DLB patients move to care facilities 2 Impact Cascade: How DLB Psychosis Affects Lives Hallucinations feel real and frightening. Delusions cause paranoia and withdrawal from social life. Patient Family members and care partners experience severe distress, exhaustion, and burnout managing unpredictable behavior. Caregiver Higher hospitalizations, emergency visits, and early institutionalization — significant cost and resource burden. Healthcare System 1. Practical Neurology, “Presentation and Management of Psychosis, Depression, Agitation, Apathy, and RBD in People Living with Lewy Body Dementia” 2. Mueller C et al. The prognosis of dementia with Lewy bodies. Volume 16, Issue 5p390 - 398 May 2017
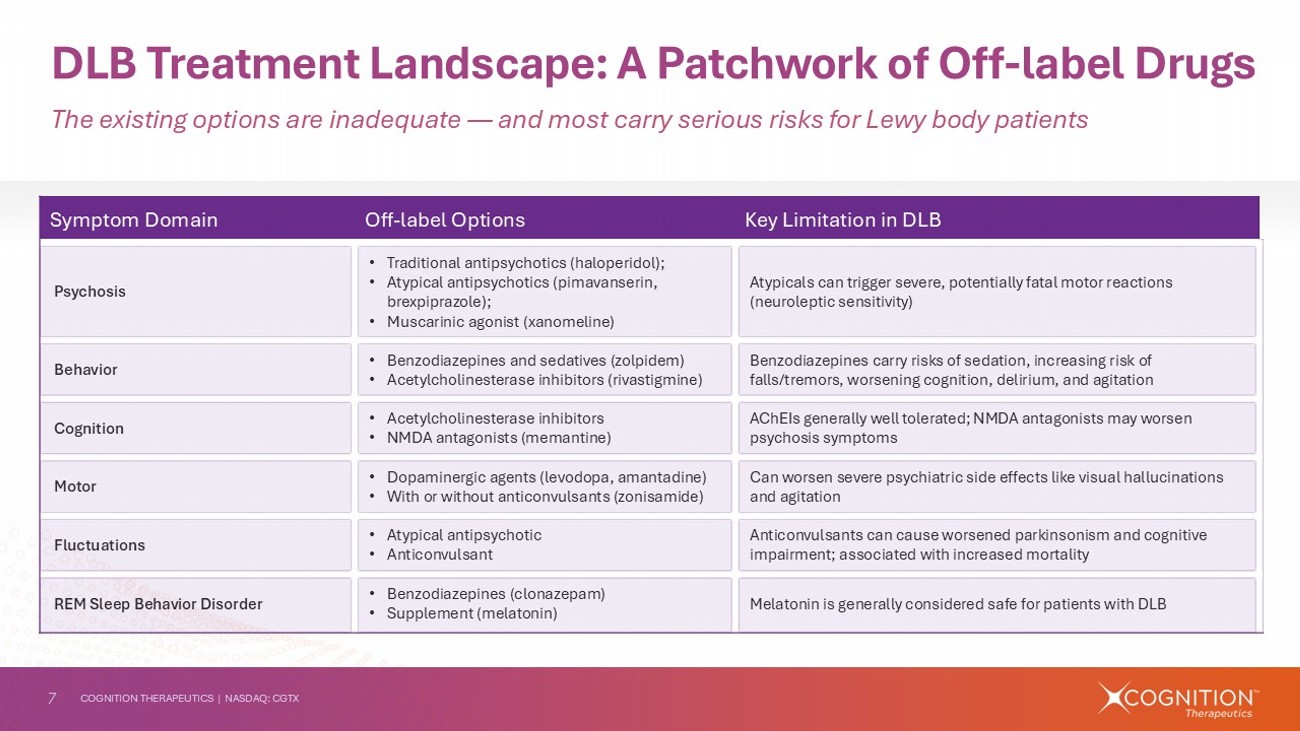
7 COGNITION THERAPEUTICS | NASDAQ: CGTX Key Limitation in DLB Off - label Options Symptom Domain Atypicals can trigger severe, potentially fatal motor reactions (neuroleptic sensitivity) • Traditional antipsychotics (haloperidol); • Atypical antipsychotics (pimavanserin, brexpiprazole ); • Muscarinic agonist ( xanomeline ) Psychosis Benzodiazepines carry risks of sedation, increasing risk of falls/tremors, worsening cognition, delirium, and agitation • Benzodiazepines and sedatives (zolpidem) • Acetylcholinesterase inhibitors (rivastigmine) Behavior AChEIs generally well tolerated; NMDA antagonists may worsen psychosis symptoms • Acetylcholinesterase inhibitors • NMDA antagonists (memantine) Cognition Can worsen severe psychiatric side effects like visual hallucinations and agitation • Dopaminergic agents (levodopa, amantadine) • With or without anticonvulsants (zonisamide) Motor Anticonvulsants can cause worsened parkinsonism and cognitive impairment; associated with increased mortality • Atypical antipsychotic • Anticonvulsant Fluctuations Melatonin is generally considered safe for patients with DLB • Benzodiazepines (clonazepam) • Supplement (melatonin) REM Sleep Behavior Disorder The existing options are inadequate — and most carry serious risks for Lewy body patients DLB Treatment Landscape: A Patchwork of Off - label Drugs
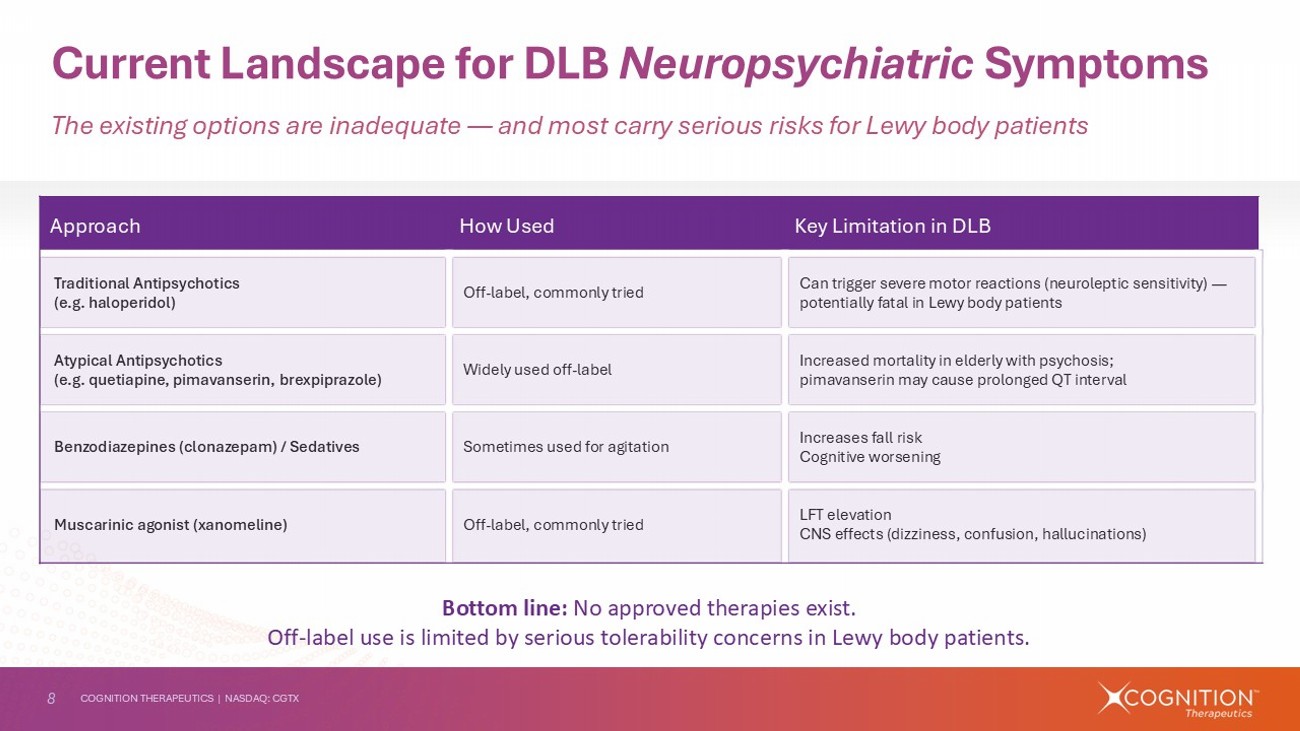
8 COGNITION THERAPEUTICS | NASDAQ: CGTX Key Limitation in DLB How Used Approach Can trigger severe motor reactions (neuroleptic sensitivity) — potentially fatal in Lewy body patients Off - label, commonly tried Traditional Antipsychotics (e.g. haloperidol) Increased mortality in elderly with psychosis; pimavanserin may cause prolonged QT interval Widely used off - label Atypical Antipsychotics (e.g. quetiapine, pimavanserin, brexpiprazole ) Increases fall risk Cognitive worsening Sometimes used for agitation Benzodiazepines (clonazepam) / Sedatives LFT elevation CNS effects (dizziness, confusion, hallucinations) Off - label, commonly tried Muscarinic agonist ( xanomeline ) The existing options are inadequate — and most carry serious risks for Lewy body patients Current Landscape for DLB Neuropsychiatric Symptoms Bottom line: No approved therapies exist. Off - label use is limited by serious tolerability concerns in Lewy body patients.
9 COGNITION THERAPEUTICS | NASDAQ: CGTX Zervimesine (CT1812) — Product Profile An oral small molecule with a practical profile for a population that needs it most • Generally well tolerated in >450 patients • No ARIA expectation from MoA • AE rates comparable to placebo in 100mg dose group Safety Profile • Strong results in hallucinations and delusions • Potential to improve cognition, fluctuations, behavior, and motor symptoms, as well as ADLs Symptom Focus • Oral, once - daily administration • 100 mg dose established based on Phase 2 study work Route & Dosing • DLB patients with psychosis • Ages 50 - 85 in Phase 2 studies • Use in community neurology setting Target Patient 1. Galvin et al. Phase 2 study of zervimesine (CT1812) in participants with mild - to - moderate dementia with Lewy bodies (DLB). Alzheimer’s Dement. 2025; 21:e71004 Abbreviations: ARIA=Amyloid - related imaging abnormalities; MoA =mechanism of action; ADLs=activities of daily living
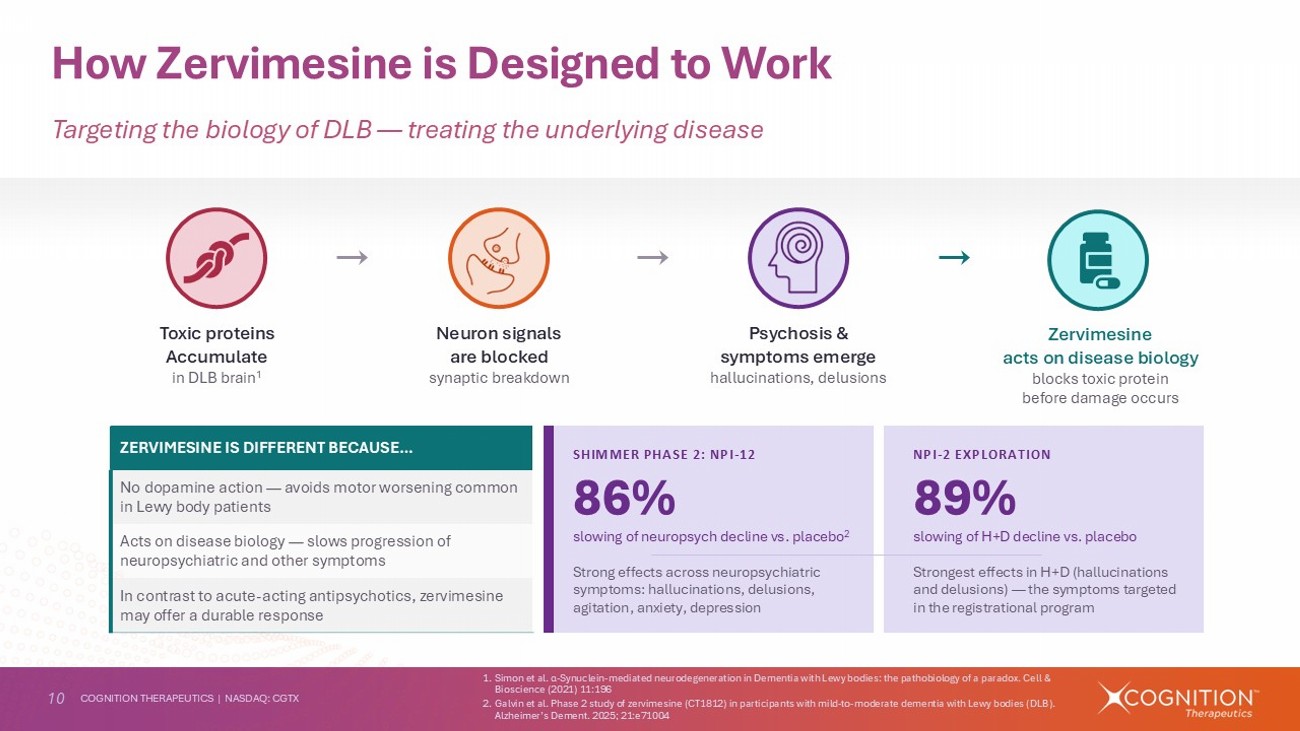
10 COGNITION THERAPEUTICS | NASDAQ: CGTX How Zervimesine is Designed to Work Targeting the biology of DLB — treating the underlying disease Toxic proteins Accumulate in DLB brain 1 Neuron signals are blocked synaptic breakdown Psychosis & symptoms emerge hallucinations, delusions Zervimesine acts on disease biology blocks toxic protein before damage occurs SHIMMER PHASE 2: NPI - 12 86% slowing of neuropsych decline vs. placebo 2 Strong effects across neuropsychiatric symptoms: hallucinations, delusions, agitation, anxiety, depression 1. Simon et al. α - Synuclein - mediated neurodegeneration in Dementia with Lewy bodies: the pathobiology of a paradox. Cell & Bioscience (2021) 11:196 2. Galvin et al. Phase 2 study of zervimesine (CT1812) in participants with mild - to - moderate dementia with Lewy bodies (DLB). Alzheimer’s Dement. 2025; 21:e71004 ZERVIMESINE IS DIFFERENT BECAUSE… No dopamine action — avoids motor worsening common in Lewy body patients Acts on disease biology — slows progression of neuropsychiatric and other symptoms In contrast to acute - acting antipsychotics, zervimesine may offer a durable response NPI - 2 EXPLORATION 89% slowing of H+D decline vs. placebo Strongest effects in H+D (hallucinations and delusions) — the symptoms targeted in the registrational program
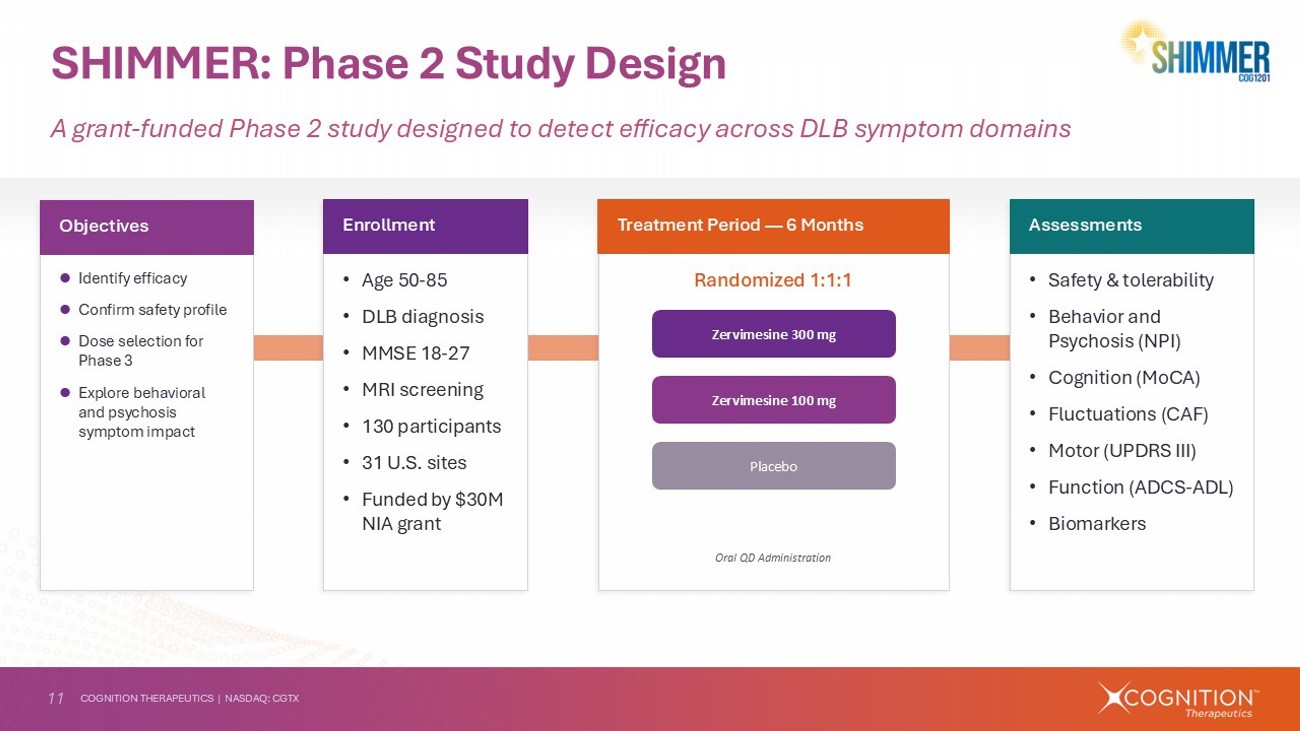
11 COGNITION THERAPEUTICS | NASDAQ: CGTX SHIMMER: Phase 2 Study Design A grant - funded Phase 2 study designed to detect efficacy across DLB symptom domains • Age 50 - 85 • DLB diagnosis • MMSE 18 - 27 • MRI screening • 130 participants • 31 U.S. sites • Funded by $30M NIA grant Enrollment • Safety & tolerability • Behavior and Psychosis (NPI) • Cognition (MoCA) • Fluctuations (CAF) • Motor (UPDRS III) • Function (ADCS - ADL) • Biomarkers Assessments Identify efficacy Confirm safety profile Dose selection for Phase 3 Explore behavioral and psychosis symptom impact Objectives Randomized 1:1:1 Treatment Period — 6 Months Zervimesine 300 mg Zervimesine 100 mg Placebo Oral QD Administration
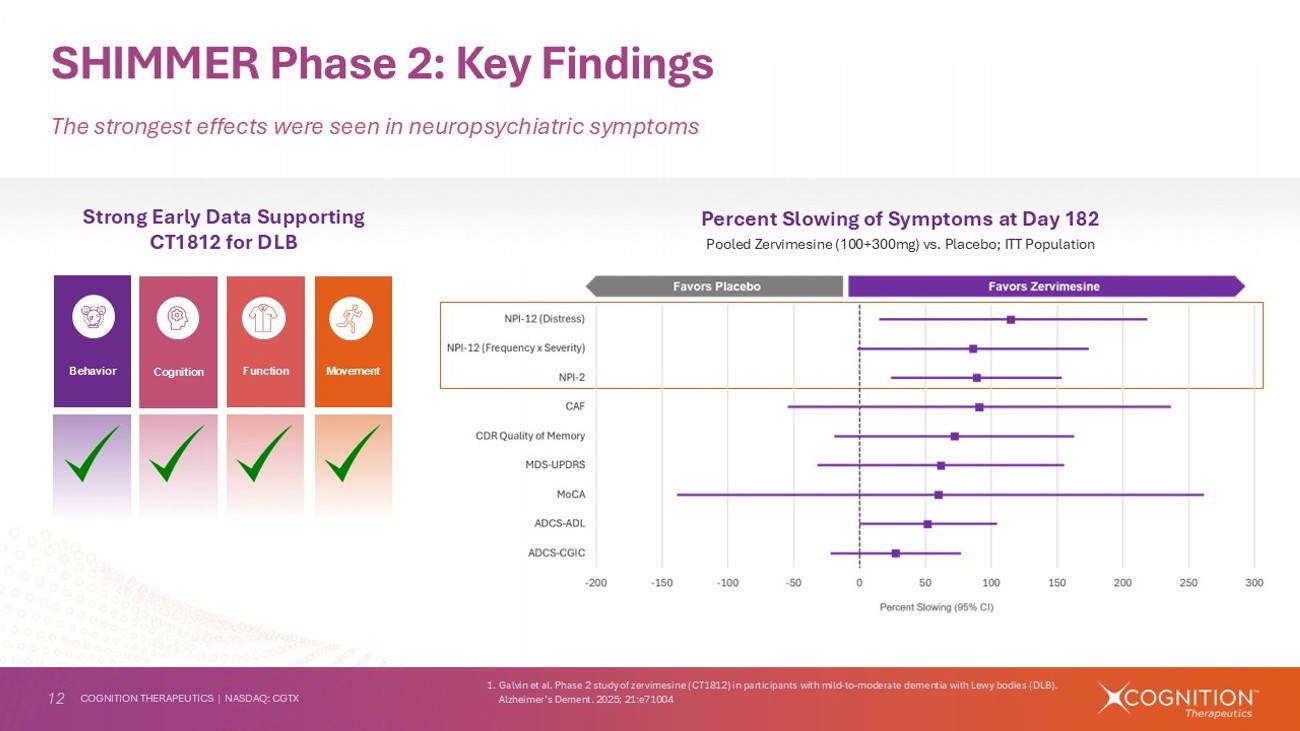
12 COGNITION THERAPEUTICS | NASDAQ: CGTX SHIMMER Phase 2: Key Findings The strongest effects were seen in neuropsychiatric symptoms Strong Early Data Supporting CT1812 for DLB 1. Galvin et al. Phase 2 study of zervimesine (CT1812) in participants with mild - to - moderate dementia with Lewy bodies (DLB). Alzheimer’s Dement. 2025; 21:e71004 Cognition Behavior Movement Function Percent Slowing of Symptoms at Day 182 Pooled Zervimesine (100+300mg) vs. Placebo; ITT Population
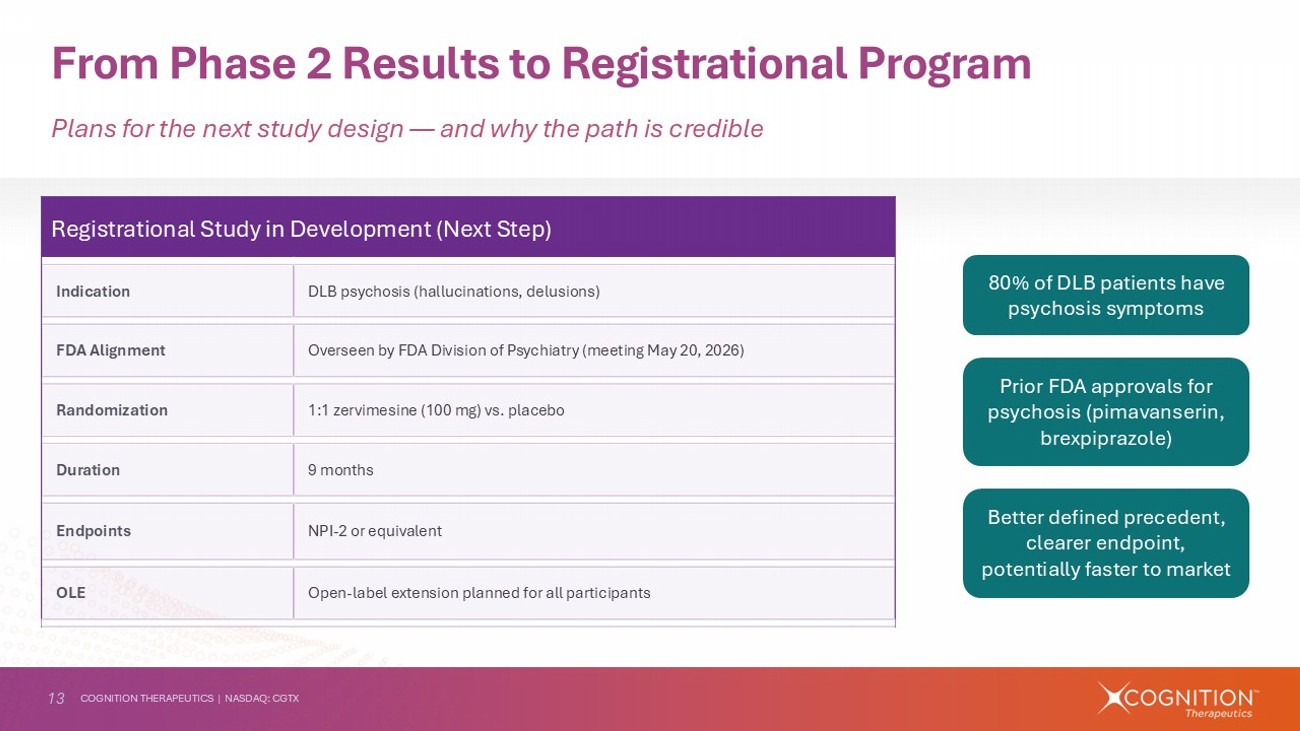
13 COGNITION THERAPEUTICS | NASDAQ: CGTX From Phase 2 Results to Registrational Program Plans for the next study design — and why the path is credible Registrational Study in Development (Next Step) DLB psychosis (hallucinations, delusions) Indication Overseen by FDA Division of Psychiatry (meeting May 20, 2026) FDA Alignment 1:1 zervimesine (100 mg) vs. placebo Randomization 9 months Duration NPI - 2 or equivalent Endpoints Open - label extension planned for all participants OLE 80% of DLB patients have psychosis symptoms Prior FDA approvals for psychosis (pimavanserin, brexpiprazole ) Better defined precedent, clearer endpoint, potentially faster to market
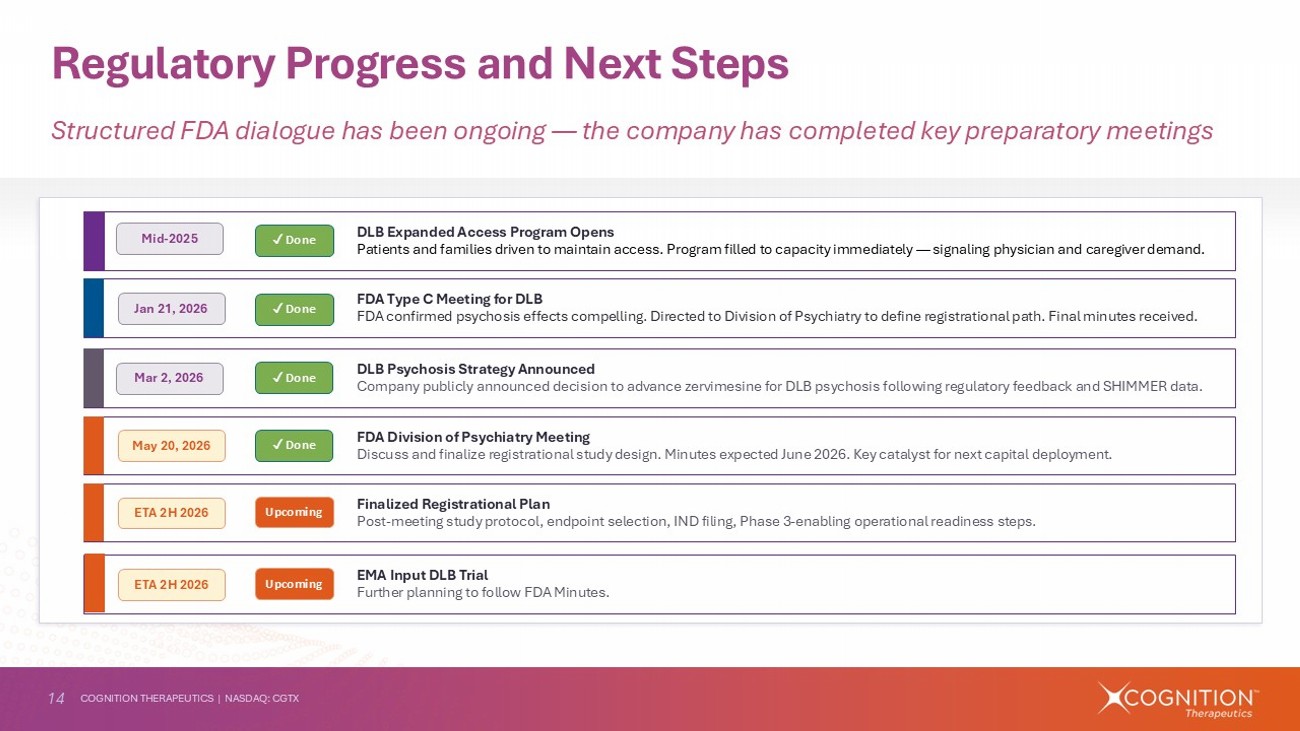
14 COGNITION THERAPEUTICS | NASDAQ: CGTX Regulatory Progress and Next Steps Structured FDA dialogue has been ongoing — the company has completed key preparatory meetings DLB Expanded Access Program Opens Patients and families driven to maintain access. Program filled to capacity immediately — signaling physician and caregiver dema nd. FDA Division of Psychiatry Meeting Discuss and finalize registrational study design. Minutes expected June 2026. Key catalyst for next capital deployment. FDA Type C Meeting for DLB FDA confirmed psychosis effects compelling. Directed to Division of Psychiatry to define registrational path. Final minutes r ece ived. DLB Psychosis Strategy Announced Company publicly announced decision to advance zervimesine for DLB psychosis following regulatory feedback and SHIMMER data. Finalized Registrational Plan Post - meeting study protocol, endpoint selection, IND filing, Phase 3 - enabling operational readiness steps. Mid - 2025 Jan 21, 2026 Mar 2, 2026 May 20, 2026 ETA 2H 2026 ✓ Done ✓ Done ✓ Done Upcoming ✓ Done EMA Input DLB Trial Further planning to follow FDA Minutes. ETA 2H 2026 Upcoming
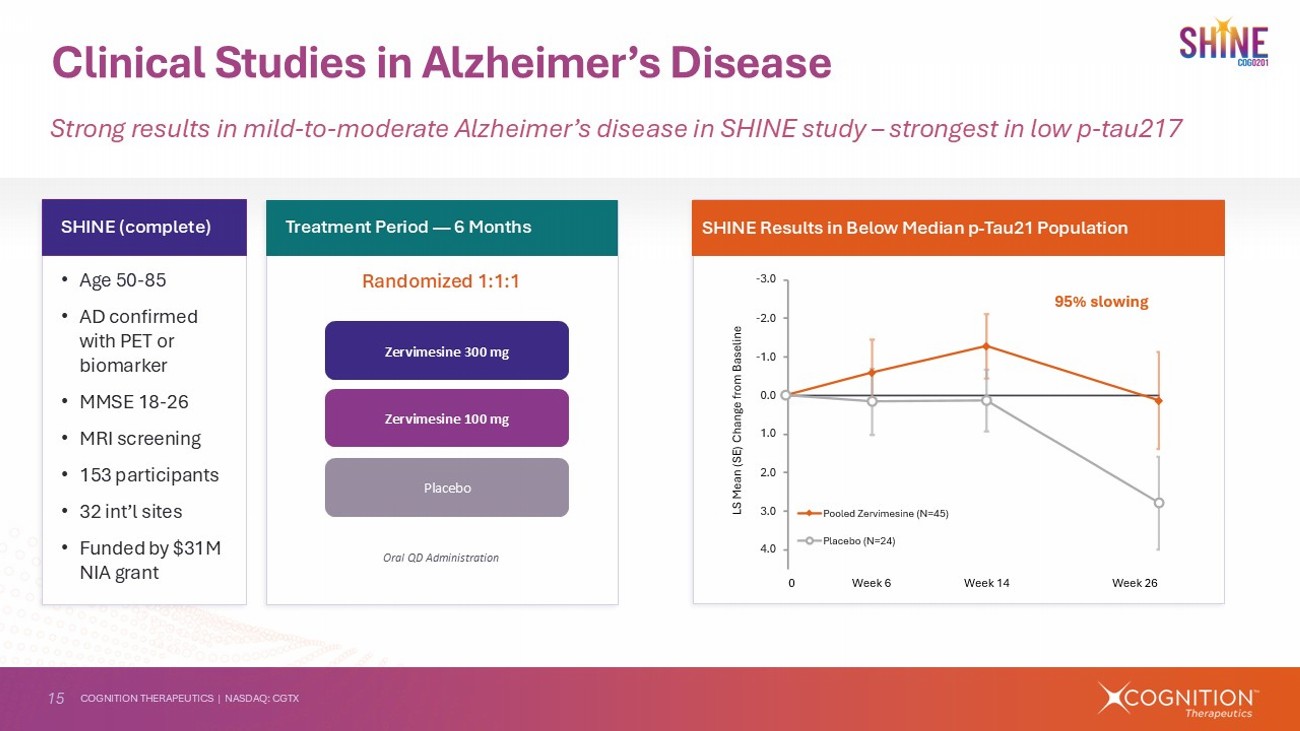
15 COGNITION THERAPEUTICS | NASDAQ: CGTX Clinical Studies in Alzheimer’s Disease Strong results in mild - to - moderate Alzheimer’s disease in SHINE study – strongest in low p - tau217 • Age 50 - 85 • AD confirmed with PET or biomarker • MMSE 18 - 26 • MRI screening • 153 participants • 32 int’l sites • Funded by $31M NIA grant SHINE (complete) Randomized 1:1:1 Treatment Period — 6 Months Zervimesine 300 mg Placebo Oral QD Administration Zervimesine 100 mg SHINE Results in Below Median p - Tau21 Population ϱ ͒ ϟ ͏ ϱ ͑ ϟ ͏ ϱ ͐ ϟ ͏ ͏ ϟ ͏ ͐ ϟ ͏ ͑ ϟ ͏ ͒ ϟ ͏ ͓ ϟ ͏ „ĺĺīôîϙ¾ôŘŽĖıôŜĖIJôϙ ϼ b ѱ ͓͔ Ͻ „īÍèôæĺϙ ϼ b ѱ ͓͑ Ͻ [‹ϙaôÍIJϙ ϼ ‹( Ͻϙ ēÍIJČôϙċŘĺıϙŜôīĖIJô ®ôôħϙ ͕͑ ®ôôħϙ ͓͐ ®ôôħϙ ͕ ͏ ͔͘ ҇ϙ ŜīĺſĖIJČϙ ͏ ϟ ͏͗͏ ͏ ϟ ͕͐͒ ͏ ϟ ͓͖͏ „ ϱ ŽÍīŪôϙ ϼ ŕĺĺīôîϙŽϙ ŕæĺ Ͻ iæŜôŘŽôîϙťŘôÍťıôIJťϙîĖƯôŘôIJèôϙŕĺĺīôîϙŽϙ ŕæĺ ϡϙ ͑ ϟ ͕͕ϙ ŕť
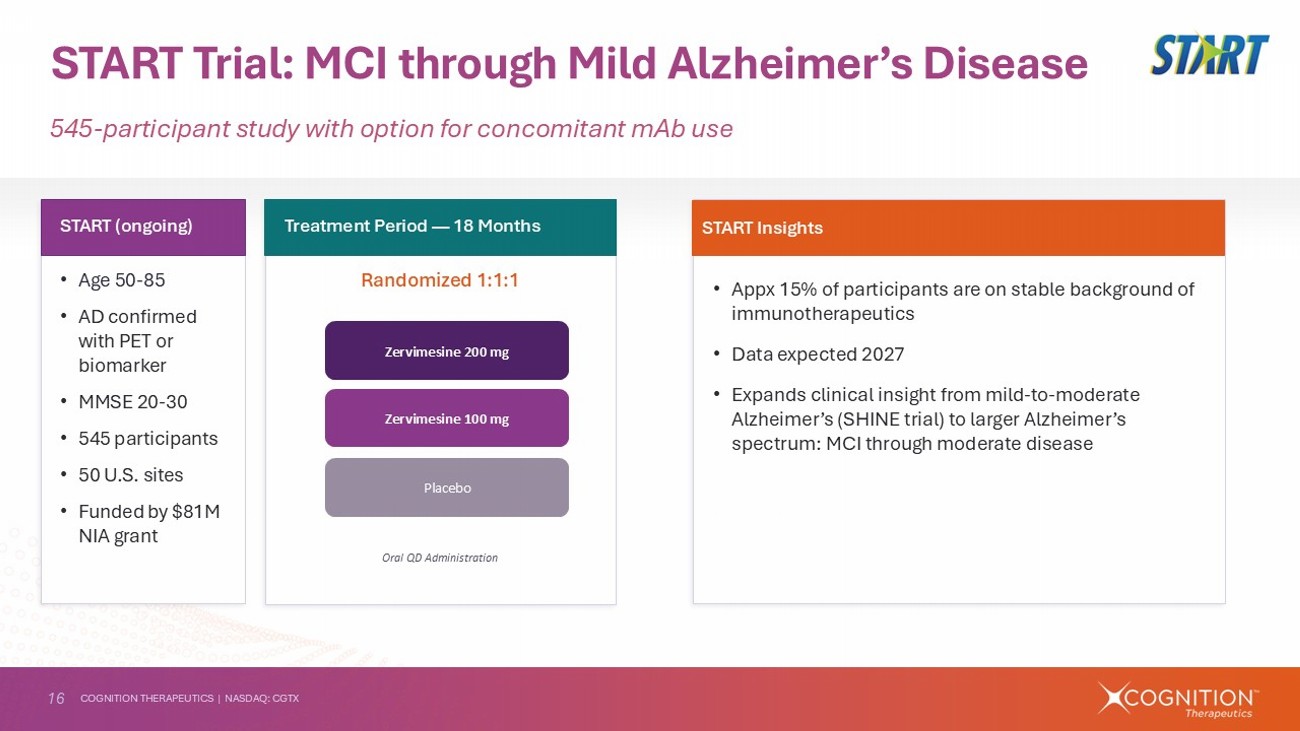
16 COGNITION THERAPEUTICS | NASDAQ: CGTX • Appx 15% of participants are on stable background of immunotherapeutics • Data expected 2027 • Expands clinical insight from mild - to - moderate Alzheimer’s (SHINE trial) to larger Alzheimer’s spectrum: MCI through moderate disease START Trial: MCI through Mild Alzheimer’s Disease 545 - participant study with option for concomitant mAb use • Age 50 - 85 • AD confirmed with PET or biomarker • MMSE 20 - 30 • 545 participants • 50 U.S. sites • Funded by $81M NIA grant START (ongoing) Randomized 1:1:1 Treatment Period — 18 Months Oral QD Administration START Insights Zervimesine 200 mg Placebo Zervimesine 100 mg
17 COGNITION THERAPEUTICS | NASDAQ: CGTX Highly Experienced Management Team Coupled with External Support and Third - Party Validation A team with CNS experience, backed by NIH, analyst consensus, and patient demand NIH/NIA Grant Funding >$170M in non - dilutive grants. $25.6M obligated NIA grant funds remaining (Mar 31, 2026). U.S. government validation of scientific merit. Analyst Consensus 4 covering analysts ( Chardan , HCW, Brookline, B. Riley) all rate CGTX Strong Buy with average 12 - month price target of $3.33 vs. ~$1.23 current price. KOL & Regulator Feedback FDA confirmed psychosis signal compelling and directed company to Division of Psychiatry. KOLs at AD/PD 2026 receptive to DLB psychosis path. Patient Demand EAP reached capacity within days of opening. Patients and physicians continue to request access. Caregiver testimonials confirm real - world impact. External Validation & Support Industry Validation Received funding from prominent industry organizations Key Leadership Lisa Ricciardi President & CEO Led Cognition since 2020 through Phase 2 completions, FDA meetings, and strategic pivot to DLB psychosis. Contact: lricciardi@cogrx.com Anthony Caggiano, MD, PhD Chief Medical Officer Architect of DLB psychosis clinical and registrational plan. Led SHIMMER design and FDA interactions. Contact: acaggiano@cogrx.com John Doyle Chief Financial Officer Leads finance, information technology and investor interactions. Experience at commercial organizations. Contact: jdoyle@cogrx.com