EXHIBIT 99.2
Topic: 26. Gene therapy, cellular immunotherapy and vaccination - Clinical
EHA-7249
First-in-human trial of LB2501, an in vivo CD19/CD20 dual targeting CAR-T therapy, in relapsed/refractory B-Cell NHL
Type: None selected
Xiaoyan Qu1 Yajing Zhang2 Haisheng Liu3 Heng Mei4 Kaiyang Ding5 Jujuan Wang1 Sanmei Wang1 Haorui Shen1 Zhengxu Sun1 Shuangshuang Xing1 Guoai Su2 Zheng Li3 Lin Liu4 Ran Li1 Hailing Liu1 Ling Zhou6 Yinrui Jiang6 Yongxin Luo6 Baoming Ni7 Dong Geng7 Guowei Fang7 Yanjie Xu6 Cong Feng6 Wenjie Wang6 Da Xu6 Zhongyuan Tu6 Hongchen Zheng6 Bing Gao6 Jin Liu6 Lei Fan1
1 The First Affiliated Hospital of Nanjing Medical University, Department of Hematology, Nanjing, China, 2 Beijing GoBroad Boren Hospital, Gobroad Medical Institute of Hematology, Department of Myeloma and Lymphoma, Beijing, China, 3 The Fourth Hospital of Hebei Medical University, Shijiazhuang, China, 4 Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Institute of Hematology, Wuhan, China, 5 The First Affiliated Hospital of USTC Anhui Provincial Hospital, Department of Hematology, Hefei, China, 6 Legend Biotech Co, Nanjing, China, 7 Legend Biotech USA Inc, Somerset, NJ, United States of America
Background
Ex vivo CAR-T therapies have advanced treatment for relapsed/refractory non-Hodgkin lymphoma (R/R NHL) but are limited by complex manufacturing and lymphodepletion. In vivo CAR-T offers an off-the-shelf alternative that generates CAR-T cells directly in patients without requiring lymphodepletion. While feasibility has been shown in multiple myeloma, clinical data for B-cell malignancies remain unreported. LB2501, a third-generation, replication-incompetent lentiviral vector (LVV) pseudotyped with a modified fusion glycoprotein and a CD3 binder for T-cell-specific transduction, encodes a CD19/CD20 dual targeting CAR to generate CAR-T in vivo.
Aims
To evaluate the safety, pharmacokinetics, and preliminary efficacy of LB2501 in R/R B-NHL.
Methods
This ongoing phase 1 trial (NCT07002112) enrolled patients with measurable R/R NHL who had primary refractory disease or progression after ≥2 prior lines of therapy. A 3+3 dose-escalation design with backfilling was used across dose levels (DLs). LB2501 was administered as a single intravenous infusion without lymphodepletion.
Results
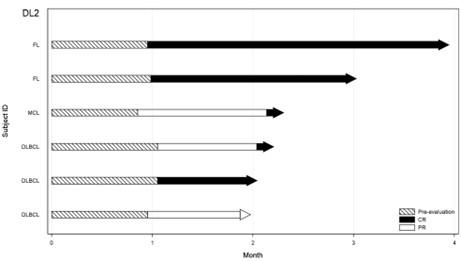
As of April 1, 2026, 12 patients had been dosed with LB2501 at DL1 (n=6) or DL2 (n=6). The median age was 58.5 years, median prior therapy lines was 3, and 58.3% were refractory to last line. Patients included 7 (58.3%) LBCL, 3 (25%) FL and 2 (16.7%) MCL. No DLT, SAE or fatal cases were reported. Infusion-related reactions occurred in 9 patients (75.0%); all were grade 1 or 2, resolved within a median of 2.0 days, and required no tocilizumab or glucocorticoids. Cytokine release syndrome (CRS) occurred in 66.7% patients (grade 1 in 58.3%, grade 2 in 8.3%); No neurotoxicity (ICANS) was observed. Grade≥3 LVV-related and CAR-T-related adverse events were limited to decreased lymphocyte count (33.3% each) and decreased neutrophil count (25.0% and 50.0%, respectively). The objective response rate (ORR) was 50% (6/12), with a complete response rate (CR) of 41.7% (5/12). At DL2, the ORR was 100% (6/6) and the CR was 83.3% (5/6). All responses were ongoing at cut-off date (Figure 1). The median follow-up for DL2 was 2.2 months (range, 2.0 to 3.8). PK analysis via qPCR confirmed dose-dependent in vivo CAR-T cell expansion in 83% (5/6) of patients at DL1 and 100% (6/6) at DL2. At DL2, the median Cmax was 109,117.5 copies/μg DNA (vs. 1,068.0 at DL1), with a median Tmax of 15.0 days. At the time of data cutoff, patients exhibited persistent PK, with CAR-T cells detectable in peripheral blood for up to 116 days. Insertion site analyses indicate in vivo transduction is highly T cell specific, polyclonal, and diverse with mostly single copy insertion per T cell. The median VCN for in vivo CAR-T was 1.05, lower than ex vivo manufactured CAR-T.
Summary/Conclusion
This study represents the initial clinical cohort of in vivo CAR-T therapy in relapsed/refractory non-Hodgkin lymphoma. LB2501, a first-in-class CD19/CD20 dual-targeting in vivo vector, introduces a novel paradigm by eliminating the need for ex vivo manufacturing and lymphodepletion. LB2501 has demonstrated a favorable safety profile and encouraging efficacy with a 100% ORR and 83.3% CR at DL2. While a longer-follow up is warranted, these data highlight the potential of LB2501 as a scalable, readily accessible “off-the-shelf” immunotherapy for B-cell malignancies.
Figure 1: Patient Responses to DL2