Exhibit 99.2
| 1 | © 2026 Aprea Therapeutics, Inc. All Rights Reserved A clinical-stage precision medicine oncology company focused on the discovery and development of targeted therapies for patients with biomarker-defined cancers May 2026 |
| 2 | © 2026 Aprea Therapeutics, Inc. All Rights Reserved Forward-Looking Statements Certain information contained in this presentation includes “forward-looking statements”, within the meaning of Section 27A of the Securities Act of 1933, as amended, and Section 21E of the Securities Exchange Act of 1934, as amended related to our study analyses, clinical trials, regulatory submissions, and projected cash position. We may, in some cases use terms such as “future,” “predicts,” “believes,” “potential,” “continue,” “anticipates,” “estimates,” “expects,” “plans,” “intends,” “targeting,” “confidence,” “may,” “could,” “might,” “likely,” “will,” “should” or other words that convey uncertainty of the future events or outcomes to identify these forward-looking statements. Our forward-looking statements are based on current beliefs and expectations of our management team and on information currently available to management that involve risks, potential changes in circumstances, assumptions, and uncertainties. All statements contained in this presentation other than statements of historical fact are forward-looking statements, including statements regarding our ability to develop, commercialize, and achieve market acceptance of our current and planned products and services, our research and development efforts, including timing considerations and other matters regarding our business strategies, use of capital, results of operations and financial position, and plans and objectives for future operations. Any or all of the forward-looking statements may turn out to be wrong or be affected by inaccurate assumptions we might make or by known or unknown risks and uncertainties. These forward-looking statements are subject to risks and uncertainties including, without limitation, risks related to the success, timing, and cost of our ongoing clinical trials and anticipated clinical trials for our current product candidates, including statements regarding the timing of initiation, pace of enrollment and completion of the trials (including our ability to fully fund our disclosed clinical trials, which assumes no material changes to our currently projected expenses), futility analyses, presentations at conferences and data reported in an abstract, and receipt of interim or preliminary results (including, without limitation, any preclinical results or data), which are not necessarily indicative of the final results of our ongoing clinical trials, our understanding of product candidates mechanisms of action and interpretation of preclinical and early clinical results from its clinical development programs and our ability to predict clinical outcomes based on such preclinical and early clinical result and the other risks, uncertainties, and other factors described under “Risk Factors,” “Management’s Discussion and Analysis of Financial Condition and Results of Operations” and elsewhere in the documents we file with the U.S. Securities and Exchange Commission. For all these reasons, actual results and developments could be materially different from those expressed in or implied by our forward-looking statements. You are cautioned not to place undue reliance on these forward-looking statements, which are made only as of the date of this presentation. We undertake no obligation to update such forward-looking statements for any reason, except as required by law. This presentation shall not constitute an offer to sell or the solicitation of an offer to buy any securities, nor shall there be any sale of any securities in any state or jurisdiction in which such offer, solicitation or sale would be unlawful prior to registration or qualification under the securities laws of any such state or jurisdiction. This presentation may not be reproduced, forwarded to any person or published, in whole or in part. |
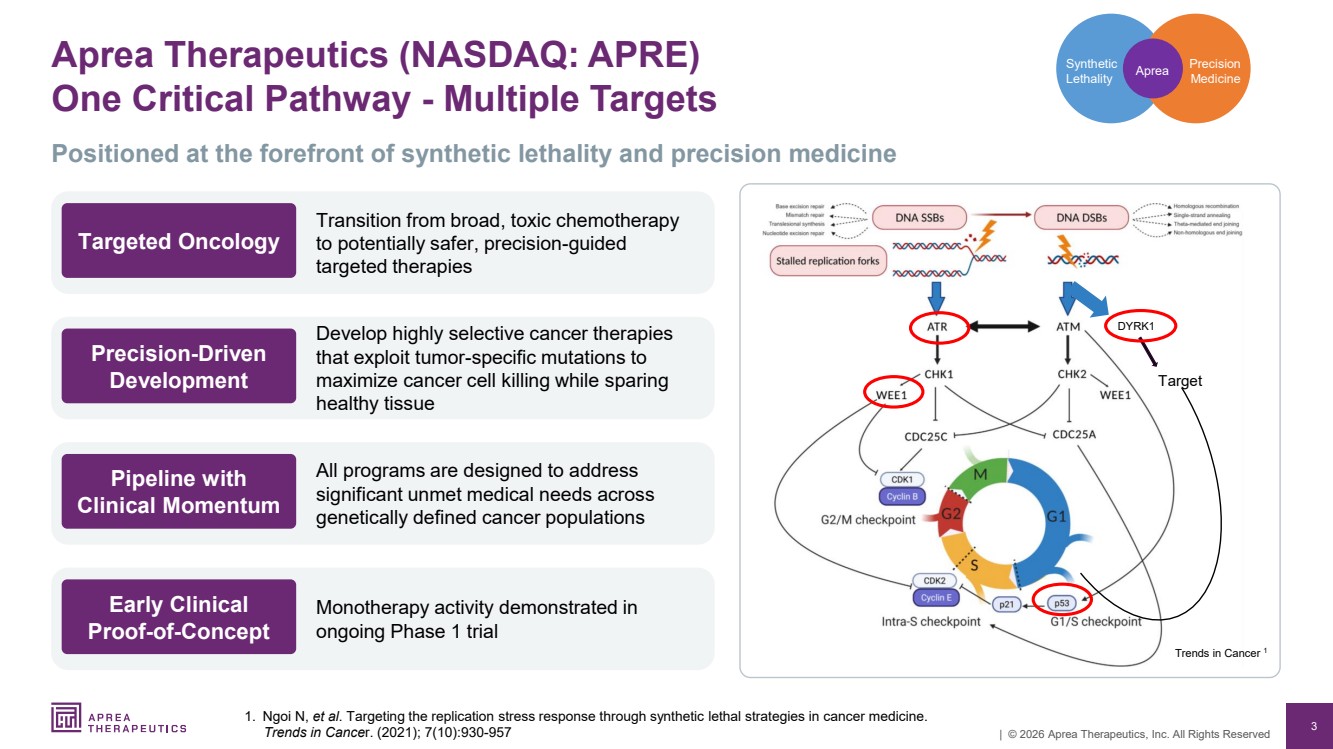
| 3 | © 2026 Aprea Therapeutics, Inc. All Rights Reserved Aprea Therapeutics (NASDAQ: APRE) One Critical Pathway - Multiple Targets 1. Ngoi N, et al. Targeting the replication stress response through synthetic lethal strategies in cancer medicine. Trends in Cancer. (2021); 7(10):930-957 Precision Medicine Synthetic Lethality Aprea DYRK1 Target Trends in Cancer 1 Positioned at the forefront of synthetic lethality and precision medicine Transition from broad, toxic chemotherapy to potentially safer, precision-guided targeted therapies Targeted Oncology Develop highly selective cancer therapies that exploit tumor-specific mutations to maximize cancer cell killing while sparing healthy tissue Precision-Driven Development All programs are designed to address significant unmet medical needs across genetically defined cancer populations Pipeline with Clinical Momentum Monotherapy activity demonstrated in ongoing Phase 1 trial Early Clinical Proof-of-Concept |
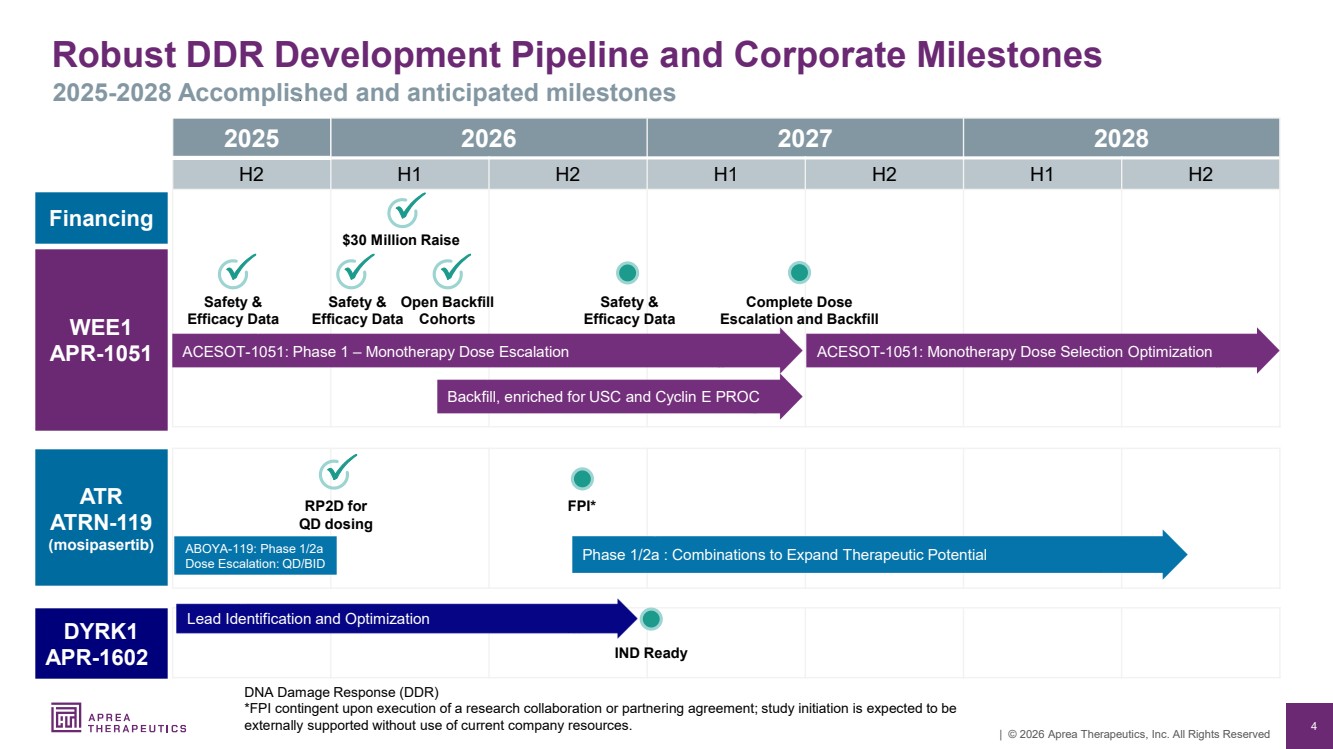
| 4 | © 2026 Aprea Therapeutics, Inc. All Rights Reserved Robust DDR Development Pipeline and Corporate Milestones 2025-2028 Accomplished and anticipated milestones 2025 2026 2027 2028 H2 H1 H2 H1 H2 H1 H2 ATR ATRN-119 (mosipasertib) WEE1 APR-1051 RP2D for QD dosing ACESOT-1051: Phase 1 – Monotherapy Dose Escalation Complete Dose Escalation and Backfill ACESOT-1051: Monotherapy Dose Selection Optimization Safety & Efficacy Data Safety & Efficacy Data Phase 1/2a : Combinations to Expand Therapeutic Potential Open Backfill Cohorts DYRK1 APR-1602 Lead Identification and Optimization ABOYA-119: Phase 1/2a Dose Escalation: QD/BID Safety & Efficacy Data DNA Damage Response (DDR) *FPI contingent upon execution of a research collaboration or partnering agreement; study initiation is expected to be externally supported without use of current company resources. FPI* IND Ready Financing $30 Million Raise Backfill, enriched for USC and Cyclin E PROC |
| 5 | © 2026 Aprea Therapeutics, Inc. All Rights Reserved Strong Drug Development and Commercial Expertise Experienced team in synthetic lethality and targeted therapy Management Board of Directors Richard Peters, MD, PhD Chairman of the Board Oren Gilad, PhD President and CEO Jean-Pierre Bizzari, MD Director Marc Duey Director Michael Grissinger Director Gabriela Gruia, MD Director John Henneman Director Rifat Pamukcu, MD Director Bernd R. Seizinger, MD, PhD Director Oren Gilad, PhD President and CEO John P. Hamill SVP and CFO Eugene Kennedy, MD Chief Medical Advisor Ze’ev Weiss, CPA, BSc Chief Business Advisor Mike Carleton, PhD Translational Medicine Advisor Brian Wiley SVP, Corporate Strategy |
| 6 | © 2026 Aprea Therapeutics, Inc. All Rights Reserved 6 WEE1 Inhibitor: APR-1051 ACESOT-1051: Clinical Proof-Of-Concept |
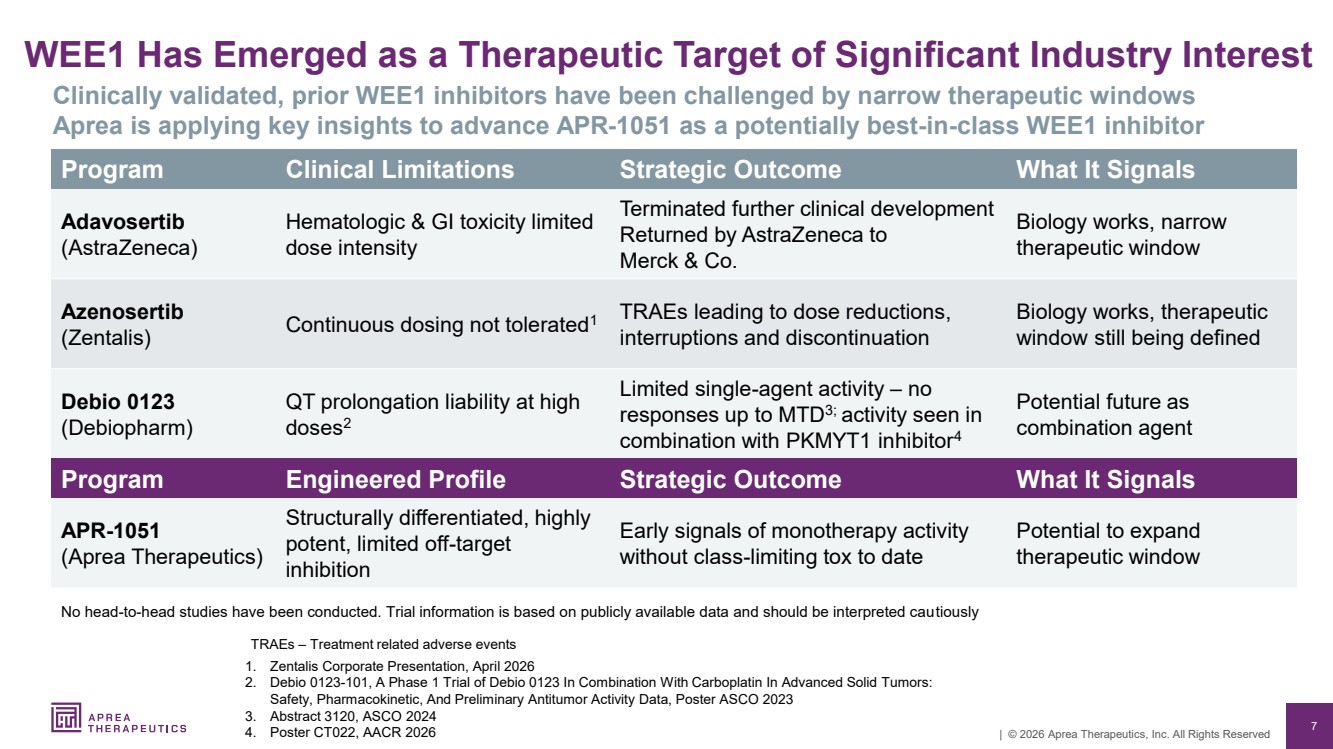
| 7 | © 2026 Aprea Therapeutics, Inc. All Rights Reserved WEE1 Has Emerged as a Therapeutic Target of Significant Industry Interest 1. Zentalis Corporate Presentation, April 2026 2. Debio 0123-101, A Phase 1 Trial of Debio 0123 In Combination With Carboplatin In Advanced Solid Tumors: Safety, Pharmacokinetic, And Preliminary Antitumor Activity Data, Poster ASCO 2023 3. Abstract 3120, ASCO 2024 4. Poster CT022, AACR 2026 Clinically validated, prior WEE1 inhibitors have been challenged by narrow therapeutic windows Aprea is applying key insights to advance APR-1051 as a potentially best-in-class WEE1 inhibitor Program Clinical Limitations Strategic Outcome What It Signals Adavosertib (AstraZeneca) Hematologic & GI toxicity limited dose intensity Terminated further clinical development Returned by AstraZeneca to Merck & Co. Biology works, narrow therapeutic window Azenosertib (Zentalis) Continuous dosing not tolerated1 TRAEs leading to dose reductions, interruptions and discontinuation Biology works, therapeutic window still being defined Debio 0123 (Debiopharm) QT prolongation liability at high doses2 Limited single-agent activity – no responses up to MTD3; activity seen in combination with PKMYT1 inhibitor4 Potential future as combination agent No head-to-head studies have been conducted. Trial information is based on publicly available data and should be interpreted cautiously Program Engineered Profile Strategic Outcome What It Signals APR-1051 (Aprea Therapeutics) Structurally differentiated, highly potent, limited off-target inhibition Early signals of monotherapy activity without class-limiting tox to date Potential to expand therapeutic window TRAEs – Treatment related adverse events |
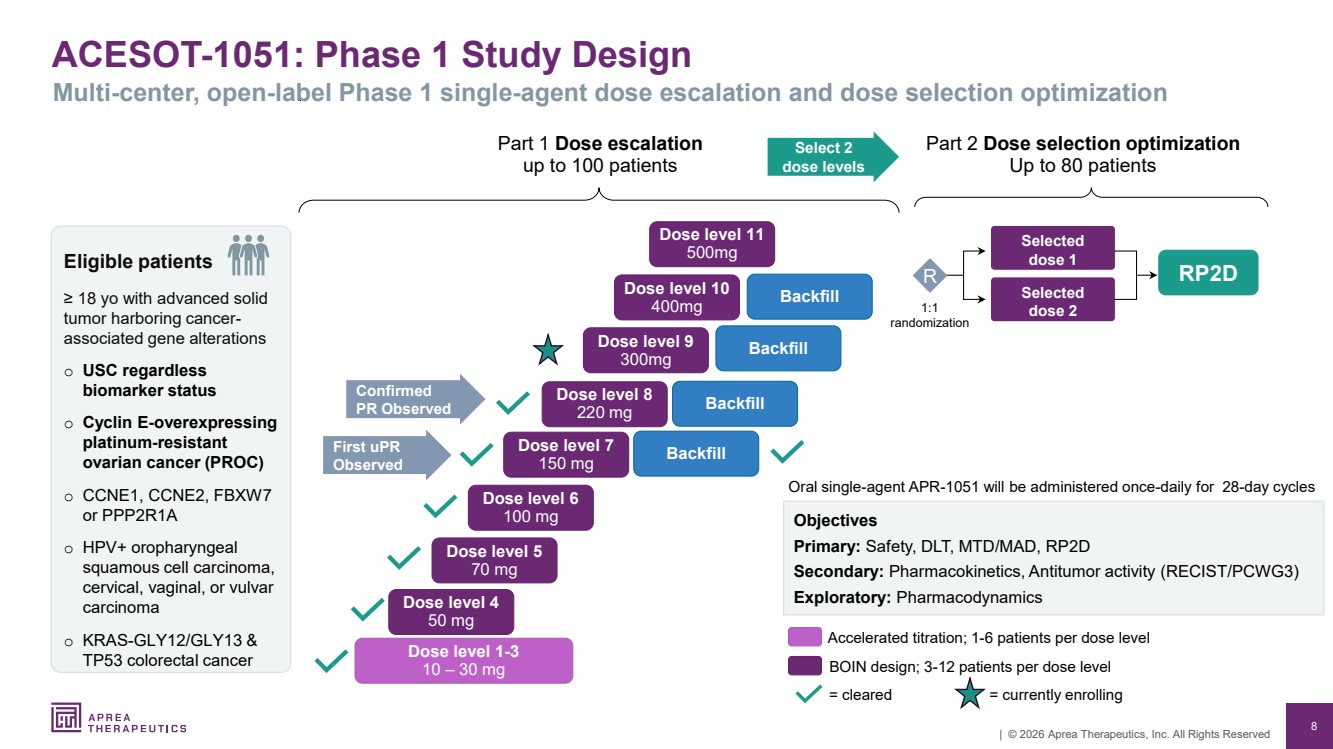
| 8 | © 2026 Aprea Therapeutics, Inc. All Rights Reserved ACESOT-1051: Phase 1 Study Design Multi-center, open-label Phase 1 single-agent dose escalation and dose selection optimization Part 1 Dose escalation up to 100 patients RP2D Oral single-agent APR-1051 will be administered once-daily for 28-day cycles Objectives Primary: Safety, DLT, MTD/MAD, RP2D Secondary: Pharmacokinetics, Antitumor activity (RECIST/PCWG3) Exploratory: Pharmacodynamics = cleared Accelerated titration; 1-6 patients per dose level BOIN design; 3-12 patients per dose level Part 2 Dose selection optimization Up to 80 patients Selected dose 2 Selected dose 1 1:1 randomization R Dose level 1-3 10 – 30 mg Dose level 4 50 mg Dose level 5 70 mg Dose level 6 100 mg Dose level 7 150 mg Dose level 8 220 mg Dose level 9 300mg Confirmed PR Observed First uPR Observed Select 2 dose levels Eligible patients ≥ 18 yo with advanced solid tumor harboring cancer-associated gene alterations o USC regardless biomarker status o Cyclin E-overexpressing platinum-resistant ovarian cancer (PROC) o CCNE1, CCNE2, FBXW7 or PPP2R1A o HPV+ oropharyngeal squamous cell carcinoma, cervical, vaginal, or vulvar carcinoma o KRAS-GLY12/GLY13 & TP53 colorectal cancer = currently enrolling Backfill Backfill Backfill Dose level 10 400mg Dose level 11 500mg Backfill |
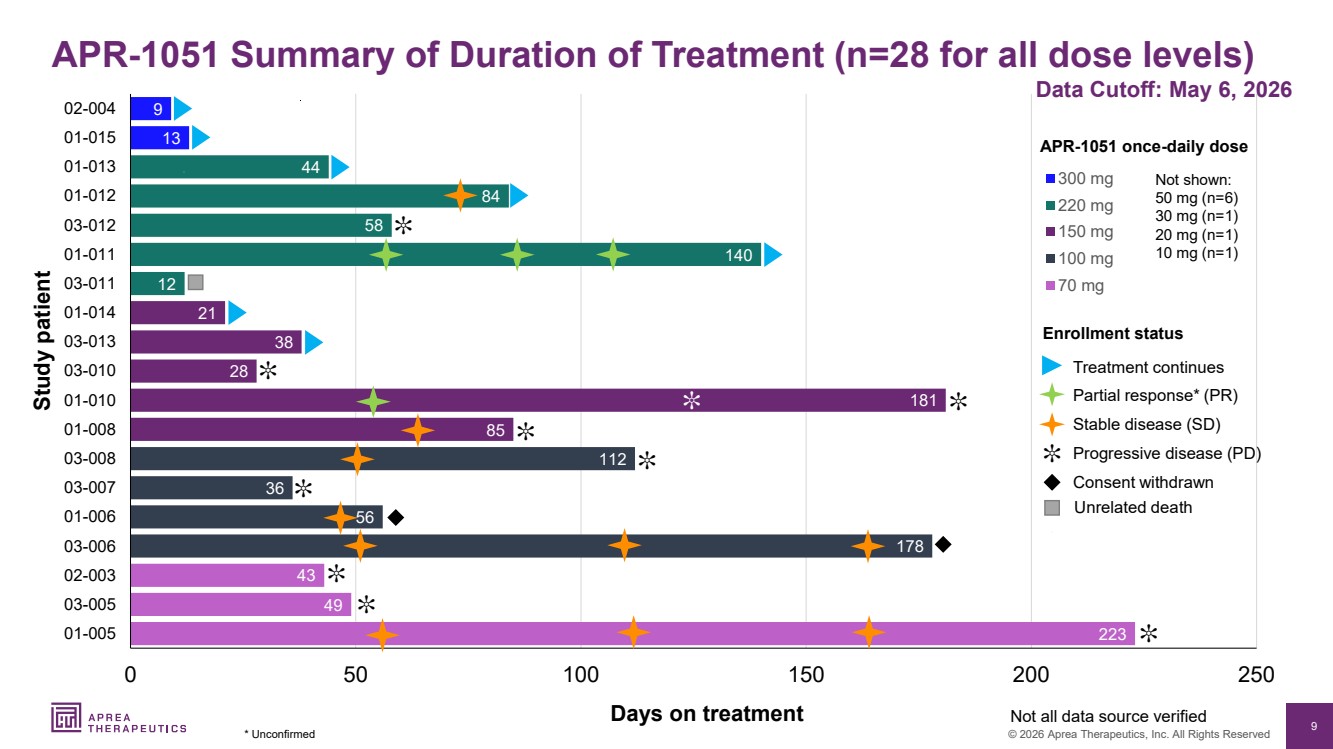
| 9 © 2026 Aprea Therapeutics, Inc. All Rights Reserved 223 49 43 178 56 36 112 85 181 28 38 21 12 140 58 84 44 13 9 0 50 100 150 200 250 01-005 03-005 02-003 03-006 01-006 03-007 03-008 01-008 01-010 03-010 03-013 01-014 03-011 01-011 03-012 01-012 01-013 01-015 02-004 300 mg 220 mg 150 mg 100 mg 70 mg Days on treatment Study patient APR-1051 once-daily dose Not all data source verified Data Cutoff: May 6, 2026 APR-1051 Summary of Duration of Treatment (n=28 for all dose levels) * Unconfirmed ✼ Progressive disease (PD) Stable disease (SD) Consent withdrawn Treatment continues Unrelated death Partial response* (PR) Enrollment status ✼ ✼ ✼ ✼ ✼ ✼ ✼ ✼ ✼ ✼ Not shown: 50 mg (n=6) 30 mg (n=1) 20 mg (n=1) 10 mg (n=1) |
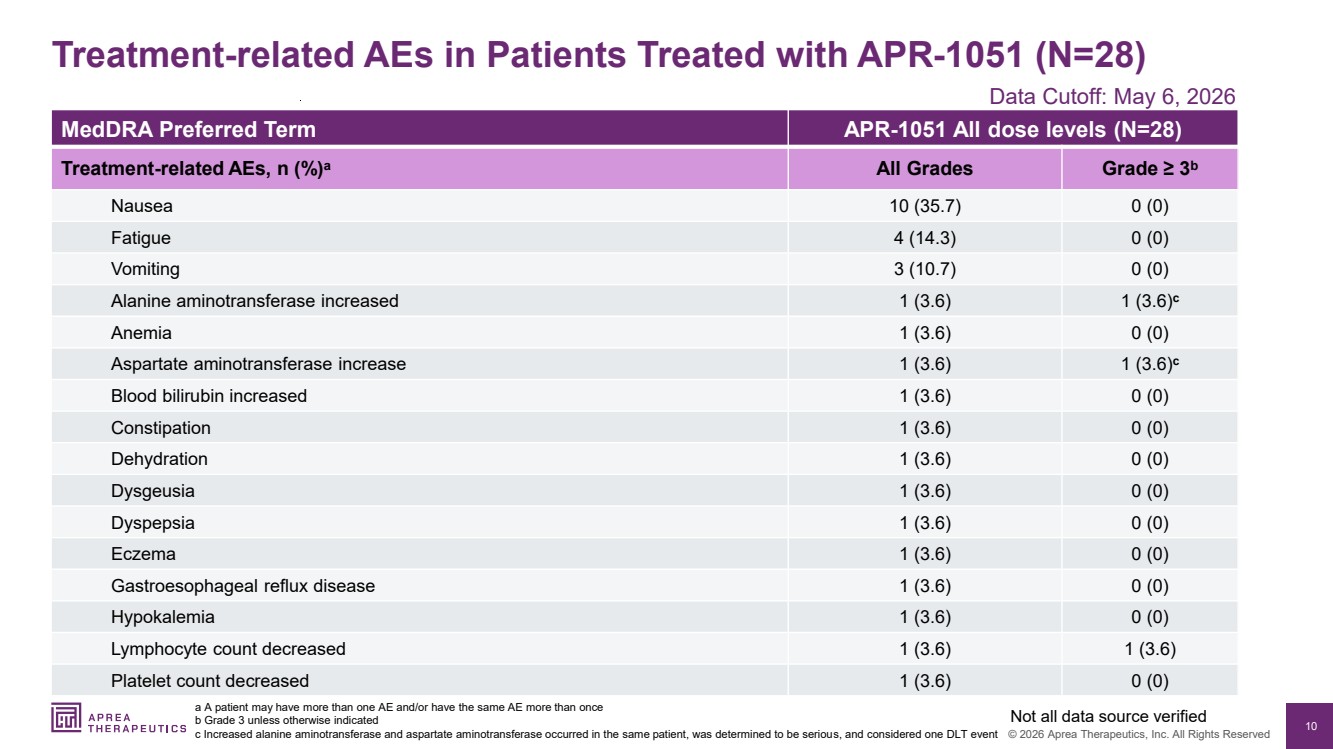
| 10 © 2026 Aprea Therapeutics, Inc. All Rights Reserved MedDRA Preferred Term APR-1051 All dose levels (N=28) Treatment-related AEs, n (%)a All Grades Grade ≥ 3b Nausea 10 (35.7) 0 (0) Fatigue 4 (14.3) 0 (0) Vomiting 3 (10.7) 0 (0) Alanine aminotransferase increased 1 (3.6) 1 (3.6)c Anemia 1 (3.6) 0 (0) Aspartate aminotransferase increase 1 (3.6) 1 (3.6)c Blood bilirubin increased 1 (3.6) 0 (0) Constipation 1 (3.6) 0 (0) Dehydration 1 (3.6) 0 (0) Dysgeusia 1 (3.6) 0 (0) Dyspepsia 1 (3.6) 0 (0) Eczema 1 (3.6) 0 (0) Gastroesophageal reflux disease 1 (3.6) 0 (0) Hypokalemia 1 (3.6) 0 (0) Lymphocyte count decreased 1 (3.6) 1 (3.6) Platelet count decreased 1 (3.6) 0 (0) Treatment-related AEs in Patients Treated with APR-1051 (N=28) a A patient may have more than one AE and/or have the same AE more than once b Grade 3 unless otherwise indicated c Increased alanine aminotransferase and aspartate aminotransferase occurred in the same patient, was determined to be serious, and considered one DLT event Not all data source verified Data Cutoff: May 6, 2026 |
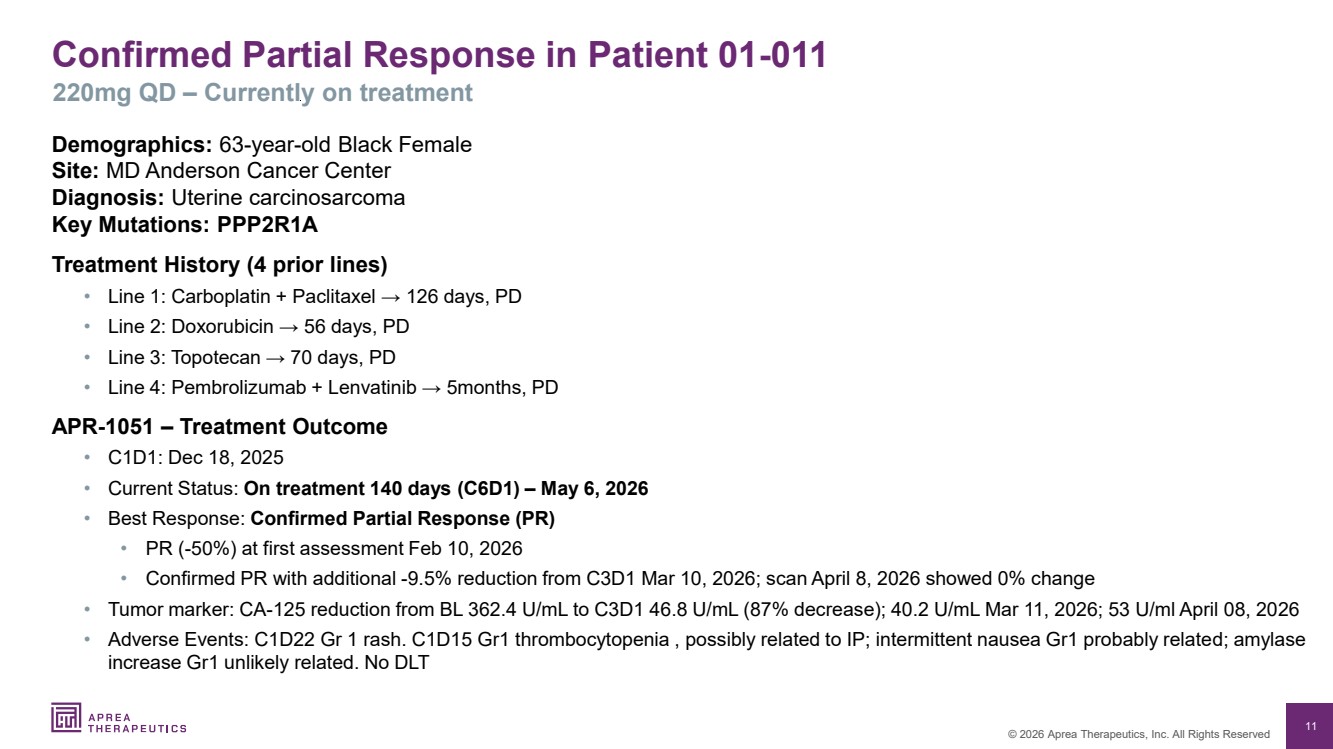
| 11 © 2026 Aprea Therapeutics, Inc. All Rights Reserved Confirmed Partial Response in Patient 01-011 220mg QD – Currently on treatment Demographics: 63-year-old Black Female Site: MD Anderson Cancer Center Diagnosis: Uterine carcinosarcoma Key Mutations: PPP2R1A Treatment History (4 prior lines) • Line 1: Carboplatin + Paclitaxel → 126 days, PD • Line 2: Doxorubicin → 56 days, PD • Line 3: Topotecan → 70 days, PD • Line 4: Pembrolizumab + Lenvatinib → 5months, PD APR-1051 – Treatment Outcome • C1D1: Dec 18, 2025 • Current Status: On treatment 140 days (C6D1) – May 6, 2026 • Best Response: Confirmed Partial Response (PR) • PR (-50%) at first assessment Feb 10, 2026 • Confirmed PR with additional -9.5% reduction from C3D1 Mar 10, 2026; scan April 8, 2026 showed 0% change • Tumor marker: CA-125 reduction from BL 362.4 U/mL to C3D1 46.8 U/mL (87% decrease); 40.2 U/mL Mar 11, 2026; 53 U/ml April 08, 2026 • Adverse Events: C1D22 Gr 1 rash. C1D15 Gr1 thrombocytopenia , possibly related to IP; intermittent nausea Gr1 probably related; amylase increase Gr1 unlikely related. No DLT |
| 12 | © 2026 Aprea Therapeutics, Inc. All Rights Reserved Disease Control Observed in Early Patient Outcomes APR-1051 shows single agent activity in rectal cancer with mutated FBXW7 100 mg Cohort Case Report Patient: 86-year-old Asian Female Diagnosis: Rectal Cancer Key Mutations: FBXW7 (Drives Cyclin E accumulation and overexpression) Treatment History: 5 prior lines - heavily pretreated • Line 1: Capecitabine/oxaliplatin → 191 days, PD • Line 2: Capecitabine/oxaliplatin/bevacizumab → 45 days, PD • Line 3: FOLFIRI + bevacizumab → 43 days, PD • Line 4: Local XRT (lung mets) → 12 days, not evaluable • Line 5: Tretinoin/bevacizumab/Tecentriq (ATRT trial) → 50 days, PD APR-1051 Activity: • Current Status: Consent withdrawn after 178 days • Best Response: SD at third scan (-15% tumor response) Notes: Durable SD maintained 181 days in a heavily pretreated 86-year-old patient; well tolerated with minimal toxicity. FBXW7 mutation may be relevant to response Stable disease maintained for 178 days in patient with FBXW7 mutation (100 mg QD) (elected to stop study participation) |
| 13 | © 2026 Aprea Therapeutics, Inc. All Rights Reserved 70 mg Cohort Case Report Disease Control Observed in Early Patient Outcomes Patient: 62-year-old White Male Diagnosis: HPV+ Oropharyngeal Squamous Cell Carcinoma (base of tongue) Key Mutations: P16+ Treatment History: 3 prior lines • Line 1: Concomitant cisplatin/XRT → 49 days, PD • Line 2: Pembrolizumab→ 84 days, PD • Line 3: Paclitaxel/carboplatin → 184 days, PD APR-1051 Activity • Current Status: PD after 223 days of SD treatment • Best Response: SD at first scan (-5% tumor response) Notes: Stable disease maintained for 223 days. APR-1051 shows single agent activity in HPV+ head and neck cancer Stable disease maintained for 223 days in patient 01-005 HPV+ head and neck cancer (70 mg QD) (PD) |
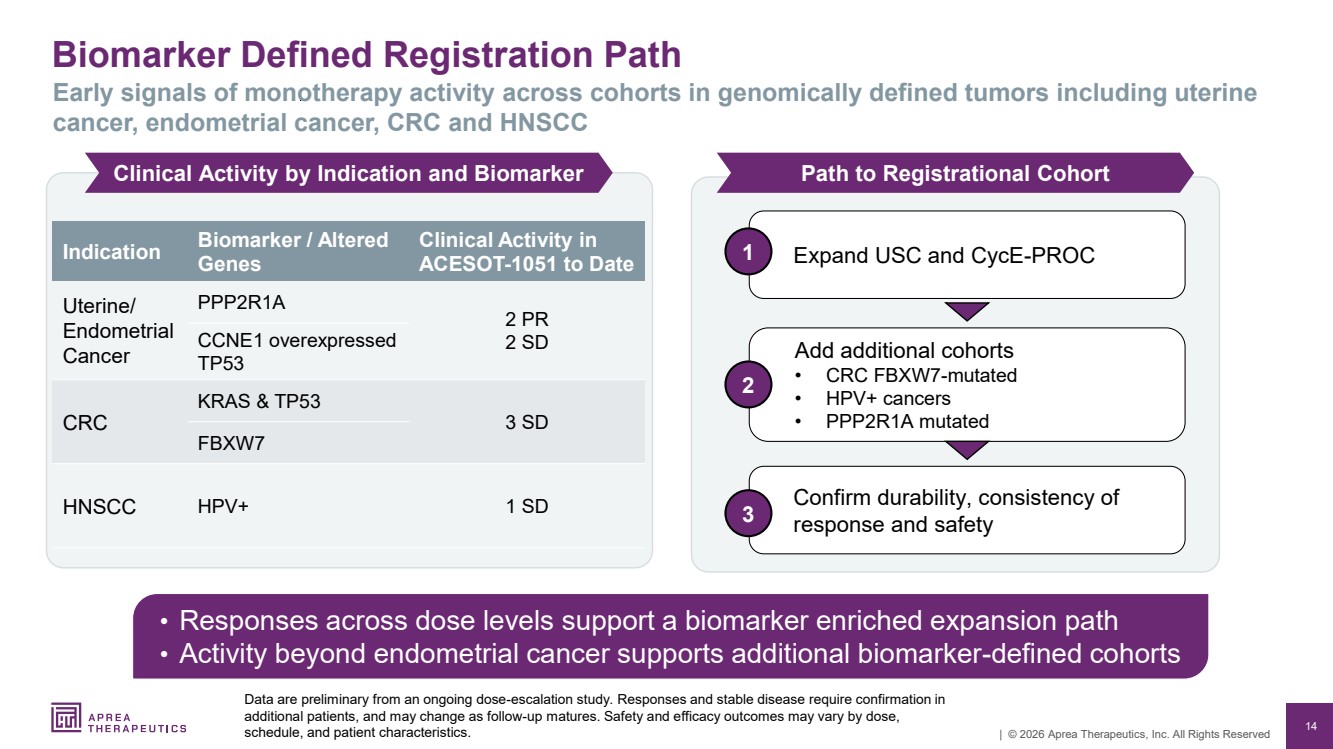
| 14 | © 2026 Aprea Therapeutics, Inc. All Rights Reserved Biomarker Defined Registration Path Data are preliminary from an ongoing dose-escalation study. Responses and stable disease require confirmation in additional patients, and may change as follow-up matures. Safety and efficacy outcomes may vary by dose, schedule, and patient characteristics. Early signals of monotherapy activity across cohorts in genomically defined tumors including uterine cancer, endometrial cancer, CRC and HNSCC • Responses across dose levels support a biomarker enriched expansion path • Activity beyond endometrial cancer supports additional biomarker-defined cohorts Clinical Activity by Indication and Biomarker Path to Registrational Cohort 1 Expand USC and CycE-PROC Add additional cohorts • CRC FBXW7-mutated • HPV+ cancers • PPP2R1A mutated 2 Confirm durability, consistency of response and safety 3 Indication Biomarker / Altered Genes Clinical Activity in ACESOT-1051 to Date Uterine/ Endometrial Cancer PPP2R1A 2 PR CCNE1 overexpressed 2 SD TP53 CRC KRAS & TP53 3 SD FBXW7 HNSCC HPV+ 1 SD |
| 15 | © 2026 Aprea Therapeutics, Inc. All Rights Reserved 15 APR-1051: Potentially Differentiated WEE1 Inhibitor Pre-Clinical |
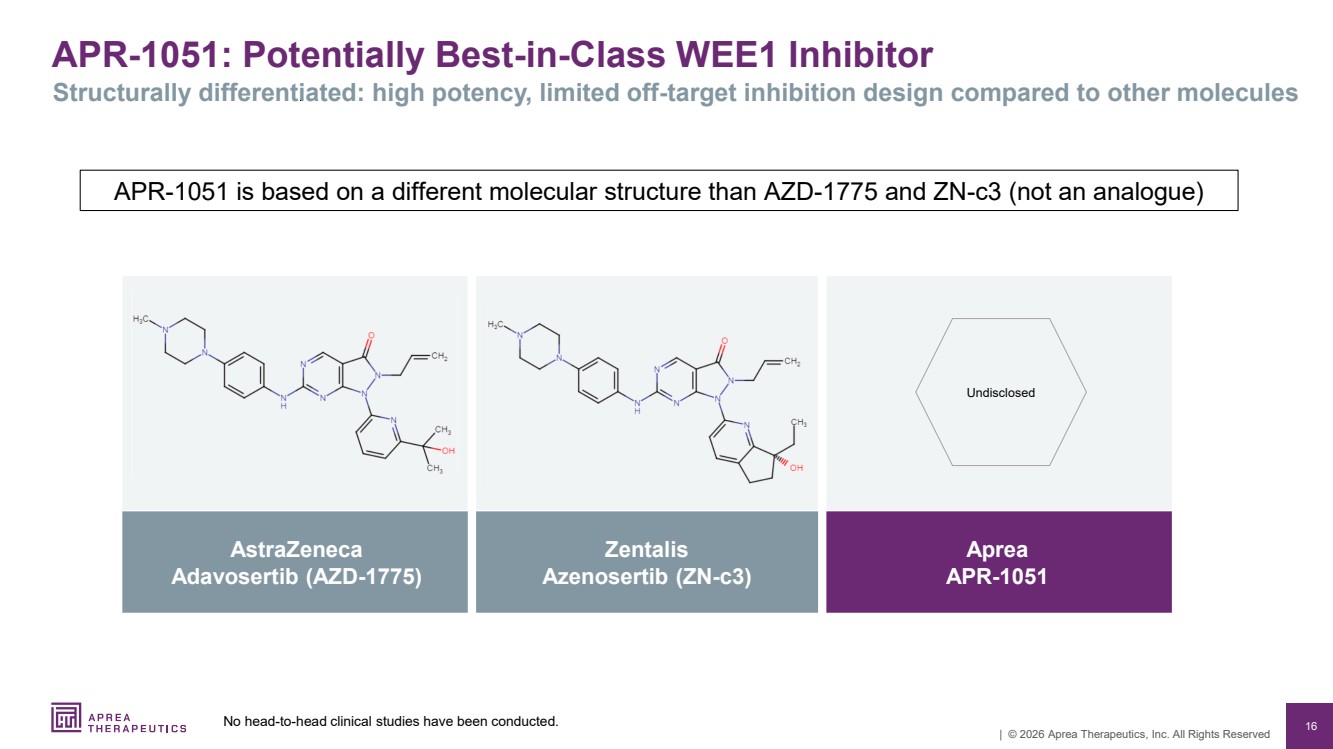
| 16 | © 2026 Aprea Therapeutics, Inc. All Rights Reserved APR-1051: Potentially Best-in-Class WEE1 Inhibitor Structurally differentiated: high potency, limited off-target inhibition design compared to other molecules AstraZeneca Adavosertib (AZD-1775) Zentalis Azenosertib (ZN-c3) Aprea APR-1051 Undisclosed APR-1051 is based on a different molecular structure than AZD-1775 and ZN-c3 (not an analogue) No head-to-head clinical studies have been conducted. |
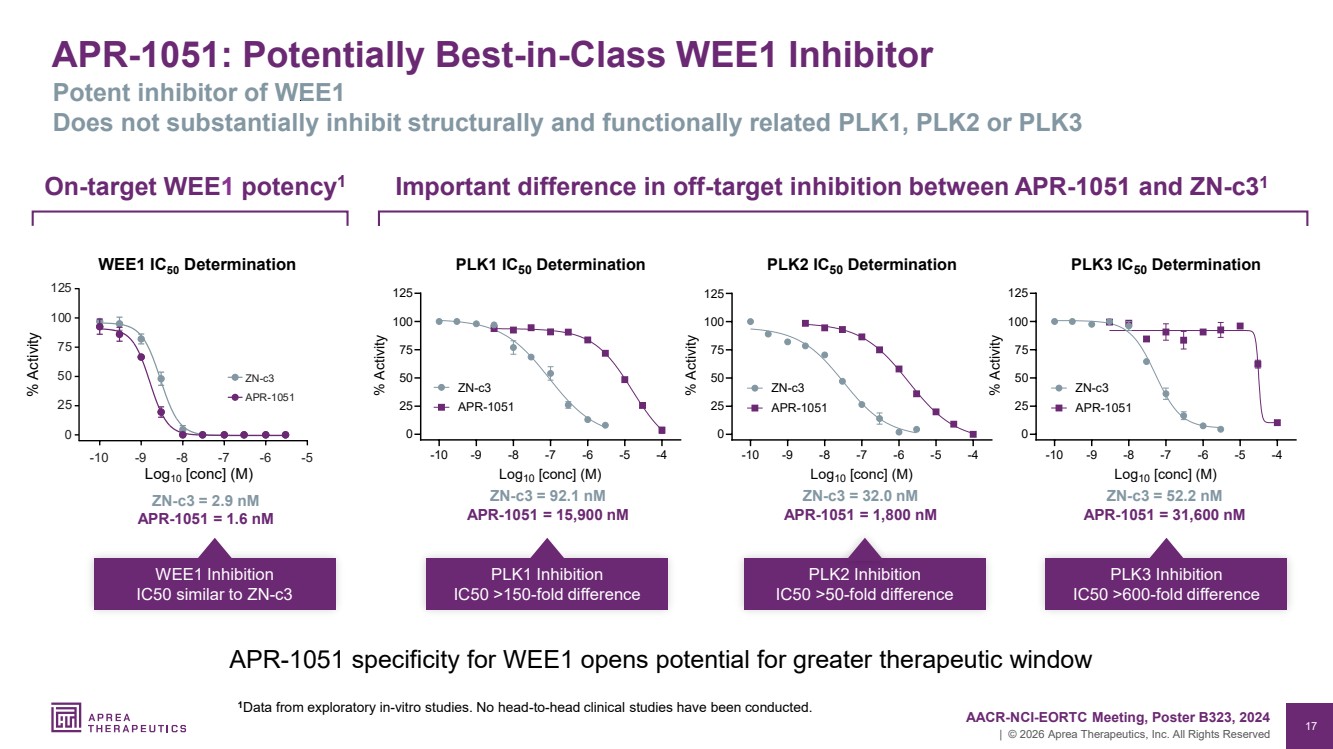
| 17 | © 2026 Aprea Therapeutics, Inc. All Rights Reserved APR-1051: Potentially Best-in-Class WEE1 Inhibitor Potent inhibitor of WEE1 Does not substantially inhibit structurally and functionally related PLK1, PLK2 or PLK3 -10 -9 -8 -7 -6 -5 -4 0 25 50 75 100 125 PLK1 IC50 Determination Log10 [conc] (M) % Activity ZN-c3 APR-1051 -10 -9 -8 -7 -6 -5 -4 0 25 50 75 100 125 PLK2 IC50 Determination Log10 [conc] (M) % Activity ZN-c3 APR-1051 -10 -9 -8 -7 -6 -5 -4 0 25 50 75 100 125 PLK3 IC50 Determination Log10 [conc] (M) % Activity ZN-c3 APR-1051 ZN-c3 = 92.1 nM APR-1051 = 15,900 nM PLK1 Inhibition IC50 >150-fold difference ZN-c3 = 32.0 nM APR-1051 = 1,800 nM PLK2 Inhibition IC50 >50-fold difference ZN-c3 = 52.2 nM APR-1051 = 31,600 nM PLK3 Inhibition IC50 >600-fold difference Important difference in off-target inhibition between APR-1051 and ZN-c3 On 1 -target WEE1 potency1 ZN-c3 = 2.9 nM APR-1051 = 1.6 nM WEE1 Inhibition IC50 similar to ZN-c3 125 100 75 50 25 0 10 9 8 7 6 5 APR 1051 c3 WEE1 IC50 Determination % Activity Log10 [conc] (M) AACR-NCI-EORTC Meeting, Poster B323, 2024 1Data from exploratory in-vitro studies. No head-to-head clinical studies have been conducted. APR-1051 specificity for WEE1 opens potential for greater therapeutic window |
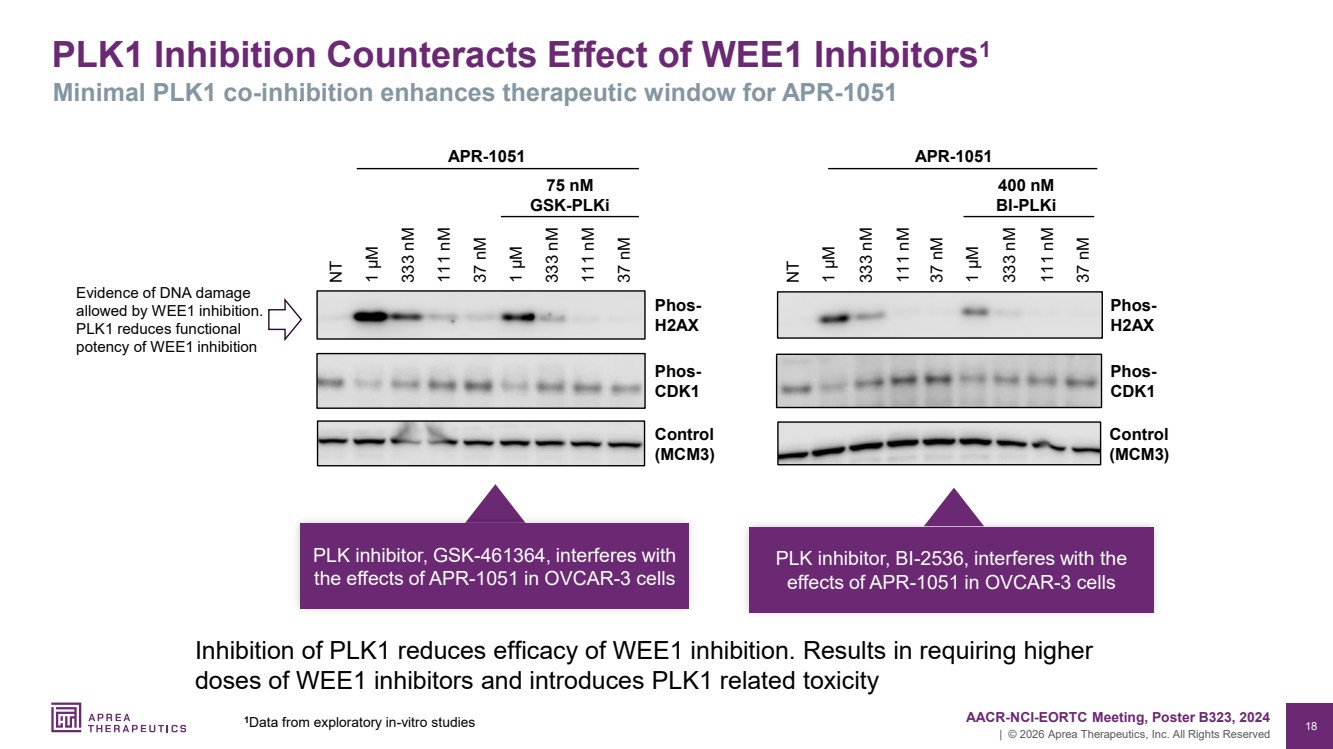
| 18 | © 2026 Aprea Therapeutics, Inc. All Rights Reserved PLK1 Inhibition Counteracts Effect of WEE1 Inhibitors1 Minimal PLK1 co-inhibition enhances therapeutic window for APR-1051 37 nM 111 nM 333 nM 1 µM 37 nM 111 nM 333 nM 1 µM Phos-H2AX Control (MCM3) NT Phos-CDK1 APR-1051 75 nM GSK-PLKi Control (MCM3) 37 nM 111 nM 333 nM 1 µM 37 nM 111 nM 333 nM NT 1 µM Phos-H2AX 400 nM BI-PLKi APR-1051 Phos-CDK1 PLK inhibitor, BI-2536, interferes with the effects of APR-1051 in OVCAR-3 cells 1 AACR-NCI-EORTC Meeting, Poster B323, 2024 Data from exploratory in-vitro studies Evidence of DNA damage allowed by WEE1 inhibition. PLK1 reduces functional potency of WEE1 inhibition PLK inhibitor, GSK-461364, interferes with the effects of APR-1051 in OVCAR-3 cells Inhibition of PLK1 reduces efficacy of WEE1 inhibition. Results in requiring higher doses of WEE1 inhibitors and introduces PLK1 related toxicity |
| 19 | © 2026 Aprea Therapeutics, Inc. All Rights Reserved Studies Show PLK1 Suppression is Associated with Sepsis-Induced Loss of Intestinal Barrier Function 1 PLK1 protects against sepsis-induced intestinal barrier dysfunction, Cao et al, Scientific Reports (2018). 2 PLK1 protects intestinal barrier function in sepsis: A translational research, Cao et al, Cytokine (2023). 3 PLK1 protects intestinal barrier function in sepsis: A translational research, Cao et al, Molecular Medicine (2022). 4 LncRNA DANCR improves the dysfunction of the intestinal barrier and alleviates epithelial injury by targeting the miR‐1306‐5p/PLK1 axis in sepsis, Wang et al., Cell Biology International (2021). |
| 20 | © 2026 Aprea Therapeutics, Inc. All Rights Reserved HPV+ Cancer – Collaboration with MD Anderson Ovarian Cancer* UMSCC47 tumor cells OVCAR3 tumor xenograft Tumor Volume (mm3 ) Vehicle Aprea ATRi 30 mg/kg QD Aprea WEE1i 30 mg/kg QD Combination – half dose, 15mg/kg each Days Post Treatment Tumor Volume (mm3 ) Days since start of xenograft mEER tumor cells Tumor Volume (mm3 ) Days since start of xenograft APR-1051 Demonstrated Preclinical Activity in Combination with Chemo, IO and ATRi Across Multiple Cancer Models * Data on file. Start of treatment 3 rea ed AP Cis a i C Start of treatment ** P<0.0001 * P=0.0067 ** ** * Chemotherapy Immuno-oncology DDR combination APR-1051 demonstrates synergistic potential preclinically with standard oncology agents |
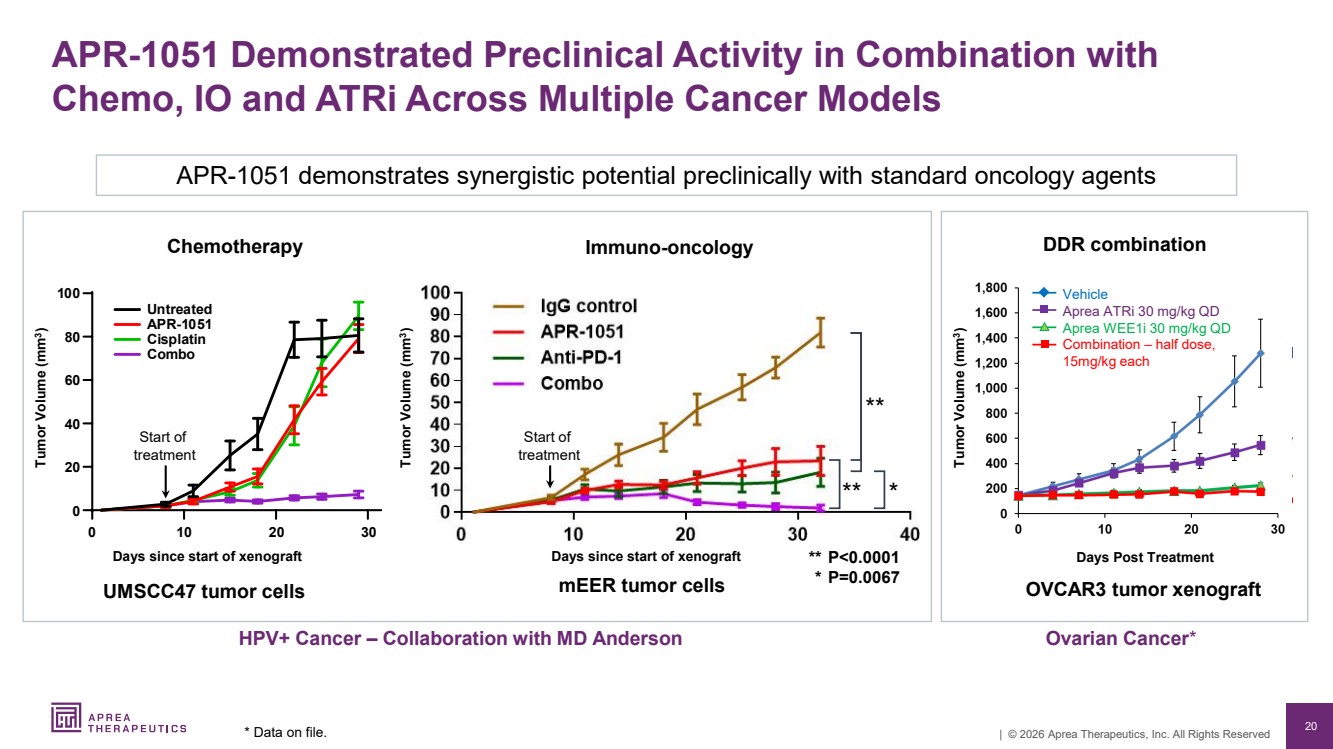
| 21 | © 2026 Aprea Therapeutics, Inc. All Rights Reserved APR-1051 WEE1 Summary First-in-class to translate validated biology into a scalable commercial asset 1 Clinically validated target • WEE1 inhibitors have shown promising activity in genomically defined tumors • Competitor programs constrained by low therapeutic window APR-1051 clinical highlights • Early clinical proof-of-concept at 150 mg and 220 mg dose levels • Two partial responses and six patients with stable disease to date • Potentially favorable safety profile at active dose levels • Clinical team strengthened to drive next development phase • Enrollment continues, additional clinical data expected this quarter APR-1051 preclinical differentiation and potentially best-in-class opportunity • Novel structure with high potency, limited off-target inhibition design • Minimal PLK1 inhibition enhances therapeutic window • Potential for synergy demonstrated in combination with standard oncology agents 2 3 |
| 22 | © 2026 Aprea Therapeutics, Inc. All Rights Reserved 22 Intellectual Property Portfolio Financial Summary & Capitalization Investment Highlights |

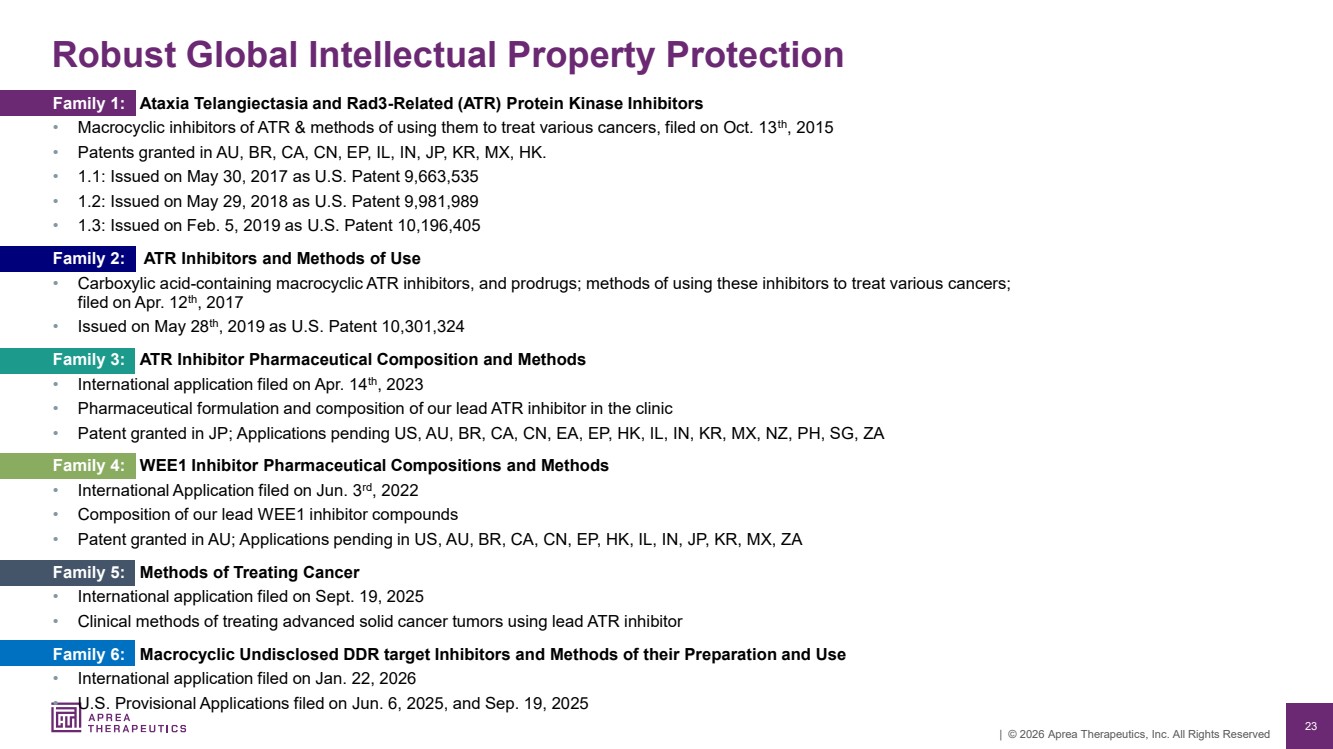
| 23 | © 2026 Aprea Therapeutics, Inc. All Rights Reserved Robust Global Intellectual Property Protection Family 1: Ataxia Telangiectasia and Rad3-Related (ATR) Protein Kinase Inhibitors • Macrocyclic inhibitors of ATR & methods of using them to treat various cancers, filed on Oct. 13th, 2015 • Patents granted in AU, BR, CA, CN, EP, IL, IN, JP, KR, MX, HK. • 1.1: Issued on May 30, 2017 as U.S. Patent 9,663,535 • 1.2: Issued on May 29, 2018 as U.S. Patent 9,981,989 • 1.3: Issued on Feb. 5, 2019 as U.S. Patent 10,196,405 Family 2: ATR Inhibitors and Methods of Use • Carboxylic acid-containing macrocyclic ATR inhibitors, and prodrugs; methods of using these inhibitors to treat various cancers; filed on Apr. 12th, 2017 • Issued on May 28th, 2019 as U.S. Patent 10,301,324 Family 3: ATR Inhibitor Pharmaceutical Composition and Methods • International application filed on Apr. 14th, 2023 • Pharmaceutical formulation and composition of our lead ATR inhibitor in the clinic • Patent granted in JP; Applications pending US, AU, BR, CA, CN, EA, EP, HK, IL, IN, KR, MX, NZ, PH, SG, ZA Family 4: WEE1 Inhibitor Pharmaceutical Compositions and Methods • International Application filed on Jun. 3rd, 2022 • Composition of our lead WEE1 inhibitor compounds • Patent granted in AU; Applications pending in US, AU, BR, CA, CN, EP, HK, IL, IN, JP, KR, MX, ZA Family 5: Methods of Treating Cancer • International application filed on Sept. 19, 2025 • Clinical methods of treating advanced solid cancer tumors using lead ATR inhibitor Family 6: Macrocyclic Undisclosed DDR target Inhibitors and Methods of their Preparation and Use • International application filed on Jan. 22, 2026 • U.S. Provisional Applications filed on Jun. 6, 2025, and Sep. 19, 2025 |
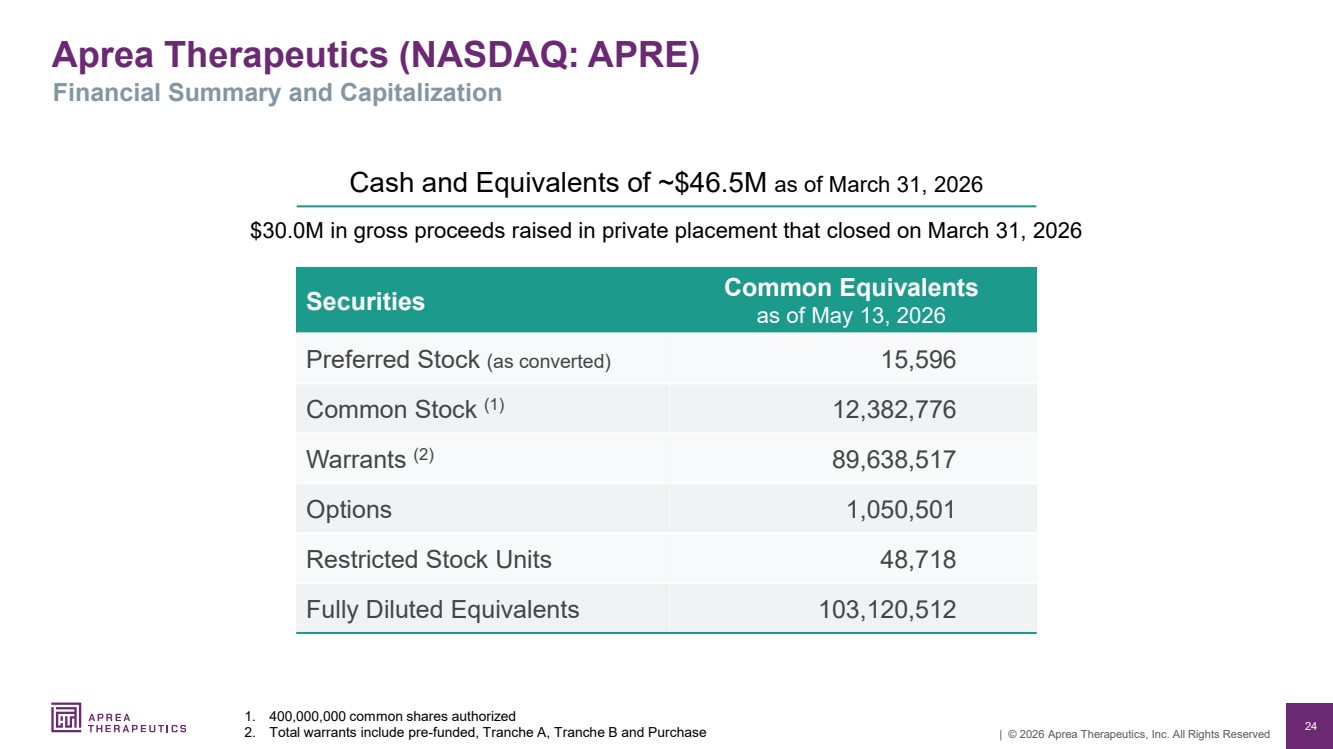
| 24 | © 2026 Aprea Therapeutics, Inc. All Rights Reserved Securities Common Equivalents as of May 13, 2026 Preferred Stock (as converted) 15,596 Common Stock (1) 12,382,776 Warrants (2) 89,638,517 Options 1,050,501 Restricted Stock Units 48,718 Fully Diluted Equivalents 103,120,512 Aprea Therapeutics (NASDAQ: APRE) 1. 400,000,000 common shares authorized 2. Total warrants include pre-funded, Tranche A, Tranche B and Purchase Cash and Equivalents of ~$46.5M as of March 31, 2026 $30.0M in gross proceeds raised in private placement that closed on March 31, 2026 Financial Summary and Capitalization |
| 25 | © 2026 Aprea Therapeutics, Inc. All Rights Reserved Expected cash runway into Q1 2028 • Achieve near term inflection points and catalysts • Evaluate optimal strategic partnerships Near term catalysts • APR-1051: Q2 2026 Safety/efficacy data; Q2 2027 Complete dose escalation • ATRN-119: October 2025 RP2D ✓ H2 2026 Potential collaborations on combinations Highly potent and selective design, potential best in class inhibitors, de-risked programs • Diversified portfolio including WEE1 (APR-1051) and ATR (ATRN-119) inhibitors • Early evidence of clinical activity including PRs (one confirmed) with APR-1051 • Single agent and combination potential therapies Technology developed by pioneers in synthetic lethality • Management with strong drug development and commercial expertise • Focused on addressing unmet needs for patients with biomarker defined cancers Investment Highlights |
| 26 | © 2026 Aprea Therapeutics, Inc. All Rights Reserved Aprea Therapeutics (NASDAQ: APRE) |