Exhibit 99.(e)
| NY xx/26 *xxxxx-26a1*25-2900 Page 1 of 10 All pages of this form must be returned. Print clearly in dark ink and avoid highlighting. 1. PRIMARY ANNUITANT Must be an individual. Check product guidelines for maximum issue age. First Name Middle Name Last Name Sex M F SSN Date of Birth (mm/dd/yyyy) Telephone Number E-mail Address Mailing Address Mailing City Mailing State Mailing Zip Code Resident Address (if different than mailing address) Resident City Resident State Resident Zip Code JOINT ANNUITANT (Optional) Not applicable for qualified contracts. Default is Joint unless this box is checked: Contingent First Name Middle Name Last Name Sex M F SSN Date of Birth (mm/dd/yyyy) Telephone Number E-mail Address Mailing Address Mailing City Mailing State Mailing Zip Code Resident Address (if different than mailing address) Resident City Resident State Resident Zip Code 2. OWNER If annuitant(s) and owner(s) are the same, do not complete this section. Check product guidelines for maximum issue age. First Name Middle Name Last Name Sex M F Entity (if an individual is not selected) SSN/TIN Date of Birth (mm/dd/yyyy) Telephone Number E-mail Address Mailing Address Mailing City Mailing State. Mailing Zip Code Resident Address (if different than mailing address) Resident City Resident State Resident Zip Code JOINT OWNER (Optional) Not applicable for qualified contracts. First Name Middle Name Last Name Sex M F Relationship to Owner SSN Date of Birth (mm/dd/yyyy) Telephone Number E-mail Address Mailing Address Mailing City Mailing State Mailing Zip Code Resident Address (if different than mailing address) Resident City Resident State Resident Zip Code Pacific Life & Annuity Company P.O. Box 2829, Omaha, NE 68103-2829 or 6750 Mercy Rd, Omaha, NE 68106 www.PacificLife.com (800) 748-6907 Pacific Protective Growth NY Individual Limited Premium Deferred Non-Guaranteed Index Annuity Contract Application NEW YORK |
| NY xx/26 *xxxx-26a2* 25-2900 Page 2 of 10 3. BENEFICIARIES If a beneficiary type is not indicated, the beneficiary will be considered a primary beneficiary. Primary and Contingent Beneficiary designations must equal 100% in total. If percentages are not provided, multiple beneficiaries will share the death benefit equally, unless otherwise specified. For contracts owned by a non-individual custodian (including IRAs, 403(b), Qualified plans) or other non-natural owners, do not complete the section below as the designated recipient will be the owner. For questions, please contact your tax and/or legal representative. If you are naming a minor as your beneficiary, please complete the [Special Beneficiary Designation Request] form. See your contract and prospectus for details about death benefit and beneficiary proceeds. 1. First Name Middle Name Last Name Relationship Entity (if an individual is not selected) SSN/TIN Date of Birth (mm/dd/yyyy) Primary Contingent Percentage % Mailing Address City State Zip Code Telephone Number 2. First Name Middle Name Last Name Relationship Entity (if an individual is not selected) SSN/TIN Date of Birth (mm/dd/yyyy) Primary Contingent Percentage % Mailing Address City State Zip Code Telephone Number 3. First Name Middle Name Last Name Relationship Entity (if an individual is not selected) SSN/TIN Date of Birth (mm/dd/yyyy) Primary Contingent Percentage % Mailing Address City State Zip Code Telephone Number 4. First Name Middle Name Last Name Relationship Entity (if an individual is not selected) SSN/TIN Date of Birth (mm/dd/yyyy) Primary Contingent Percentage % Mailing Address City State Zip Code Telephone Number 5. First Name Middle Name Last Name Relationship Entity (if an individual is not selected) SSN/TIN Date of Birth (mm/dd/yyyy) Primary Contingent Percentage % Mailing Address City State Zip Code Telephone Number 6. First Name Middle Name Last Name Relationship Entity (if an individual is not selected) SSN/TIN Date of Birth (mm/dd/yyyy) Primary Contingent Percentage % Mailing Address City State Zip Code Telephone Number |
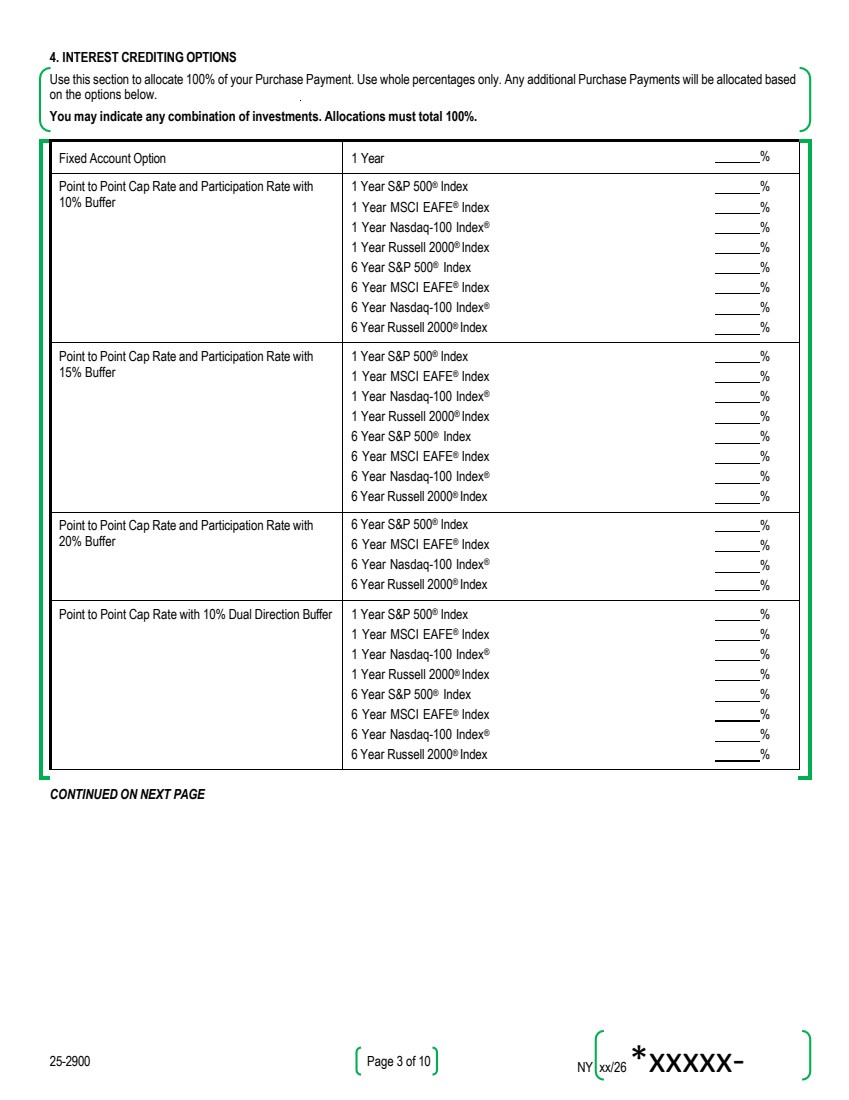
| NY xx/26*xxxxx-26A3* 25-2900 Page 3 of 10 4. INTEREST CREDITING OPTIONS Use this section to allocate 100% of your Purchase Payment. Use whole percentages only. Any additional Purchase Payments will be allocated based on the options below. You may indicate any combination of investments. Allocations must total 100%. Fixed Account Option 1 Year % Point to Point Cap Rate and Participation Rate with 10% Buffer 1 Year S&P 500® Index 1 Year MSCI EAFE® Index 1 Year Nasdaq-100 Index® 1 Year Russell 2000® Index 6 Year S&P 500® Index 6 Year MSCI EAFE® Index 6 Year Nasdaq-100 Index® 6 Year Russell 2000® Index % % % % % % % % Point to Point Cap Rate and Participation Rate with 15% Buffer 1 Year S&P 500® Index 1 Year MSCI EAFE® Index 1 Year Nasdaq-100 Index® 1 Year Russell 2000® Index 6 Year S&P 500® Index 6 Year MSCI EAFE® Index 6 Year Nasdaq-100 Index® 6 Year Russell 2000® Index % % % % % % % % Point to Point Cap Rate and Participation Rate with 20% Buffer 6 Year S&P 500® Index 6 Year MSCI EAFE® Index 6 Year Nasdaq-100 Index® 6 Year Russell 2000® Index % % % % Point to Point Cap Rate with 10% Dual Direction Buffer 1 Year S&P 500® Index 1 Year MSCI EAFE® Index 1 Year Nasdaq-100 Index® 1 Year Russell 2000® Index 6 Year S&P 500® Index 6 Year MSCI EAFE® Index 6 Year Nasdaq-100 Index® 6 Year Russell 2000® Index % % % % % % % % CONTINUED ON NEXT PAGE |
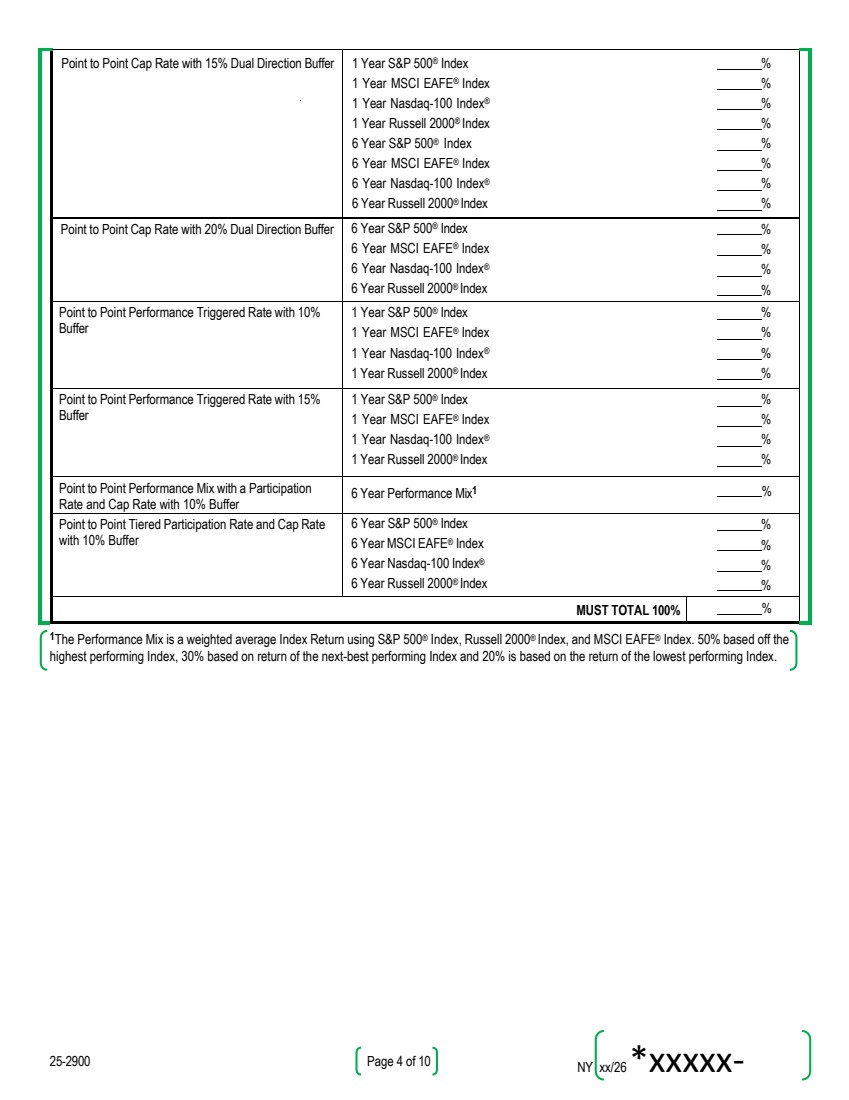
| NY xx/26*xxxxx-26A4* 25-2900 Page 4 of 10 Point to Point Cap Rate with 15% Dual Direction Buffer 1 Year S&P 500® Index 1 Year MSCI EAFE® Index 1 Year Nasdaq-100 Index® 1 Year Russell 2000® Index 6 Year S&P 500® Index 6 Year MSCI EAFE® Index 6 Year Nasdaq-100 Index® 6 Year Russell 2000® Index % % % % % % % % Point to Point Cap Rate with 20% Dual Direction Buffer 6 Year S&P 500® Index 6 Year MSCI EAFE® Index 6 Year Nasdaq-100 Index® 6 Year Russell 2000® Index % % % % Point to Point Performance Triggered Rate with 10% Buffer 1 Year S&P 500® Index 1 Year MSCI EAFE® Index 1 Year Nasdaq-100 Index® 1 Year Russell 2000® Index % % % % Point to Point Performance Triggered Rate with 15% Buffer 1 Year S&P 500® Index 1 Year MSCI EAFE® Index 1 Year Nasdaq-100 Index® 1 Year Russell 2000® Index % % % % Point to Point Performance Mix with a Participation Rate and Cap Rate with 10% Buffer 6 Year Performance Mix1 % Point to Point Tiered Participation Rate and Cap Rate with 10% Buffer 6 Year S&P 500® Index 6 Year MSCI EAFE® Index 6 Year Nasdaq-100 Index® 6 Year Russell 2000® Index % % % % MUST TOTAL 100% % 1The Performance Mix is a weighted average Index Return using S&P 500® Index, Russell 2000® Index, and MSCI EAFE® Index. 50% based off the highest performing Index, 30% based on return of the next-best performing Index and 20% is based on the return of the lowest performing Index. |
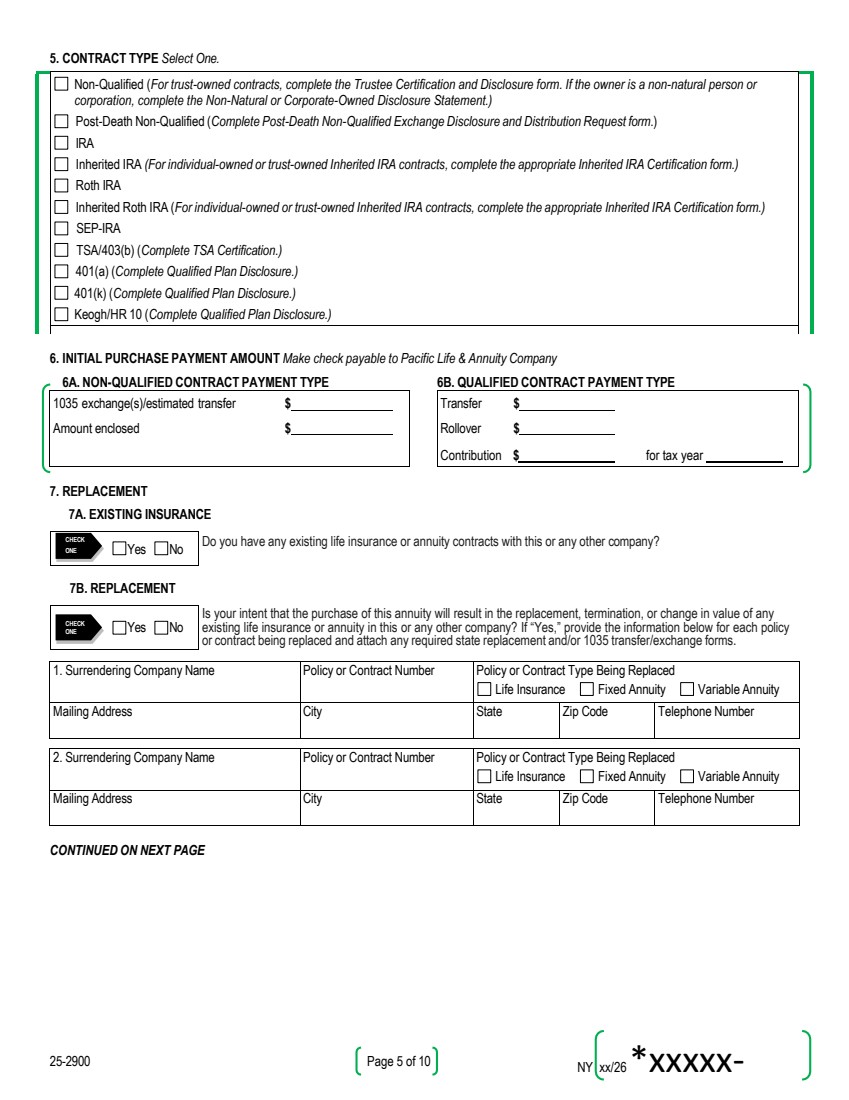
| NY xx/26*xxxxx-26A5* 25-2900 Page 5 of 10 5. CONTRACT TYPE Select One. Non-Qualified (For trust-owned contracts, complete the Trustee Certification and Disclosure form. If the owner is a non-natural person or corporation, complete the Non-Natural or Corporate-Owned Disclosure Statement.) Post-Death Non-Qualified (Complete Post-Death Non-Qualified Exchange Disclosure and Distribution Request form.) IRA Inherited IRA (For individual-owned or trust-owned Inherited IRA contracts, complete the appropriate Inherited IRA Certification form.) Roth IRA Inherited Roth IRA (For individual-owned or trust-owned Inherited IRA contracts, complete the appropriate Inherited IRA Certification form.) SEP-IRA TSA/403(b) (Complete TSA Certification.) 401(a) (Complete Qualified Plan Disclosure.) 401(k) (Complete Qualified Plan Disclosure.) Keogh/HR 10 (Complete Qualified Plan Disclosure.) 6. INITIAL PURCHASE PAYMENT AMOUNT Make check payable to Pacific Life & Annuity Company 6A. NON-QUALIFIED CONTRACT PAYMENT TYPE 6B. QUALIFIED CONTRACT PAYMENT TYPE 1035 exchange(s)/estimated transfer $ Transfer $ Amount enclosed $ Rollover $ Contribution $ for tax year 7. REPLACEMENT 7A. EXISTING INSURANCE CHECK ONE Yes No Do you have any existing life insurance or annuity contracts with this or any other company? 7B. REPLACEMENT CHECK ONE Yes No Is your intent that the purchase of this annuity will result in the replacement, termination, or change in value of any existing life insurance or annuity in this or any other company? If “Yes,” provide the information below for each policy or contract being replaced and attach any required state replacement and/or 1035 transfer/exchange forms. 1. Surrendering Company Name Policy or Contract Number Policy or Contract Type Being Replaced Life Insurance Fixed Annuity Variable Annuity Mailing Address City State Zip Code Telephone Number 2. Surrendering Company Name Policy or Contract Number Policy or Contract Type Being Replaced Life Insurance Fixed Annuity Variable Annuity Mailing Address City State Zip Code Telephone Number CONTINUED ON NEXT PAGE |
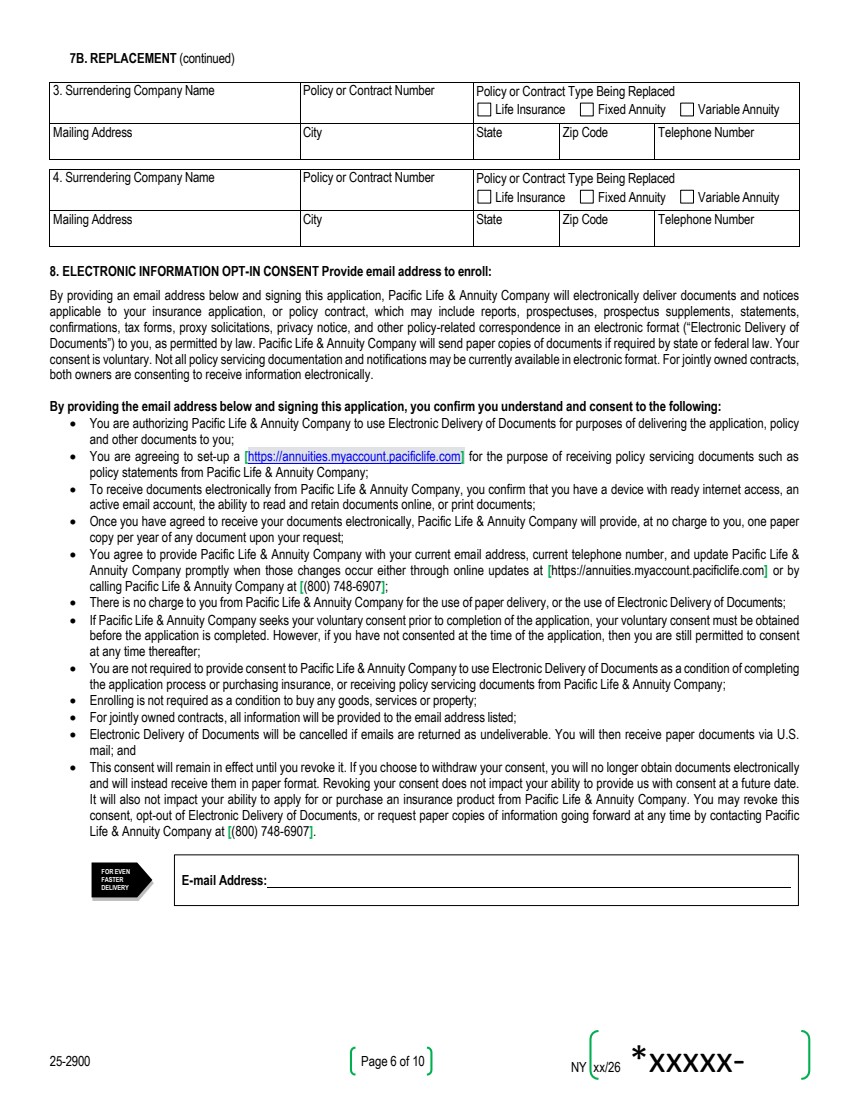
| NY xx/26 *xxxxx-26a6* 25-2900 Page 6 of 10 FOR EVEN FASTER DELIVERY E-mail Address: 7B. REPLACEMENT (continued) 3. Surrendering Company Name Policy or Contract Number Policy or Contract Type Being Replaced Life Insurance Fixed Annuity Variable Annuity Mailing Address City State Zip Code Telephone Number 4. Surrendering Company Name Policy or Contract Number Policy or Contract Type Being Replaced Life Insurance Fixed Annuity Variable Annuity Mailing Address City State Zip Code Telephone Number 8. ELECTRONIC INFORMATION OPT-IN CONSENT Provide email address to enroll: By providing an email address below and signing this application, Pacific Life & Annuity Company will electronically deliver documents and notices applicable to your insurance application, or policy contract, which may include reports, prospectuses, prospectus supplements, statements, confirmations, tax forms, proxy solicitations, privacy notice, and other policy-related correspondence in an electronic format (“Electronic Delivery of Documents”) to you, as permitted by law. Pacific Life & Annuity Company will send paper copies of documents if required by state or federal law. Your consent is voluntary. Not all policy servicing documentation and notifications may be currently available in electronic format. For jointly owned contracts, both owners are consenting to receive information electronically. By providing the email address below and signing this application, you confirm you understand and consent to the following: • You are authorizing Pacific Life & Annuity Company to use Electronic Delivery of Documents for purposes of delivering the application, policy and other documents to you; • You are agreeing to set-up a [https://annuities.myaccount.pacificlife.com] for the purpose of receiving policy servicing documents such as policy statements from Pacific Life & Annuity Company; • To receive documents electronically from Pacific Life & Annuity Company, you confirm that you have a device with ready internet access, an active email account, the ability to read and retain documents online, or print documents; • Once you have agreed to receive your documents electronically, Pacific Life & Annuity Company will provide, at no charge to you, one paper copy per year of any document upon your request; • You agree to provide Pacific Life & Annuity Company with your current email address, current telephone number, and update Pacific Life & Annuity Company promptly when those changes occur either through online updates at [https://annuities.myaccount.pacificlife.com] or by calling Pacific Life & Annuity Company at [(800) 748-6907]; • There is no charge to you from Pacific Life & Annuity Company for the use of paper delivery, or the use of Electronic Delivery of Documents; • If Pacific Life & Annuity Company seeks your voluntary consent prior to completion of the application, your voluntary consent must be obtained before the application is completed. However, if you have not consented at the time of the application, then you are still permitted to consent at any time thereafter; • You are not required to provide consent to Pacific Life & Annuity Company to use Electronic Delivery of Documents as a condition of completing the application process or purchasing insurance, or receiving policy servicing documents from Pacific Life & Annuity Company; • Enrolling is not required as a condition to buy any goods, services or property; • For jointly owned contracts, all information will be provided to the email address listed; • Electronic Delivery of Documents will be cancelled if emails are returned as undeliverable. You will then receive paper documents via U.S. mail; and • This consent will remain in effect until you revoke it. If you choose to withdraw your consent, you will no longer obtain documents electronically and will instead receive them in paper format. Revoking your consent does not impact your ability to provide us with consent at a future date. It will also not impact your ability to apply for or purchase an insurance product from Pacific Life & Annuity Company. You may revoke this consent, opt-out of Electronic Delivery of Documents, or request paper copies of information going forward at any time by contacting Pacific Life & Annuity Company at [(800) 748-6907]. |
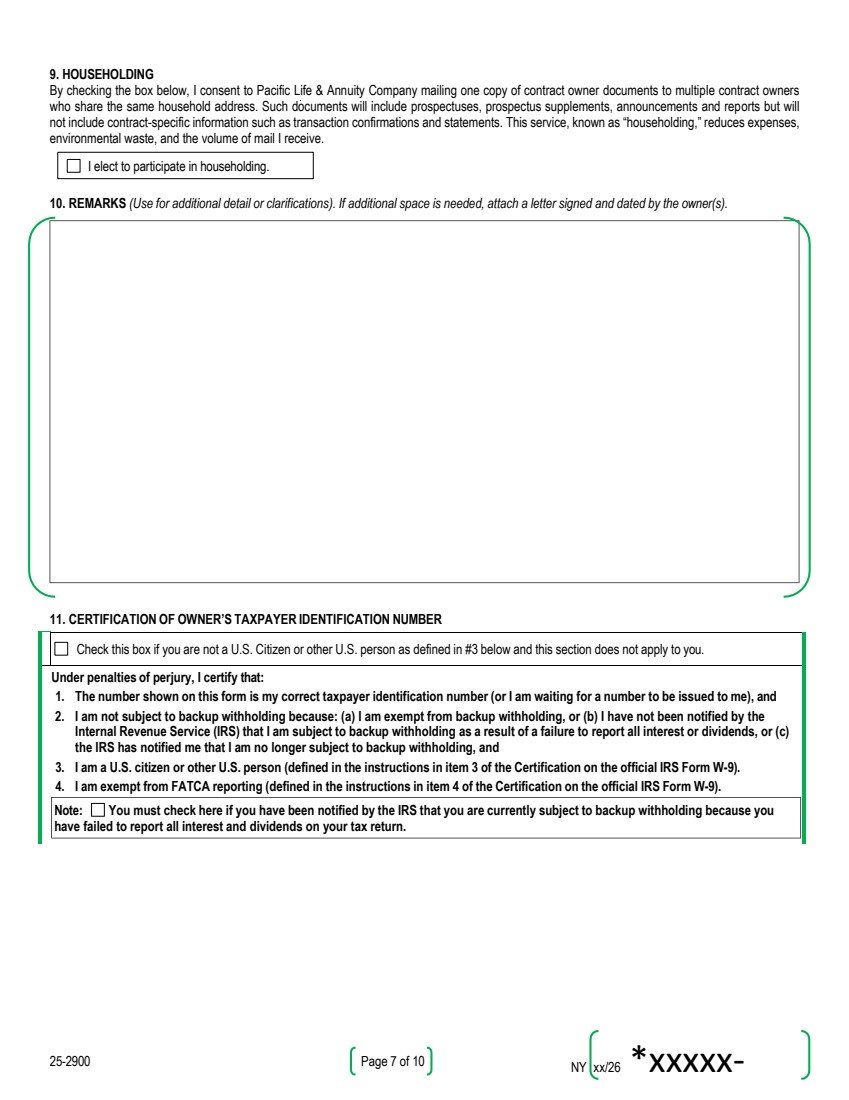
| NY xx/26 *xxxxx-26a7* 25-2900 Page 7 of 10 I elect to participate in householding. 9. HOUSEHOLDING By checking the box below, I consent to Pacific Life & Annuity Company mailing one copy of contract owner documents to multiple contract owners who share the same household address. Such documents will include prospectuses, prospectus supplements, announcements and reports but will not include contract-specific information such as transaction confirmations and statements. This service, known as “householding,” reduces expenses, environmental waste, and the volume of mail I receive. 10. REMARKS (Use for additional detail or clarifications). If additional space is needed, attach a letter signed and dated by the owner(s). 11. CERTIFICATION OF OWNER’S TAXPAYER IDENTIFICATION NUMBER Check this box if you are not a U.S. Citizen or other U.S. person as defined in #3 below and this section does not apply to you. Under penalties of perjury, I certify that: 1. The number shown on this form is my correct taxpayer identification number (or I am waiting for a number to be issued to me), and 2. I am not subject to backup withholding because: (a) I am exempt from backup withholding, or (b) I have not been notified by the Internal Revenue Service (IRS) that I am subject to backup withholding as a result of a failure to report all interest or dividends, or (c) the IRS has notified me that I am no longer subject to backup withholding, and 3. I am a U.S. citizen or other U.S. person (defined in the instructions in item 3 of the Certification on the official IRS Form W-9). 4. I am exempt from FATCA reporting (defined in the instructions in item 4 of the Certification on the official IRS Form W-9). Note: You must check here if you have been notified by the IRS that you are currently subject to backup withholding because you have failed to report all interest and dividends on your tax return. |
| NY xx/26 *xxxxx-26a8* 25-2900 Page 8 of 10 12. STATEMENT OF OWNER(S) 1. I/We, the owner(s), understand that I/we have applied for a deferred annuity contract (“contract”) issued by Pacific Life & Annuity Company (“company”). 2. I/We received the annuity prospectus, product disclosure (“Contract Summary”), and if applicable, the Buyer’s Guide for Deferred Annuities for this annuity contract. 3. I/We have discussed all fees and charges for this contract with my/our Financial Professional, including withdrawal charges. I/We understand all fees and charges for this contract. 4. I/We understand that if I/we cancel a contract issued as a result of this application, without penalty during the Right to Cancel initial review period, it is possible the amount refunded may be less than the initial amount I/we invested due to the investment experience of my/our selected interest crediting options. 5. I/We understand this contract will not become effective unless it is issued while the Owner(s) and Annuitant(s) are living. 6. I/We understand this application is to be attached to and made part of the contract. I/WE UNDERSTAND THAT AMOUNTS ALLOCATED TO THE FIXED ACCOUNT OPTION EARN INTEREST NOT LESS THAN THE MINIMUM GUARANTEED INTEREST RATE STATED IN THE CONTRACT SPECIFICATIONS. I/WE UNDERSTAND THAT WHILE THE VALUES OF THE CONTRACT MAY BE AFFECTED BY AN EXTERNAL INDEX, THE CONTRACT DOES NOT DIRECTLY PARTICIPATE IN ANY STOCK OR EQUITY INVESTMENT. I/WE UNDERSTAND THAT VALUES PROVIDED UNDER THE INDEX-LINKED OPTIONS MAY BE POSITIVE, NEGATIVE, OR ZERO. AMOUNTS DIRECTED INTO INDEX-LINKED OPTIONS WILL BE BASED ON THE INVESTMENT EXPERIENCE OF THE APPLICABLE INDEX. ANY POSITIVE INDEX RETURNS ARE LIMITED BY THE CREDITING STRATEGY AND NEGATIVE RETURNS ARE LIMITED BY THE PROTECTION LEVELS APPLIED TO SUCH INDEX-LINKED OPTIONS. THESE AMOUNTS MAY INCREASE OR DECREASE AND ARE NOT GUARANTEED AS TO DOLLAR AMOUNT. CREDITING STRATEGIES AND PROTECTION LEVELS ONLY APPLY AT THE END OF EACH TERM. FURTHER, ANY WITHDRAWALS OR DISTRIBUTIONS TAKEN BEFORE THE END OF A TERM WILL BE SUBJECT TO AN INTERIM VALUE ADJUSTMENT. All answers to questions and statements made on this application are true and complete to the best of my knowledge and belief. THE INTERNAL REVENUE SERVICE DOES NOT REQUIRE YOUR CONSENT TO ANY PROVISION OF THIS DOCUMENT OTHER THAN THE CERTIFICATIONS REQUIRED TO AVOID BACKUP WITHHOLDING. Owner’s Signature Owner’s Signature Date (mm/dd/yyyy) Joint Owner’s Signature Joint Owner’s Signature (if applicable) Date (mm/dd/yyyy) Signed at: City State State Solicited: Complete this box for custodial-owned qualified contracts only. Will not be valid for any other contract types. Information put here will be used for contract and Financial Professional appointment purposes. SIGN HERE SIGN HERE |
| NY xx/26 *xxxxx-26a9* 25-2900 Page 9 of 10 13. FINANCIAL PROFESSIONAL’S STATEMENT 13A. EXISTING INSURANCE CHECK ONE Yes No Do you have any reason to believe that the applicant has any existing life insurance policies or annuity contracts? 13B. REPLACEMENT CHECK ONE Yes No Do you have reason to believe that any existing life insurance policy or annuity contract has been (or will be) surrendered, withdrawn from, loaned against, changed, or otherwise reduced in value, or replaced in connection with this transaction assuming the contract applied for will be issued? If “Yes,” I affirm that I have referred the applicant to the replacement question in Section 7B of this application. 1. I hereby certify that I have used only Pacific Life & Annuity Company’s approved sales material in connection with this sale and that copies of all sales materials used were left with the applicant(s). Any insurer-approved electronically presented sales materials will be provided in printed form to the applicant(s) no later than at the time of the contract or contract delivery. I further certify that I have discussed the appropriateness of replacement and followed Pacific Life & Annuity Company’s written replacement guidelines. I have explained to the owner(s) how the annuity will meet their insurable needs and financial objectives. 2. I certify that I have provided the applicant(s) with the annuity prospectus, a product disclosure (“Contract Summary”), and if applicable, a Buyer’s Guide for Deferred Annuities for this annuity contract. I have explained to the owner(s) how the annuity will meet their insurable needs and financial objectives. 3. I certify that I have reviewed this application and have determined that its proposed purchase is suitable as required under applicable law(s), based in part on information provided by the owner(s), as applicable, including age, income, net worth, tax status, and any existing investments and insurance program. I further certify that I have also considered the owner’s liquidity needs, financial resources used to fund the annuity (including debts and obligations), willingness to accept any non-guaranteed elements, risk tolerance, and time horizon; that I followed my broker/dealer’s suitability guidelines in both the recommendation of this annuity and the choice of fixed and index terms; and that this application is subject to review for suitability by my broker/dealer. 4. I further certify that the recommended purchase is in the best interest of the owner(s), that I have followed the standards and obligations required under law in making that best interest determination, and that I did not place my own or Pacific Life & Annuity Company’s financial interests ahead of the interests of the owner(s). I further certify that I have truly and accurately recorded on the application the information provided to me by the applicant(s). 5. If the applicant(s) is an active-duty member of the United States Armed Forces (including active-duty military reserve personnel), I certify that this application was not solicited and/or signed on a military base or installation, and I provided to the applicant(s) the disclosure required by Section 10 of the Military Personnel Financial Services Protection Act. I further certify that, prior to soliciting the contract applied for, I have completed all state mandated annuity, insurance, and/or product training and agree to provide documentation of such completion upon request by Pacific Life & Annuity Company. I have provided a Pacific Life & Annuity Company approved annuity illustration to the applicant in connection with this application. CONTINUED ON NEXT PAGE |
| NY xx/26 *xxxxx-26a10* 25-2900 Page 10 of 10 13. FINANCIAL PROFESSIONAL’S STATEMENT (continued) First Soliciting Financial Professional’s Signature Print First Financial Professional’s Full Name First Financial Professional’s Telephone Number First Financial Professional’s Email Address First Broker/Dealer’s Name (if applicable) First Brokerage Account Number (optional) First Distribution Firm’s Name (if applicable) First Option A B C D E First ID # (if applicable) Commission % (Default will be 100% if one Financial Professional is listed) Second Soliciting Financial Professional’s Signature Print Second Financial Professional’s Full Name Second Financial Professional’s Telephone Number Second Financial Professional’s Email Address Second Broker/Dealer’s Name (if applicable) Second Brokerage Account Number (optional) Second Distribution Firm’s Name (if applicable) Second Option Option will be the same as selected above. Second ID # (if applicable) Commission % (Commission will be equally split unless otherwise specified) Send completed application as follows: APPLICATION WITH PAYMENT: APPLICATION WITHOUT PAYMENT: Regular Mail Delivery: P.O. Box 2736 Omaha, NE 68103-2736 Regular Mail Delivery: P.O. Box 2829 Omaha, NE 68103-2829 Email: AnnuityService@PacificLife.com Fax: (888) 837-8172 Online Upload: Financial Professionals can log in to annuities.pacificlife.com Overnight Mail Delivery: 6750 Mercy Rd Omaha, NE 68106 Overnight Mail Delivery: 6750 Mercy Rd Omaha, NE 68106 Questions: (800) 748-6907 SIGN HERE Soliciting Financial Professional’s Signature SIGN HERE Soliciting Financial Professional’s Signature (if applicable) |